


Introduction
The clinical term social anxiety disorder (SAD) is used to describe pathological anxiety characterized by an excessive fear of scrutiny from others, and avoidance of social interaction (American Psychiatric Association, 2013). SAD can follow a chronic and pernicious course, resulting in significant functional impairment in terms of education, employment and in forming and maintaining meaningful relationships (Bruce et al., Reference Bruce, Yonkers, Otto, Eisen, Weisberg and Pagano2008; Grant et al., Reference Grant, Hasin, Stinson, Dawson, Goldstein and Smith2006; Greca and Lopez, Reference Greca and Lopez1998; Kessler et al., Reference Kessler, Berglund, Demler, Jin, Merikangas and Walters2005; Van Ameringen et al., Reference Van Ameringen, Mancini and Farvolden2003). Despite being a common psychological complaint, SAD is often left undiagnosed and untreated (Fink et al., Reference Fink, Akimova, Spindelegger, Hahn, Lanzenberger and Kasper2009).
In the UK, and in many other healthcare systems around the world, cognitive behavioural therapy (CBT) is a first-line therapy for SAD. Although CBT is an effective treatment for social anxiety, attrition ranges from 10 to 20% (Fernandez et al., Reference Fernandez, Salem, Swift and Ramtahal2015; Swift and Greenberg, Reference Swift and Greenberg2014) and response rates are often less than 50% (Loerinc et al., Reference Loerinc, Meuret, Twohig, Rosenfield, Bluett and Craske2015). However, estimates vary greatly, and response rates of 84–85% have been reported using Clark and Wells’ (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) model of CBT for social anxiety (Clark et al., Reference Clark, Ehlers, Hackmann, Mcmanus, Fennell and Grey2006; Yoshinaga et al., Reference Yoshinaga, Matsuki, Niitsu, Sato, Tanaka and Ibuki2016). Clark and Wells’ model has been found to be an effective model for delivering CBT, and is widely utilized in the UK (Clark et al., Reference Clark, Ehlers, Mcmanus, Hackmann, Fennell and Campbell2003; Mörtberg et al., Reference Mörtberg, Clark, Sundin and Wistedt2007). We chose to conceptualize and measure SAD in reference to Clark and Wells’ cognitive model so that any findings of interest may be translatable into practice. Clark and Wells’ posit that pathological social anxiety develops from negative schemata regarding the self and others, and is maintained by four inter-related and bi-directional cognitive behavioural processes. These processes include: excessive self-focused attention towards internally generated information (such as sensations of nausea or heart palpitations); negatively biased mental representations of one’s outward appearance as it is thought to be perceived by others; utilization of maladaptive safety behaviours; and excessive worry and rumination related to social interaction events. The presentation is theorized as arising from negative core beliefs that underpin intermediate level assumptions about the self and others, resulting in an exaggerated fear of social rejection and the rendering of others as phobic objects. See Fig. 1 for an illustrative example of the model with example cognitive, behavioural and somatic symptoms and characteristics.
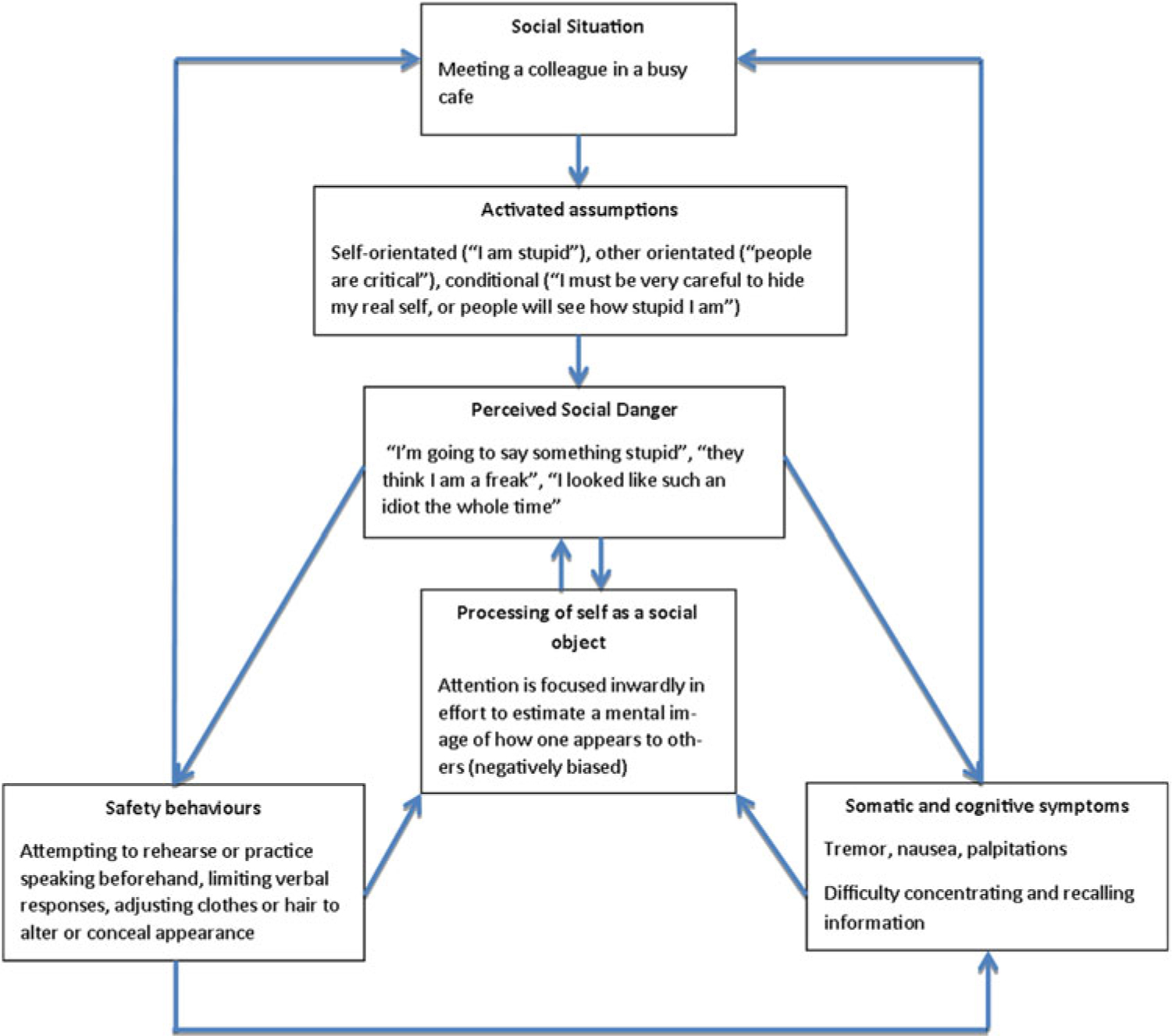
Figure 1. Adapted from Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995), pp. 69–93.
From an attribution theory perspective, SAD is associated with negative explanatory style (Arkin et al., Reference Arkin, Appelman and Burger1980; Stopa and Clark, Reference Stopa and Clark1993; Teglasi and Fagan, Reference Teglasi and Fagin1984). Explanatory style refers to how people tend to attribute causation for outcomes to situations or events along a set of dimensions related to their own and other’s agency. Causation can be perceived as being negative or positive (Weiner, Reference Weiner1986). Psychologically healthy people tend to operate a positive explanatory style, sometimes dubbed a ‘self-serving bias’. When a positive explanatory style is adopted, outcomes perceived as being good are attributed to internal, stable and controllable causes; bad outcomes are attributed to external, unstable and uncontrollable causes. For example, one might make sense of a good exam result as being due to their own intelligence and hard work, and make sense of failing an exam by attributing their poor performance to the ‘wrong’ questions being set for the exam paper. When a negative attributional style is adopted, causation is attributed opposingly, so that good outcomes are perceived as external, unstable and uncontrollable, and poor outcomes as internal, stable and controllable: implying greater personal responsibility for poor outcomes and less responsibility for good outcomes. For example, a socially anxious person might enter into a conversation with a stranger, selectively attending to threat-related cues, becoming highly aware of potentially critical statements or evidence of lack of rapport (such as failing to elicit laughter with a joke). They may then decide the conversation had a poor outcome (e.g. they felt rejected and embarrassed), and that the reasons for this were internal (a result of their own actions), stable (due to their own innate lack of social ability which may be related to a core belief such as being ‘useless’ or ‘different’), and controllable (that is, it is within their power to employ safety-seeking behaviours to avoid poor outcomes such as this).
Inflated responsibility refers to the inclination to readily and excessively accept personal responsibility for actual or potential events which the majority of people are likely to deem separate and independent from themselves. First described and measured within the context of obsessive compulsive disorder (OCD), Salkovskis et al. (Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester and Richards2000) described inflated responsibility as ‘the belief that one has power which is pivotal to bring about or prevent subjectively crucial negative outcomes. These outcomes are perceived as essential to prevent. They may be actual, that is, having consequences in the real world, and/or at a moral level’ (p. 350). Inflated responsibility is considered characteristic of OCD and has been well researched in this context. However, there are data to suggest that inflated responsibility may be a transdiagnostic feature of anxiety disorder (Pozza and Dèttore, Reference Pozza and Dèttore2014a; Startup and Davey, Reference Startup and Davey2003). Pozza and Dèttore, (Reference Pozza and Dèttore2014b) conducted a comprehensive meta-analysis of the available evidence, and found that, depending on the psychometric measures being employed, responsibility was not more strongly associated with OCD over anxiety and depression. In the lead author’s clinical experience, fear-related cognitions elicited during CBT for social anxiety describe a fear of embarrassment or humiliation directly attributed to the patient’s own actions, e.g. ‘I will say something stupid’. The authors hypothesized that patients experiencing social anxiety are prone to fear aversive outcomes which arise as a result of their own actions because, to some unknown degree, they are predisposed to accept personal responsibility for these outcomes.
The purposes of this study were (1) to establish to what extent SAD participants exhibited an inflated sense of responsibility specific to social interaction situations compared with non-anxious control participants; and (2) if a propensity for inflated responsibility were apparent, to establish if a relationship existed between this inflated responsibility and other features of SAD including worry, rumination, use of safety behaviours, self-focused attention and severity of symptoms.
Method
Participants
We recruited 18 patients awaiting CBT for SAD from the waiting list of a primary care mental health service in the UK to act as cases. Patients were 18 years or older and had received a GP referral to the service for therapy to manage pathological social anxiety. Patients with a previous or current diagnosis of OCD or other co-morbid condition that could be causative of social anxiety symptoms (such as panic disorder or PTSD) were excluded.
To act as controls, we recruited 65 healthy individuals from the general public via online advertisements. This was slightly less than the 72 participants needed for a 4:1 allocation ratio, optimal to boost statistical power in case-control studies (Dos Santos Silva, Reference Dos Santos Silva1999). Inclusion was dependent on potential participants completing the ultra-brief 4-item Patient Health Questionnaire screening measure (PHQ-4; Kroenke et al., Reference Kroenke, Spitzer, Williams and Löwe2009) consisting of a 2-item depression scale and a 2-item generalized anxiety scale. Potential participants scoring higher than the recognized healthy population mean for the screening measure were excluded and presented with a message explaining why, and advising them to speak to their GP if they felt they could benefit from help with anxiety or low mood. The measure has demonstrated good reliability and validity in terms of total item correlations (r = 0.62), internal consistency (Cronbach’s alpha = 0.78) and convergence with similar, more comprehensive measures (Löwe et al., Reference Löwe, Wahl, Rose, Spitzer, Glaesmer and Wingenfeld2010).
Waiting list patients eligible to participate were given an information leaflet regarding the study at their initial assessment appointment. These patients were asked if they would be willing to be contacted by telephone at a later date to discuss possible participation in the study. Those who agreed were contacted by the lead author to answer any queries about the study, and to confirm consent to participate. Ethical approval for the study was given by Wales Rec 7 Research Ethics Committee (15/WA/0117). Cambridge and Peterborough NHS Foundation Trust gave site-specific approval, and approval was given by the University of Oxford as study sponsor. In cases where consent was obtained, the participant was sent a secure web link to access the study questionnaires, or offered an appointment to complete the questionnaires at the practice if they were unable to access the internet at home. However, no participants were unable to access the internet at home.
Control group participants were recruited using online advertisements placed on social media and local news websites, and offered entry into a raffle for a £50 online shopping voucher. Participants found to be eligible following completion of the brief screening measure completed the Social Responsibility Attitudes Scale and the Causal Dimensions Scale (Revised) questionnaires via secure web link.
Both groups provided demographic information (age and gender). Cases provided information of current medication usage, and control group participants who wished to enter the raffle provided an email address. These data were held securely in an encrypted folder on a password-protected computer at the practice. No identifiable information such as name, address or date of birth were sought from participants in either group.
Method
Self-report measures
To measure inflated responsibility specific to social interaction we developed the Social Responsibility Attitudes Scale (SRAS). The SRAS is based upon the original Responsibility Attitudes Scale (RAS), developed by Salkovskis and colleagues (Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester and Richards2000). The original RAS was designed to measure perceived sense of responsibility in general terms. Both the RAS and the SRAS consist of 26 items, each of which is answered on a 7-point Likert scale allowing for a possible minimum numerical score of 26 and a maximum of 182, representing lower and higher perceived responsibility. SRAS items were contextually altered so that they could be applied only to social interaction situations rather than a multitude of general situations. For example, the first item of the original RAS would read as ‘I often feel responsible for things which go wrong’, whilst the SRAS reads ‘I often feel responsible for things which go wrong during social interactions’. We found that the SRAS demonstrated internal consistency (Cronbach’s alpha = 0.95) greater than that of the original RAS (Cronbach’s alpha = 0.90–0.92) (Mather and Cartwright-Hatton, Reference Mather and Cartwright-Hatton2004; Salkovskis et al., Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester and Richards2000), probably due to the increased specificity of the concept being measured.
The Causal Dimensions Scale (Revised) (CDS-II) (McAuley et al., Reference McAuley, Duncan and Russell1992) was used to measure explanatory style. The CDS-II is a situation-specific measure of explanatory style in accordance with Weiner’s (Reference Weiner1985) theory of causal attribution. Prior to completing the CDS-II, participants are asked to recall a specific situation or event to complete the measure in reference to. For the purposes of our study we asked participants to recall a social interaction situation perceived to have had a poor outcome leading to embarrassment, humiliation or rejection felt by themselves or others. The measure consists of 12 items along four sub-scales. Each sub-scale pertains to a domain of perceived causality: locus of causality being perceived as internal or external; perceived degree of personal control over outcomes; enduring stability of causal attribution; and perceived degree of external control over outcomes. Each item is anchored by two opposing statements related to the outcome of the reference situation or event, and are separated by a numerical scale used to denote agreement. For the purposes of the study we inverted the scoring of the personal control sub-scale, so that a higher total score represented an increasingly negative explanatory style and a lower score a positive explanatory style. In terms of reliability, average internal consistency across all sub-scales of the CDS-II (as calculated using Cronbach’s alpha coefficient) has been found to range from the lower end of acceptable (locus of causality, Cronbach’s alpha = 0.67; stability, Cronbach’s alpha = 0.67), to good (personal control, Cronbach’s alpha = 0.79; external control, Cronbach’s alpha = 0.82) (Boisvert and Faust, Reference Boisvert and Faust1999). Based on factor analysis carried out by Watkins et al. (Reference Watkins, Sachs and Regmi1997) and Crocker et al. (Reference Crocker, Eklund and Graham2002), the external control sub-scale was dropped for this study in order to increase internal consistency across sub-scales.
To measure symptom severity we used the Social Phobia Inventory (SPIN; Connor et al., Reference Connor, Davidson, Churchill, Sherwood, Weisler and Foa2000). The SPIN is a widely used measure that forms part of the IAPT (Improving Access to Psychological Therapies) minimum dataset used in NHS organizations in England. The SPIN consists of 17 items along three sub-scales, each using a 5-point Likert scale to denote agreement with statements related to fear, avoidance and physiological symptoms of SAD. The SPIN has been found to demonstrate good test–retest reliability (r = 0.78–0.89) and good internal consistency (Cronbach’s alpha = 0.82–0.92) (Antony et al., Reference Antony, Coons, Mccabe, Ashbaugh and Swinson2006; Connor et al., Reference Connor, Davidson, Churchill, Sherwood, Weisler and Foa2000). A cut-off score of 19 (out of a total of 72) is recognized as a reliable predictor of SAD.
We employed a battery of self-report tools to measure the cognitive behavioural processes through to characterize SAD according to Clark and Wells’ model (Clark and Wells, Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995; cited in Heimberg, Reference Heimberg1995). The Anticipatory Processing Questionnaire (APQ) (Vassilopoulos, Reference Vassilopoulos2004) was used to measure anticipatory anxiety prior to engagement in social situations. The APQ consists of 18 items, each answered using a visual analogue scale to denote agreement with opposing statements related to anticipatory anxiety prior to social interaction situations. A total score for each individual item (excluding item 17, which requires a yes/no answer) represents lower or higher anticipatory anxiety. In terms of validity and reliability, the APQ has been found to demonstrate significant convergent validity with previously validated measures of social anxiety (r = 0.49, p ≤ 0.001) and good internal consistency (Cronbach’s alpha = 0.91) (Vassilopoulos, Reference Vassilopoulos2004).
The Post-Event Processing Questionnaire (Revised) (PEPQ-R) (McEvoy and Kingsep, Reference McEvoy and Kingsep2006) was used to measure negatively valenced ruminative thought following engagement in social situations. The PEPQ-R consists of 13 items each answered using a visual analogue scale to denote agreement with opposing statements regarding ruminative thought related to social interaction situations. The PEPQ-R has been found to be reliable, exhibiting good internal consistency (Cronbach’s alpha = 0.89–0.90) (Brozovich and Heimberg, Reference Brozovich and Heimberg2011; McEvoy and Kingsep, Reference McEvoy and Kingsep2006).
The Self-Focused Attention (SFA) (Bögels et al., Reference Bögels, Alberts and Jong1996) scale was used to measure degree of inwardly focused attention. Each of the SFA’s 11 items are answered using a numerical scale to denote agreement with a statement related to self-focused attention along two sub-scales of autonomic arousal and behavioural indicators of inwardly focused attention. The SFA has been found to be a reliable measure, demonstrating good internal consistency (Cronbach’s alpha = 0.78–0.86) (Bögels et al., Reference Bögels, Alberts and Jong1996).
Finally, the Subtle Avoidance Frequency Examination (SAFE) (Cuming et al., Reference Cuming, Rapee, Kemp, Abbott, Peters and Gaston2009) was used to measure frequency of overt and covert safety-seeking behaviour. The SAFE consists of 32 items, answered using a 5-point Likert scale to denote the frequency with which respondents engage in safety-seeking behaviours prior to and during social interaction situations. The SAFE has been found to demonstrate good internal consistency (Cronbach’s alpha = 0.91) and can thus be considered a reliable measure (Cuming et al., Reference Cuming, Rapee, Kemp, Abbott, Peters and Gaston2009).
Results
Descriptive statistics
Descriptive data and between-group differences including t-value and effect size (Cohen’s d) for cases and control participants are presented in Table 1. Median SRAS, CDS-II and CDS-II locus of causality and stability sub-scale scores were significantly higher for cases than for control group participants. There was no significant difference in age between the two groups, but the control group had significant gender imbalance (85% female).
Table 1. Descriptive data and between-group differences

SD, standard deviation; SPIN, Social Phobia Inventory; SRAS, Social Responsibility Attitudes Scale; CDS-II, Causal Dimension Scale; LOC, Locus of Control.
Median scores for psychometric measures specific to social anxiety presentation are presented in Table 3.
Correlation analysis
Pearson’s product moment correlation was carried out using case group participant data, and included demographic variables and psychometric test scores. The results are presented in Table 4. A higher SRAS score was found to be correlated with higher SPIN and SAFE scores; female gender was found to correlate with higher SRAS and SFA scores.
Table 2. Regression coefficients for demographic and psychometric variables

* Control group used as reference category. CDS-II, Causal Dimension Scale 2nd Revision; LOC, Locus of Control; PC, Personal Control.
Regression analysis
Ordinal logistic regression was carried out to find predictors of higher SRAS scores for all participants after controlling for age and gender. ‘Group’ was assigned as a binary factor with the control group as the reference category. SRAS scores were square root transformed prior to regression analysis, as although the dataset could be considered normally distributed, the distribution did exhibit some skewness (–0.19) and kurtosis (2.12). Regression coefficients are presented in Table 2.
Table 3. Descriptive statistics for cases (n = 18)

M, median average (*mean average for age); SD, standard deviation. SPIN, Social Phobia Inventory; SRAS, Social Responsibility Attitudes Scale; APQ, Anticipatory Processing Questionnaire; SFA, Self-Focused Attention scale; SAFE, Subtle Avoidance Frequency Examination; PEPQ-R, Post-Event Processing Questionnaire-Revised.
Table 4. Pearson’s product moment correlation

*Female gender used as reference category; **current medication usage used as reference category; SPIN, Social Phobia Inventory; SRAS, Social Responsibility Attitudes Scale; APQ, Anticipatory Processing Questionnaire; SFA, Self-Focused Attention scale; SAFE, Subtle Avoidance Frequency Examination; PEPQ-R, Post-Event Processing Questionnaire-Revised.
*p < .05, **p < .01, ***p < .001.
Caseness was found to be a significant predictor of higher SRAS score, as was higher CDS-II stability sub-scale score. CDS-II personal control sub-scale scores did not differ significantly between groups and were omitted from regression analysis to avoid hyper-collinearity.
Discussion
We found that cases scored significantly higher on a measure of inflated responsibility specific to social interaction compared with healthy control participants. Furthermore this measure exhibited good internal consistency and correlated well with an existing and well-validated measure of social anxiety symptomatology. Inflated sense of responsibility specific to social interaction correlated highly with social anxiety symptomatology, and with usage of safety-seeking behaviours. We also found statistically significant positive correlations between female gender, inflated responsibility and self-focused attention. At regression analysis, caseness was found to be a significant predictor of inflated sense of responsibility specific to social interaction. Although more rigorous validation is needed, these data suggest that the SRAS is measuring what it is designed to measure, and that inflated sense of responsibility specific to social interaction is associated with SAD.
Cases reported an increasingly negative explanatory style within the context of social interaction situations compared with controls. Regression analysis suggested that stability of causal attribution – but not overall negativity of explanatory style nor externality or internality of locus of control – predicted inflated responsibility. These results suggest that an inability to consider different potential causes for poor outcomes contributes to social anxiety symptoms; e.g. the patient may not have sufficient cognitive flexibility to view an awkward date as being due to a lack of shared interests, as opposed to being due to a lack of social skills on their part – therefore accepting responsibility for the poor outcome. Based on these findings it would appear that an emphasis on cognitive restructuring with a view to increase cognitive flexibility by encouraging the patient to entertain a range of different possible causations would be beneficial. Techniques such as the ‘responsibility pie’ (Veale, Reference Veale2007) could be a useful tool to this end, as could the inclusion of compassion-focused therapy techniques to reduce self-blame and self-criticism (Gilbert, Reference Gilbert2009). See Fig. 2 for an illustrative example of how this approach might fit in to the existing Clark and Wells (Reference Clark, Wells, Heimberg, Liebowitz, Hope and Schneier1995) model.
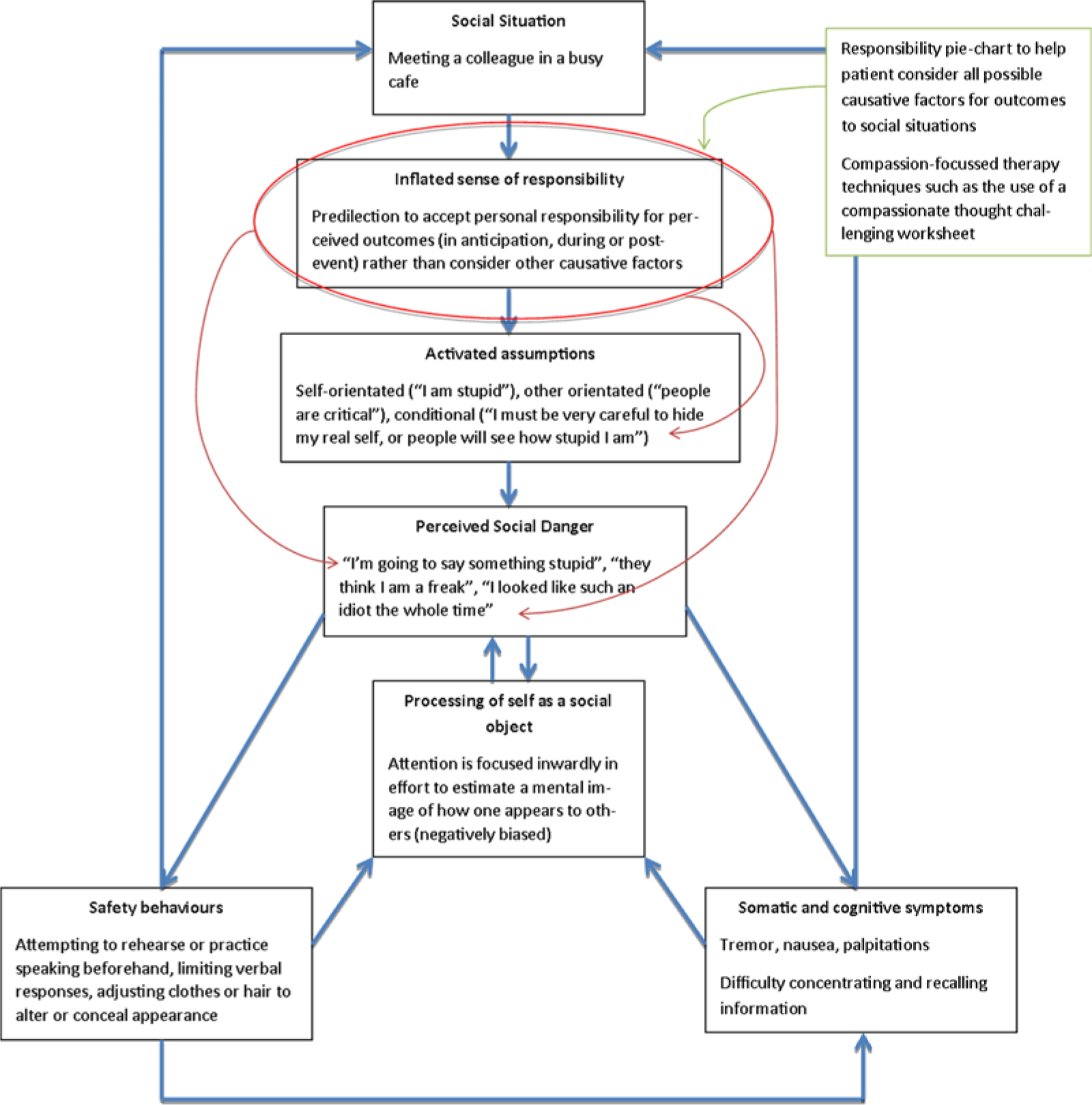
Figure 2. Inflated sense of responsibility and additional treatment components within the cognitive model of social anxiety.
Our study suffered from a lack of a structured diagnostic interview to define caseness, which may have had a deleterious effect on the validity of our results, although all cases scored significantly higher than the recognized cut-off of 19/72, indicating SAD when completing the SPIN measure. As patients were on a waiting list, there is a possibility that an undiagnosed co-morbid problem such as OCD or generalized anxiety disorder may have contributed to inflated responsibility in one or more cases. The study was limited by a sample of cases, and an insufficiently matched control group. Although our results lack sufficient power to confidently assert clear between-group differences in inflated responsibility and explanatory style, these data do highlight the need for further study.
Future research should involve clinical participants and assess whether a tendency to accept excessive moral responsibility for outcomes associated with social interaction contributes to social anxiety presentation, and to what degree. The ramifications for cognitive behavioural case formulation should also be investigated. For example, it may be advantageous to explore the role of maladaptive beliefs and attitudes related to inflated responsibility when working with SAD, and make use of techniques such as the responsibility pie to encourage cognitive change.
Acknowledgement
This study was undertaken as part of an MSc level programme of study.
Declaration of interest
The authors have no conflicts of interest to declare.
Ethical statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, and its most recent revision. Ethical approval for the study was given by Wales Rec 7 Research Ethics Committee (15/WA/0117). Cambridge and Peterborough NHS Foundation Trust gave site-specific approval, and approval was given by the University of Oxford as study sponsor.
Key practice points
(1) Inflated sense of responsibility may form part of anxiety presentations other than OCD.
(2) When formulating SAD, inflated responsibility may be an underlying feature of the presentation.
(3) Inflexible thinking in making sense of outcomes to situations and events may play a role in SAD presentations.







Comments
No Comments have been published for this article.