


Psychological models of psychopathology have long employed a great amount of effort to analyze unipolar depression, as it is the most frequent psychiatric complaint and the first cause of disability worldwide (e.g., Murray & López, Reference Murray and López1996). One of the most popular models of depression is the cognitive model advocated by Beck, Rush, Shaw, and Emery (Reference Beck, Rush, Shaw and Emery1979), which suggests that the core characteristic of depression is a pattern of negative thinking about the self, the world, and the future, known as the cognitive triad. According to this model, negative automatic thoughts are the most proximal cause of depressive symptoms and they are produced when stressful events activate depressogenic schemas. These schemas are considered the distal cause of depression, as they are thought to be shaped by early negative life experiences, to be relatively stable, and to remain latent until the individual encounters negative events that activate them. When this occurs, depressogenic schemas skew the information processing system, leading to the production of negative automatic thoughts, which are more unstable and state-dependent.
Given the relevance of negative automatic thoughts, several measures of the frequency with which individuals experience them have been proposed (Nezu, Ronan, Meadows, & Clure, Reference Nezu, Ronan, Meadows and Clure2000). The most widely used instrument of negative thoughts is the Automatic Thoughts Questionnaire (ATQ; Hollon & Kendall, Reference Hollon and Kendall1980). The ATQ is a 30-item, 5-point Likert-type scale (5 = all the time; 1 = not at all) that measures the frequency of negative automatic thoughts experienced during the past week. The ATQ was developed by asking undergraduates to recall dysphoric experiences and report associated thoughts. One hundred items were generated that were administered to an undergraduate sample and then reduced to the final 30 items. Hollon and Kendall (Reference Hollon and Kendall1980) found that the ATQ had excellent internal consistency, a four-factor structure, and it discriminated between depressive and nondepressive participants.
Numerous studies have confirmed that the ATQ possesses excellent internal consistency, temporal consistency, and convergent and discriminant validity (e.g., Chioqueta & Stiles, Reference Chioqueta and Stiles2004; Hollon & Kendall, Reference Hollon and Kendall1980; Hollon, Kendall, & Lumry, Reference Hollon, Kendall and Lumry1986; Kazdin, Reference Kazdin1990). With regard to the factor structure of the ATQ, exploratory factor analyses have usually yielded more than one factor (e.g., Bryant & Baxter, Reference Bryant and Baxter1997; Cano-García & Rodríguez-Franco, Reference Cano-García and Rodríguez-Franco2002; Chioqueta & Stiles, Reference Chioqueta and Stiles2006; Deardorf, Hopkins, & Finch Jr, Reference Deardorf, Hopkins and Finch1984; Ghassemzadeh, Mojtabai, Karamghadiri, & Ebrahimkhani, Reference Ghassemzadeh, Mojtabai, Karamghadiri and Ebrahimkhani2006; Joseph, Reference Joseph1994; Kazdin, Reference Kazdin1990; Oei & Mukhtar, Reference Oei and Mukhtar2008; Sahin & Sahin, Reference Sahin and Sahin1992; see reviews in Netemeyer et al., Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002; Zettle, Webster, Gird, Wagener, & Burdsal, Reference Zettle, Webster, Gird, Wagener and Burdsal2013), but most studies showed different factorial solutions to the four factors identified by Hollon and Kendall (Reference Hollon and Kendall1980). As noted by Netemeyer et al. (Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002), all studies found that the first factor accounted for a large proportion of the variance, and the remaining factors for only small percentages. Thus, data suggest that a single factor might underlie the 30 items of the ATQ. Furthermore, most studies only use the overall score of the ATQ obtained by summing the scores of the 30 items, which treats the scale as represented by only one factor.
In spite of its excellent psychometric properties, the length of the ATQ can be an obstacle for administering it in some kinds of studies where participants are asked to complete several measures. In other words, measurement efficiency is an issue in this type of research because nonresponse and respondent fatigue need to be considered (Cortina, Reference Cortina1993; Netemeyer et al., Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002). In this sense, longer measures usually have better psychometric properties but might also contain redundant items. Indeed, in narrowly defined constructs, fewer items can result in reliable and valid measures (Clark & Watson, Reference Clark and Watson1995).
Taking into account the results obtained in factor-analytic research and that measurement efficiency can be an issue for using the ATQ, Netemeyer et al. (Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002) offered 15– and 8-item shortened versions of the ATQ. The authors used two samples of 439 and 419 nonclinical participants, respectively, to derive the reduced one-factor versions. Subsequently, two additional cross-validation samples showed that the reduced versions had good psychometric properties, with the ATQ-8 showing coefficient alphas between .85 and .92 across the samples. Additionally, a one-factor structure was obtained in the exploratory and confirmatory factor analyses conducted on the ATQ-8, while less clear results were obtained for the ATQ-15. Correlations between the ATQ, ATQ-15, and ATQ-8 were almost perfect, whereas correlations with other related instruments were basically the same. In conclusion, the ATQ-8 seems to be an efficient measure of the frequency of negative automatic thoughts.
To our knowledge, there is no measure of the frequency of negative automatic thoughts validated in Colombian samples, which makes it difficult to conduct studies in this country related to the cognitive model of depression. Additionally, testing measures in culturally diverse samples enhances both our confidence in the measure and the cross-cultural relevance of the underlying theory being measured (Elosua, Mujika, Almeida, & Hermosilla, Reference Elosua, Mujika, Almeida and Hermosilla2014). Accordingly, the aim of this study was to analyze the factor structure and psychometric properties of the ATQ-8 in Colombia. We used the 8 items of the ATQ-8 from the Spanish version of the ATQ (full scale) by Cano-García and Rodríguez-Franco (Reference Cano-García and Rodríguez-Franco2002). These authors showed that the ATQ had excellent psychometric properties in patients suffering from chronic pain in Spain. A four-factor structure was found with the first one accounting for 53.4% of the variance, which indicated that a single factor might underlie the 30 items of the ATQ.
A secondary aim of this study was to explore metric and scalar invariances across clinical and nonclinical samples. This is important because violations of measurement invariance might impede a meaningful comparison between the scores of clinical and nonclinical samples. To our knowledge, no study has explored the measurement invariance of the ATQ-8 between clinical and nonclinical samples.
After confirming that the ATQ-8 items were understandable by Colombian participants, the test was administered in conjunction with other related measures to three samples with a total of 1587 participants: a sample of 762 undergraduates, a sample of 724 Colombian people recruited through internet, and a clinical sample of 101 participants. We expected the ATQ-8 to show similar psychometric characteristics in Colombia to the original scale and to be sensitive to the effect of the 1-session acceptance and commitment therapy intervention.
Method
Participants
Sample 1
This sample consisted of 762 undergraduates (age range 18–63, M = 21.16, SD = 3.76) from seven universities of Bogotá. Forty-six percent of the sample was studying Psychology. The other studies included Law, Engineering, Philosophy, Communication, Business, Medicine, and Theology. Sixty-two percent were women. Of the overall sample, 26% of participants had received psychological or psychiatric treatment at some time, but only 4.3% were currently in treatment. Also, 2.9% of participants were taking some psychotropic medication.
Sample 2
The sample consisted of 724 participants (74.4% females) with age ranging between 18 and 88 years (M = 26.11, SD = 8.93). The relative educational level of the participants was: 17.8% primary studies (i.e., compulsory education) or mid-level study graduates (i.e., high school or vocational training), 63.8% were undergraduates or college graduates, and 18.4% were currently studying or had a postgraduate degree. They responded to an anonymous internet survey distributed through social media. All of them were Colombian. Forty-five percent reported having received psychological or psychiatric treatment at some time, but only 8.4% were currently in treatment. Also, 5.4% of participants reported using psychotropic medication.
Sample 3
It consisted of 101 patients (52 of them were women) with an age range of 18 to 67 years (M = 32.22, SD = 12.09), suffering from emotional (67.3%) or sexual disorders (32.7%). All participants were being evaluated in some private psychological consultation centers in Bogotá. Only 5% of the participants reported that they were consuming some psychotropic medication.
Sample 4
This sample consisted of 11 participants (2 men, age range: 18 to 32 years, M = 22.18, SD = 4.40,) who participated in a multiple baseline design study that analyzed the effect of a 1-session acceptance and commitment therapy (ACT; Hayes, Strosahl, & Wilson, Reference Hayes, Strosahl and Wilson1999) intervention to disrupt repetitive negative thinking. The relative educational level of the participants was as follows: 1 with mid-level studies, 6 undergraduate students, and 4 college graduates.
Instruments
Automatic Thoughts Questionnaire – 8 (ATQ-8; Netemeyer et al., Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002; Spanish version by Cano-García & Rodríguez-Franco, Reference Cano-García and Rodríguez-Franco2002). The ATQ-8 is the result of reducing the ATQ to only 8 items while maintaining the same instructions and Likert-type scale (Netemeyer et al., Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002). Examples of items are “I’m no good,” “Nothing feels good anymore,” “What’s wrong with me?” and “I’m worthless.” To administer the ATQ-8 in this study, we used only the 8 items of the Spanish version by Cano-García and Rodríguez-Franco (Reference Cano-García and Rodríguez-Franco2002).
Dysfunctional Attitude Scale - Revised (DAS-R; de Graaf, Roelofs, & Huibers, Reference de Graaf, Roelofs and Huibers2009; Spanish version by Ruiz et al., Reference Ruiz, Suárez-Falcón, Odriozola-González, Barbero-Rubio, López-López, Eisenbeck and Gil2015). The DAS is a classic measure of dysfunctional schemas. The revised version of the DAS is a 17-item, 7-point Likert-type scale (7 = fully agree; 1 = fully disagree) grouped in two factors: Perfectionism/Performance evaluation and Dependency. In a Colombian sample, the DAS-R showed excellent psychometric properties and a factor structure with two correlated factors and a second-order factor (Ruiz, Suárez-Falcón, Barón-Rincón et al., Reference Ruiz, Suárez-Falcón, Barón-Rincón, Barrera-Acevedo, Martínez-Sánchez and Peña2016). In this study, the DAS-R showed a Cronbach’s alpha of .91. According to the cognitive model of depression, medium to strong correlations between the ATQ-8 and the DAS-R were expected.
Depression, Anxiety, and Stress Scales – 21 (DASS-21; Antony, Bieling, Cox, Enns, & Swinson, Reference Antony, Bieling, Cox, Enns and Swinson1998; Spanish version by Daza, Novy, Stanley, & Averill, Reference Daza, Novy, Stanley and Averill2002). The DASS-21 is a 21-item, 4-point Likert-type scale (3 = applied to me very much, or most of the time; 0 = did not apply to me at all) consisting of sentences describing negative emotional states. It contains three subscales (Depression, Anxiety, and Stress) and has shown good internal consistency and convergent and discriminant validity. The DASS-21 has shown good psychometric properties in Colombia (Ruiz, García-Martín, Suárez-Falcón, & Odriozola-González, Reference Ruiz, García-Martín, Suárez-Falcón and Odriozola-González2017) and hierarchical factor structure with three first-order factors (Depression, Anxiety, and Stress) and a second-order factor (Emotional Symptoms). The DASS-21 was administered because the frequency of negative thoughts strongly correlated with emotional symptoms in previous studies, not only with depression. Therefore, strong correlations between the ATQ-8 and the DASS-21 subscales were expected.
General Health Questionnaire – 12 (Goldberg & Williams, Reference Goldberg and Williams1988; Spanish version by Rocha, Pérez, Rodríguez-Sanz, Borrell, & Obiols, Reference Rocha, Pérez, Rodríguez-Sanz, Borrell and Obiols2011). The GHQ-12 is a 12-item, 4-point Likert-type scale that is frequently used as screening for psychological disorders. Respondents are asked to indicate the degree to which they have recently experienced a range of common symptoms of distress, with higher scores reflecting greater levels of psychological distress. The Likert scoring method was used in this study, with scores ranging from 0 to 3 assigned to each of the four response options. Alpha values for the GHQ-12 in this study were good (Sample 1: .88; Sample 3: .93). The GHQ-12 was administered because the frequency of negative thoughts is positively correlated with measures of psychological distress. Medium to strong positive correlations were, therefore, expected between the ATQ-8 and the GHQ-12.
Satisfaction with Life Survey (SWLS; Diener, Emmons, Larsen, & Griffin, Reference Diener, Emmons, Larsen and Griffin1985; Spanish version by Atienza, Pons, Balaguer, & García-Merita, Reference Atienza, Pons, Balaguer and García-Merita2000). The SWLS is a 5-item, 7-point Likert-type scale (7 = strongly agree; 1 = strongly disagree) that measures self-perceived well-being. Examples of items are “I am satisfied with my life” and “In most ways, my life is close to my ideal.” The SWLS has good psychometric properties and convergent validity. Alpha values in this study for the SWLS were good (Sample 1: .85; Sample 2: .89; Sample 3: .84). As previous research has shown that the frequency of negative thoughts negatively correlates with life satisfaction, medium to strong negative correlations were expected between the ATQ-8 and the SWLS.
Acceptance and Action Questionnaire – II (AAQ-II; Bond et al., Reference Bond, Hayes, Baer, Carpenter, Guenole, Orcutt and Zettle2011; Spanish translation by Ruiz, Langer, Luciano, Cangas, & Beltrán, Reference Ruiz, Langer, Luciano, Cangas and Beltrán2013). The AAQ-II is a 7-item, 7-point Likert-type scale (7 = always; 1 = never true) that measures general experiential avoidance or psychological inflexibility. The items reflect unwillingness to experience unwanted emotions and thoughts and the inability to be in the present moment and behave according to value-directed actions when experiencing unwanted psychological events. The Spanish version by Ruiz, Suárez-Falcón, Cárdenas-Sierra, et al. (Reference Ruiz, Suárez-Falcón, Cárdenas-Sierra, Durán, Guerrero and Riaño-Hernández2016) showed good psychometric properties (mean alpha of .90) and a one-factor structure in Colombian samples. The AAQ-II was administered because previous research has shown strong positive correlations between the AAQ-II and ATQ scores (e.g., Ruiz & Odriozola-González, Reference Ruiz and Odriozola-González2016).
Mindful Attention Awareness Scale (MAAS; Brown & Ryan, Reference Brown and Ryan2003; Spanish version by Soler et al., Reference Soler, Tejedor, Feliu-Soler, Pascual, Cebolla, Soriano and Pérez2012). The MAAS is a 15-item, 6-point Likert-type scale (6 = almost never; 1 = almost never) designed to measure the extent to which individuals pay attention during several tasks or, in contrast, behave on “autopilot,” without paying enough attention to the tasks. The MAAS does not require familiarity with meditation. Higher scores indicate greater mindfulness level. The MAAS has shown good psychometric properties and a one-factor structure in a Colombian sample (Ruiz, Suárez-Falcón, & Riaño-Hernández, Reference Ruiz, Suárez-Falcón, Barón-Rincón, Barrera-Acevedo, Martínez-Sánchez and Peña2016). The MAAS was administered in view of the established negative correlation between present moment awareness and frequency of negative thoughts. Medium to strong negative correlations were expected between the ATQ-8 and the MAAS.
Procedure
A small pilot study was conducted to explore whether the items of the ATQ-8 were understandable by Colombian participants. Specifically, ten Colombian undergraduates were asked to rate item clarity. The undergraduates rated the items as highly understandable, so we did not change any of them.
In Sample 1, the administration of the questionnaire package was conducted in the participants’ classrooms during the beginning of a regular class. Participants in Sample 2 responded to an anonymous internet survey distributed through social media (e.g., institutional webpages, Facebook profiles, etc). Lastly, participants in Sample 3 responded to the questionnaires during one of the clinical assessment interviews at the beginning of the treatment in the presence of their therapist.
In Samples 1 to 3, participants provided informed consent and were given a questionnaire packet. Participants in Sample 1 responded to the ATQ-8, AAQ-II, DASS-21, GHQ-12, MAAS, DAS-R, and SWLS. Participants in Sample 2 responded to the ATQ-8, AAQ-II, SWLS, and DASS-21. Participants in Sample 3 responded to the GHQ-12 in addition to the questionnaires administered in Sample 2. The number of questionnaires applied varied across samples according to the available time for conducting the assessment. Upon completion of the study, participants were debriefed about the aims of the study and thanked for their participation. No incentives were provided for participation.
Participants in Sample 4 were recruited through advertisements in social media and had spent at least 6 months entangled in thoughts, memories, and/or worries that provoked significant interference in at least two life areas. Additional information of the inclusion and exclusion criteria can be seen in Ruiz, Riaño-Hernández, Suárez-Falcón, and Luciano (Reference Ruiz, Riaño-Hernández, Suárez-Falcón and Luciano2016). Participants completed a baseline period ranging between 2 to 10 weeks during which the ATQ-8 was administered every 2 weeks in addition to other measures. Subsequently, participants received a one-session ACT intervention specifically oriented to disrupt repetitive negative thinking in the form of worry and rumination. Participants then completed follow-up measures for 6 weeks (one measurement each 2 weeks). The ACT protocol consisted of an approximately 75-minute, individual session. The main objectives of the protocol were: (a) to identify triggers for negative repetitive thinking and experiential avoidance strategies related to them, (b) to promote creative hopelessness regarding the counterproductive effect of engaging in repetitive negative thinking and the other experiential avoidance strategies, (c) to promote values clarification and the commitment to valued actions, and (d) to introduce defusion training. It was expected that participants would show significant changes on the ATQ-8 to the extent that disrupting worry/rumination would decrease the frequency of negative thoughts.
Data analysis
Prior to conducting factor analyses, data from Samples 1 to 3 (Sample 4 was too small to conduct factor analyses and was only used to analyze the treatment sensitivity of the ATQ-8) were examined searching for missing values, which were imputed using the matching response pattern of LISREL© (version 8.71, Jöreskog & Sörbom, Reference Jöreskog and Sörbom1999), which was the software used to conduct the confirmatory factor analyses (CFA). Fifty-nine values were missing (from 7 for Item 6 to 11 for Items 2 and 8), which represents only 0.60% of the data. In this imputation method, the value to be substituted for the missing value of a single case is obtained from another case (or cases) having a similar response pattern over the remaining items of the ATQ-8.
Because the ATQ-8 uses a Likert-type scale measured on an ordinal scale, a weighted least squares (WLS) estimation method using polychoric correlations was used in conducting the CFA. The WLS method is recommended in large samples with fewer than 20 items, as in the current study (Jöreskog & Sörbom, Reference Jöreskog and Sörbom1996). We computed the chi-square test and the following goodness of fit indexes for the one-factor model: (a) the root mean square error of approximation (RMSEA); (b) the comparative fit index (CFI); and (c) the non-normed fit index (NNFI). According to Kelloway (Reference Kelloway1998) and Hu and Bentler (Reference Hu and Bentler1999), RMSEA values below .10 represent an acceptable fit, and values below .05 represent a very good fit to the data. With respect to the CFI and NNFI, values above .90 indicate acceptable-fitting models, and above .95 represent a good fit to the data.
Additional CFA were performed to test for metric and scalar invariances across samples and gender following Jöreskog (Reference Jöreskog2005), and Millsap and Yun-Tein (Reference Millsap and Yun-Tein2004). In other words, we analyzed whether the item factor loadings and items intercepts are invariant across the three samples and between men and women. In so doing, the relative fits of three increasingly restrictive models were compared: the multiple-group baseline model, the metric invariance model, and the scalar invariance model. The multiple-group baseline model allowed the eight unstandardized factor loadings to vary across the three samples and across men and women. The metric invariance model, which was nested within the multiple-group baseline model, placed equality constraints (i.e., invariance) on those loadings across groups. Lastly, the scalar invariance model, which was nested within the metric invariances model, is tested by constraining the factor loadings and the items intercepts to be the same across groups. Equality constraints were not placed on estimates of the factor variances because these are known to vary across groups even when the indicators are measuring the same construct in a similar manner (Kline, Reference Kline2005). For the model comparison, the RMSEA, CFI, and NNFI indices between nested models were compared. The more constrained model was selected (i.e., second model versus first model, and third model versus second model) if the following criteria suggested by Cheung and Rensvold (Reference Cheung and Rensvold2002) and Chen (Reference Chen2007) were met: (a) the difference in RMSEA (ΔRMSEA) was lower than .01; (b) the differences in CFI (ΔCFI) and NNFI (ΔNNFI) were equal to or greater than –.01.
The remaining statistical analyses were performed on SPSS 19©. Coefficient alphas were computed providing 95% confidence intervals (CI) to explore the internal consistency of the ATQ-8 in Samples 1 to 3 and the overall sample. Corrected item-total correlations were obtained to identify items that should be removed because of low discrimination item index (i.e., values below .20). Descriptive data were also calculated, and gender differences in ATQ-8 scores were explored by computing independent sample t-test. To examine criterion validity, scores on the ATQ-8 were compared between participants in Sample 1 and 2 (nonclinical participants) and participants in Sample 3 (clinical participants). Pearson correlations between the ATQ-8 and other scales were calculated to assess convergent construct validity. Lastly, to explore whether the ATQ-8 scores were sensitive to the effects of a 1-session ACT intervention, a paired sample t-test was conducted between the last ATQ-8 score of participants’ baseline and the 6-week follow-up. Cohen’s d for within-participant studies was also computed.
Results
Descriptive data and psychometric quality of the items
Table 1 shows the original items of the ATQ-8, their translation into Spanish, the descriptive data and corrected item-total correlations for each sample. All items showed good discrimination, with corrected item-total correlations ranging from .56 to .64 in Sample 1, from .63 to .78 in Sample 2, and from .46 to .73 in Sample 3.
Table 1. Item Description, Corrected Item-Total Correlations, Descriptive Data

Table 2 shows that Coefficient alpha of the ATQ-8 ranged from .85 (Sample 1) to .91 (Sample 2), with an overall alpha of .89. There were no differences on ATQ-8 scores between men and women across Samples 1 to 3.
Table 2. Coefficient alphas and Descriptive Data across Samples

Validity evidence based on internal structure
Dimensionality
The overall fit of the one-factor model was adequate, and scores on the goodness-of-fit indexes were good: χ2(20) = 237.62, p < .01; RMSEA = .083, 90% CI [.074, .092], CFI = .96, NNFI = .95. Figure 1 depicts the results of the standardized solution of the one-factor model.

Figure 1. Results of the confirmatory factor analysis conducted with the overall sample to analyze the fit of a one-factor model.
Measurement invariance
Table 3 shows the results of the metric and scalar invariance analyses. Parameter invariance was supported at both the metric and scalar levels across samples and gender because changes in RMSEA, CFI, and NNFI were lower than .01.
Table 3. Metric and Scalar Invariance across Samples and Gender

Validity evidence based on relationships with other variables
The ATQ-8 showed correlations with all the other assessed constructs in theoretically coherent ways (see Table 4). Specifically, the ATQ-8 showed positive correlations with psychological inflexibility (AAQ-II), depression, anxiety, and stress symptoms (DASS-21), emotional distress (GHQ-12), and dysfunctional attitudes (DAS-R); and negative correlations with mindful awareness (MAAS), and satisfaction with life (SWLS).
Table 4. Pearson Correlations between the ATQ-8 Scores and Other Relevant Self-report Measures
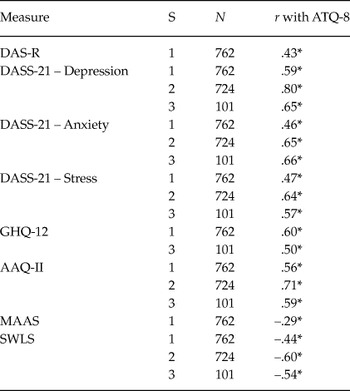
Note: AAQ-II: Acceptance and Action Questionnaire – II; ATQ-8: Automatic Thoughts Questionnaire – 8; DAS-R: Dysfunctional Attitude Scale – Revised; DASS: Depression, Anxiety, and Stress Scales – 21; GHQ-12: General Health Questionnaire – 12; MAAS: Mindful Attention Awareness Scale; SWLS: Satisfaction with Life Scale. *p < .001.
Means and standard deviations of the ATQ-8 score for each sample can be seen in Table 2. Participants’ mean score in the clinical sample (Sample 3) was higher than those of participants in Sample 1 (t = –5.75, p < .001) and Sample 2 (t = –2.95, p = .004).
Sensitivity to treatment
In Sample 4, participants’ mean score during the baseline assessment was 21.45 (SD = 5.58), whereas the mean score at the 6-week follow-up was 12.45 (SD = 4.78). The difference was statistically significant and with a very large effect size (t = 6.05, p < .001, d = 1.61).
Discussion
While some Spanish versions of the ATQ already existed, to our knowledge, no study has explored the psychometric properties and factor structure of the ATQ-8 in Spanish, which was the main aim of this study. The data obtained showed that this Spanish version of the ATQ-8 has good psychometric properties in Colombia. Specifically, the ATQ-8 showed construct validity to the extent that factor analysis yielded a one-factor solution, as in Netemeyer et al. (Reference Netemeyer, Williamson, Burton, Biswas, Jindal, Landreth and Primeaux2002). The internal consistency of the ATQ-8 was good, with an overall alpha of .89, and it showed criterion validity to the extent that its scores discriminated between clinical and nonclinical samples. The instrument also showed convergent validity in view of the positive correlations found with dysfunctional schemas, emotional symptoms, and psychological inflexibility, and the negative correlations with mindfulness and life satisfaction. Lastly, the ATQ-8 was shown to be sensitive to the effect of a one-session ACT intervention focused on disrupting repetitive negative thinking.
This study also provides evidence of the measurement invariance (metric and scalar) of the ATQ-8 in Colombia across clinical and nonclinical samples. This indicates that the ATQ-8 scores have a similar origin (metric invariance) and that they can be compared since equality of factor loadings and intercepts has been found (scalar invariance). These findings are especially relevant because no study to date had explored the measurement invariance of the ATQ-8. Further studies might try to replicate this finding in other countries including additional Spanish-speaking countries.
Some limitations of this study are worth mentioning. Firstly, the functioning of the ATQ-8 was tested only in one relatively small clinical sample so that further research is necessary in larger clinical samples to confirm the results obtained in this study. Secondly, no systematic information was obtained concerning the specific diagnosis in clinical participants because they were categorized in broad categories such as emotional and sexual disorders. Thirdly, some of the instruments used to explore the convergent and divergent validity of the ATQ-8 lacked formal validation in Colombian samples (e.g., SWLS); however, their internal consistencies in the current study were adequate and similar to the ones obtained in the original language validation studies.
In conclusion, according to the reliability and validity data provided in this study, this Spanish version of the ATQ-8 can be used to measure the frequency of negative thoughts as experienced by individuals suffering from depression in Colombia.





