


Introduction and context
The UK is an ethnically rich and diverse country. However, the North East of England is a region with one of the lowest foreign-born populations (ONS, 2010). In the context of delivering psychological therapy (CBT) cross-culturally, there are many considerations that are helpful, for example, the impact of migration and absence of historical clinical records, theories of acculturation and the impact of religion. Although these issues are all highly relevant, this paper will focus specifically on the use of an interpreter.
Guidance recommends that staff reflect the ethnic make-up of the local population and it is hoped that this gives clients the opportunity to see a therapist from the same community or faith group as themselves (DoH/IAPT, 2009). The guidance naturally focuses on areas where services frequently use interpreters; however, it does not inform a less diverse staff group on how to overcome barriers to working with people who do not speak English. This is further impacted by lower numbers of non-English-speaking people in some pockets of the North East giving staff less opportunity to gain experience in working with interpreters.
Differences between culture and language have been discussed previously (Ahmer et al. Reference Ahmer, Faruqui and Aijaz2007) and it is argued here that overcoming language barriers more effectively would allow cultural issues to become more accessible and better integrated into therapy. It has been highlighted that how the individual relates to their community and cultural group may be of significance to their formulation (Levinson, Reference Levinson, Dryden and Branch2012). Levinson outlines the key difficulties of universalist services with ‘standard ideas’ (p. 163) adapting practice to fit diverse individual needs, and also notes that diverging away from empirically supported treatment plans means that they are no longer empirically supported.
It is clearly important to take into account ethnicity, culture and faith, and Grant et al. (Reference Grant, Townend, Mills and Cockx2008) provide a helpful summary about how culture and religion can be incorporated into the therapeutic process when working with clients (see Recommended Reading section for further information on culture and formulation). Language is the vehicle through which this can be achieved, and therefore appears to be the simplest and most important part of the process to get right. However, although there is literature supporting the delivery of CBT through interpreters to people experiencing trauma-related symptoms (Hinton & Otto, Reference Hinton and Otto2006; d'Ardenne et al. Reference d'Ardenne, Farmer, Ruaro and Priebe2007a, b) there is a paucity of written information about using interpreters in CBT for common mental health problems such as anxiety and depression. Due to this lack of literature on the subject, a literature search was performed using The Cumulative Index to Nursing and Allied Health Literature (CINAHL) database as it incorporates PsychARTICLES, Psychology and Behavioural Sciences Collection and PsycINFO. The search generated limited CBT-specific information which suggests a difficulty for therapists using interpreters and complying with National Institute for Clinical Excellence (NICE) and Improving Access to Psychological Therapies (IAPT) guidelines effectively.
Despite the sparse literature, Westermyer (Reference Westermyer1990) described two models of interpreting; the ‘triangle model’ and the ‘black box model’. The triangle model is where the interpreter is fully involved in the therapeutic relationship and conveys the message of what the client is saying in a more interpretive rather than literal way. In support of this, Costa (Reference Costa2010) noted that the interpreter should be treated as an ‘equal and integral component of the dynamic’ rather than simply an addition. While this model allows for cultural nuances to be emphasized or explained, it makes the therapeutic relationship more complex by more fully incorporating a third person. The black box model treats the interpreter as a literal translator and although this minimizes complicated transference issues, it can exclude a vital resource for the therapist and be demeaning for the interpreter.
To put the above into context, we will consider the case of Dalia, whose therapist adopted the triangle model of interpreting, the implications for which will be discussed in the following sections. Clarification and guidance on interpreting models can be found in ‘Guidelines for Psychologists’ (Tribe & Thompson, Reference Tribe and Thompson2008). The case of Dalia provides the opportunity for reflection on this specific case but also suggests the need for research on the use of interpreters generally. It is worth noting that the author was a trainee at the time of working with this client, but it is felt that the points made are relevant to both trainees and qualified therapists. Dalia gave consent for this report to be written. A pseudonym has been used and some detail has been made more generic to protect her identity.
Case history and presenting problems
Dalia was a 35-year-old woman who moved to the North East of England from the Middle East approximately 1 year prior to treatment. She was referred to the IAPT service by her GP who suspected that she was experiencing depression. In her first two sessions Dalia described feeling very isolated, low in mood and greatly missing her family. She was also deeply concerned that this problem indicated something strange about her that made her different to other people. It transpired that she had a phobia of many different types of animals and linked to this were several traumatic experiences in her childhood. While the experiences were predominantly associated with chickens her family owned and cats that lived nearby, her anxiety had spread to other animals over the years. The IAPT minimum dataset was collected at each session. At the beginning of treatment Dalia's highest Patient Health Questionnaire (PHQ-9; Kroenke et al. Reference Kroenke, Spitzer and Williams2001) score was 19, and her score for phobia question 3 was 8. It is unclear whether these scores are an appropriate measure of Dalia's problems given her cultural background.
Formulation
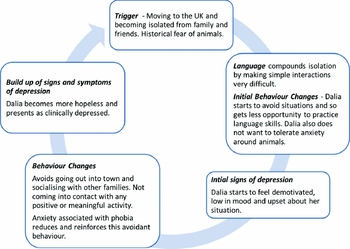
On moving to the UK from the Middle East Dalia had experienced a marked increase in both linguistic and social isolation. Initially Dalia made good efforts to find other Middle Eastern families to integrate with as well attending English-language classes; however, these efforts waned as she became depressed and felt more hopeless about her situation. Dalia was phobic of various animals and was avoiding any potential contact with them. She found it very difficult to understand why people would keep pets and she attributed this to cultural differences. Dalia's phobia of animals was compounding the problem and increasing her avoidant behaviour. It was hypothesized that this episode of depression was triggered by her sudden isolation and difficulty engaging in rewarding experiences. She then began to experience feelings of hopelessness and started to use avoidance as a strategy, which consequently was reinforced by a decrease in the anxiety associated with animals. This is represented as a formulation diagram (see Fig. 1).

Fig. 1. Adapted from Behavioural Activation for Depression (Martell et al. Reference Martell, Dimidjian and Herman-Dunn2010). Reprinted with permission of The Guilford Press.
Interventions
Since communication with services so far had been via her husband, the first intervention was for communication to be facilitated in a way that was appropriate to Dalia. Despite there being a limited choice of interpreters, by good fortune a female interpreter (which Dalia requested) who was from the same part of the Middle East, and who was approximately the same age was available.
The ‘Guidelines for Psychologists’ (Tribe & Thompson, Reference Tribe and Thompson2008) suggests that if the client is from a small community the risk of them knowing the interpreter is greater causing potential confidentiality issues. As Dalia had only recently moved to the area and the interpreter was travelling from a different part of the region, there was some significant geographical and social distance between them. This seemed appropriate for all parties and Dalia stated to feel comfortable using this interpreter.
Evidence shows that behavioural activation is a simple and effective treatment for depression (Ekers et al. Reference Ekers, Richards and Gilbody2008) and also lends itself easily to incorporating an exposure plan. Activity monitoring and scheduling were undertaken and a shared language was gradually developed to complete the diary sheets. Initially Dalia completed them in Arabic but then as standard terms were developed to describe specific activities, she used these English words to complete the monitoring sheet. This approach also fitted with her goal of trying to improve her English-language skills.
Once a pattern of scheduled activities was established the theory of habituation was explained to Dalia in order to give her a clear rationale for exposure. A graph depicting the rise and fall of anxiety while engaged in avoidant behaviour was drawn which was then contrasted to a graph depicting habituation to anxiety over a period of time through exposure. This pictorial method was useful in enhancing meaning as well as reducing the risk of the theory becoming lost in translation.
Once Dalia understood the rationale the exposure hierarchy was developed. At first this involved visiting a local pet shop and staying within close proximity to the cages until Dalia's anxiety reduced. These tasks progressed until Dalia was able to handle a hamster in session with the therapist. Although Dalia's phobia was not animal specific, a hamster was used due to its availability. Dalia began to use the techniques learned in session while out in public, for example, not crossing the road when she saw a dog. As the phobic anxiety reduced Dalia was able to schedule in more activities which reduced her isolation and boredom which in turn impacted positively on her mood. Time was also spent exploring different cultural approaches to keeping pets, for example Dalia discussed how in her culture animals were kept purely for functional reasons such as producing eggs or milk. This information enhanced the formulation and provided a learning opportunity for the therapist, who was then able to explain how animals may be kept in the UK for companionship. This allowed Dalia to see the presence of animals as more acceptable and this cultural exchange was a mechanism for developing the relationship (Newman, Reference Newman, Gilbert and Leahy2007).
Outcome
Subjectively Dalia experienced positive outcomes from her treatment approach, and the therapist also had an opportunity to learn and gain experience in delivering therapy through an interpreter. Dalia's mood had improved and she was engaging in a variety of activities that brought her a sense of achievement as well as increasing her interactions with others. Such activities included interacting with other families and continuing to attend English classes. Dalia's phobia of the hamster was greatly reduced and she has plans to continue this exposure therapy with other types of animals. As sessions progressed the delivery of CBT through the interpreter became more efficient and effective. A three-way relationship started to develop and both Dalia and the therapist became more accustomed to using this medium to communicate.
In the same way that collaboration was used to tackle the depression and phobia, a shared strategy for overcoming the communication barriers also evolved. For example, very simplistic coding was developed when completing the activity monitoring forms as opposed to having to interpret each word. Once a variety of common English words to describe what Dalia had been doing were established, she was able to continually repeat these words and the therapist was able to understand their meaning on a broader scale.
Figure 2 shows the outcome data from the PHQ-9, Generalized Anxiety Disorder Scale (GAD-7; Spitzer et al. Reference Spitzer, Kroenke, Williams and Lowe2006) and the phobia question from the IAPT minimum dataset. The measures indicate a somewhat mixed presentation over the course of treatment with a general trend of reduction. It is unclear how reliable these measures are when used with people of Middle Eastern origin and this could be an area for future research.

Fig. 2. PHQ-9, GAD-7 and Phobia Q3 scores collected at each session.
Discussion
This case study highlighted the difficulties of delivering therapy through an interpreter. This issue becomes particularly pertinent when the community is fairly homogenous as it becomes difficult for both individual therapists and the service to become experienced in this type of work.
Discussions with colleagues from other IAPT services have indicated that these issues could be occurring on a wider scale in IAPT. There were also specific issues with this case that suggest problems could be occurring on a wider scale in IAPT services. Examples of such issues are discussed below:
Therapeutic relationship
In terms of the therapeutic relationship it has been noted in the literature that the close relationship of client and interpreter can leave the therapist feeling disengaged (Kline et al. Reference Kline, Acosta, Austin and Johnson1980). One instance when this seemed particularly acute was during the riots in the Middle East when both the client and the interpreter were concerned about their respective family's welfare. The therapist was able to manage this by becoming familiar with the situation prior to the session to increase understanding of the topic and also by allowing extra time for points to be explained. The therapist also had to disclose when their knowledge of the situation became limited and be open to learning from Dalia about her experience and circumstances (Newman, Reference Newman, Gilbert and Leahy2007).
Learning and supervision
The fact that Dalia's therapist was a trainee at the time meant there was the possibility that the therapist lacked confidence in their own ability as well as the CBT process. It could be perceived that having a third person in the room increases the pressure on the therapist and gives a sense of being scrutinized (Tribe & Thompson, Reference Tribe and Thompson2008). This could also apply to qualified therapists who may be anxious about having an interpreter in the room. Furthermore, the slow pace of sessions and protracted method of conducting therapy could make using the Cognitive Therapy Scale – Revised (CTS-R; Blackburn et al. Reference Blackburn, James, Milne, Baker, Standart, Garland and Reichelt2001) difficult, consequently inhibiting therapists from receiving valuable feedback and developing interaction with interpreters.
Supervision was utilized regularly for reflection purposes and to plan for future sessions. In this case, for example, the therapist was able to identify a transdiagnostic path for treatment which allowed Dalia to benefit more fully from short-term therapy. Supervision was also used to consider and rehearse simple explanations of the theoretical model that could be easily interpreted, and also highlighted the notion that the problems encountered were compounded by limited teaching and literature in this area.
Interventions
Tribe & Lane (Reference Tribe and Lane2009, p. 238) describe language as shaping and constructing meaning rather than a ‘set of interchangeable words’, which might make identifying thoughts and beliefs through an interpreter very complex. Considering this, it would also be difficult to focus on the nuance and subtlety required of thought-challenging techniques, an area which requires further debate. In this case, behavioural interventions such as exposure and behavioural activation were useful to the therapist due to their reliance on basic human learning, rather than detailed language.
In-session dynamic
Within sessions the therapist found it difficult to interrupt while Dalia was talking. There were occasions when Dalia talked for prolonged periods of time, and in shared language therapy there would have been the opportunity to maintain focus by linking back to the agenda. The inability to interrupt led to the dialogue often deviating from the agreed agenda before the therapist was able to rectify the situation. This raised the question as to how Socratic it was possible to be and whether the therapist needed to be more directive at times.
Feedback from the interpreter suggested that Dalia had a good sense of humour and an understanding of sarcasm, something which she had found difficult to convey to the therapist. The interpreter explained that there were moments in therapy where Dalia knew that the therapist had believed something she had said to be of a serious nature when in fact she was speaking sarcastically; however that had been difficult to explain during the session.
The use of questionnaires
It was difficult to establish the validity of the IAPT minimum dataset in the case of Dalia and whether or not it was appropriate to use questionnaires developed in the Western world to people of different cultures (Ahmer et al. Reference Ahmer, Faruqui and Aijaz2007). While it was possible to access the IAPT minimum dataset in Arabic, the therapist had difficulty accessing evidence to support its use and questioned whether it was a semantically and culturally appropriate measure of Dalia's symptoms.
Wider implications
The issues described here are all amplified in a service where it is not commonplace to work with interpreters and so staff do not have the opportunity to build up a rapport with interpreters, and vice versa. Similarly, staff do not have the opportunity to practice using the skills necessary to manage such interactions and develop a natural style of doing this. It is reasonable to suggest that this affects the quality of the service that non-English speakers receive in these areas.
Conclusion and recommendations
It is difficult to make recommendations for practice based upon a single case study. However, the positive therapy outcomes might suggest that some of the alterations to practise were successful. The recommendations for practise may include therapists taking more time to ensure that communication is as good as it can be as this will make integrating culturally sensitive practise far easier. This can be achieved by paying attention to the presence of the interpreter, using more behavioural interventions and simple concepts that are less likely to become lost in translation, as well as using a more directive style at times when the session is diverging from the therapy goals.
It would be useful for trainee therapists in these areas to have access to literature that describes how to integrate different CBT interventions into therapy through an interpreter. Staff might also benefit from spending time in different IAPT services and having more opportunity to work with a variety of foreign-language speakers; which may possibly be achieved by the introduction of secondment opportunities to different areas. This could not only increase the sense of normality when working with an interpreter, but could also significantly reduce anxiety and allow for experiential learning.
The issue of working cross-culturally raises many issues. However, the case study presented here focused on the issue of language and communication through an interpreter. It was the opinion of the therapist that if this could be done more effectively then issues of religion, ethnicity and culture would be easier to explore and integrate into therapy. The dearth of literature in this area and difficulties highlighted in this case reflect a need for more empirical research. However, the subjective and highly nuanced nature of language and interpretation would make this very complicated, and perhaps more clinical reflection would be equally as useful to clinicians in this field. These problems are intensified in areas where the number of people able to speak other languages is minimal and staff do not use interpreters as a matter of course.
Summary
This article presents a case study of a Middle Eastern woman presenting with depression and animal phobia. The discussion focuses on how an interpreter was used during treatment, some of the problems that this presented and how the therapist attempted to overcome them. The ethnic make-up of the area is discussed and how this might impact on therapist confidence in using an interpreter.
Acknowledgements
The authors thanks Dalia for her consent and input, and David Ekers for helpful discussions.
Declaration of Interest
None.
Learning objectives
(1) To explore the use of interpreters in delivering CBT to people with common mental health problems and how the make-up of the local population may impact on therapist learning.
(2) To illustrate the clinical case formulation and treatment of depression and animal phobia and how this was delivered through an interpreter.
(3) To highlight the importance of skills development when using interpreters and how this could be achieved by further research.


Comments
No Comments have been published for this article.