Introduction
Mass murder has generally been defined as the unlawful killing of four or more individuals, excluding the perpetrator(s), within one event, in one location. In 2013, the US Congress proposed the alternative parameter of three or more victims (Douglas, Burgess, Burgess, & Ressler, Reference Douglas, Burgess, Burgess and Ressler2012; Krouse & Richardson, Reference Krouse and Richardson2015). In the USA, mass murders involving firearms, commonly termed mass shootings, have become more prevalent, with greater numbers of casualties, since 2000, and especially since 2010 (Follman, Aronsen, & Pan, Reference Follman, Aronsen and Pan2019; Peterson & Densley, Reference Peterson and Densley2019). Although mass shootings account for only a small fraction of the murders committed annually in the USA or worldwide (https://www.cdc.gov/nchs/fastats/homicide.htm), they exert a disproportionately strong influence on society, invoking collective fear and calls for preparedness and policy changes. This growing public health concern has prompted calls for discourse and research regarding the relationship between mass shootings and mental illness (McGinty, Webster, & Barry, Reference McGinty, Webster and Barry2014; Parks, Bechtold, Shelp, Lieberman, & Coffey, Reference Parks, Bechtold, Shelp, Lieberman and Coffey2019), with potential implications for the stringency of state firearm laws (Reeping et al., Reference Reeping, Cerda, Kalesan, Wiebe, Galea and Branas2019) and other policy changes that might aid prevention (Gostin, Reference Gostin2016; McGinty et al., Reference McGinty, Webster and Barry2014; Sacks et al., Reference Sacks, Malina, Morrissey, Campion, Hamel and Drazen2016; Wintemute, Reference Wintemute2018).
Depending on the definition of mental illness used, the proportion of mass shootings associated with it varies from 4.7% to 78% across studies (Parks et al., Reference Parks, Bechtold, Shelp, Lieberman and Coffey2019). Silver, Simons & Craun (Reference Silver, Simons and Craun2018) reported that 25% of 63 active shooters identified by the Federal Bureau of Investigation (FBI) had psychiatric disorders. Among the perpetrators of 167 mass shootings in the USA between 1966 and 2019 analyzed for The Violence Project, 19% had previously been hospitalized for psychiatric reasons; 25% had undergone counseling; 20% had used psychotropic medications; 23% had mood disorders; and 26% exhibited thought disorders (Peterson & Densley, Reference Peterson and Densley2019). Psychosis was at least a partial motivating factor in 15.8% of cases. Stone found that 22% of mass murderers were mentally ill (Stone, Reference Stone2015). Appelbaum (Reference Appelbaum2013), noting that severe mental disorders may be overrepresented among mass shooters, suggested that attempts to draw firm conclusions about this relationship are limited by nonsystematic data collection.
Most individuals with psychosis are not dangerous and the majority of violence is committed by non-psychotic individuals (Taylor, Reference Taylor2008). Some research, however, suggests a somewhat increased risk for violence, especially homicide, among individuals with psychotic symptoms or disorders (Fazel, Gulati, Linsell, Geddes, & Grann, Reference Fazel, Gulati, Linsell, Geddes and Grann2009; Keers, Ullrich, Destavola, & Coid, Reference Keers, Ullrich, Destavola and Coid2014; Large & Nielssen, Reference Large and Nielssen2011; McNiel, Eisner, & Binder, Reference McNiel, Eisner and Binder2000; Swanson et al., Reference Swanson, Swartz, Van Dorn, Elbogen, Wagner, Rosenheck and Lieberman2006), especially during their first episodes (Large & Nielssen, Reference Large and Nielssen2011), while other reports suggest that abuse of drugs or alcohol is a key mediating factor (Elbogen & Johnson, Reference Elbogen and Johnson2009; Steadman et al., Reference Steadman, Mulvey, Monahan, Robbins, Appelbaum, Grisso and Silver1998; Swartz et al., Reference Swartz, Swanson, Hiday, Borum, Wagner and Burns1998). This and other work has implied a link between violence and psychosis (Walsh, Buchanan, & Fahy, Reference Walsh, Buchanan and Fahy2002), which may be misrepresented by the media in the context of mass violence (Parks et al., Reference Parks, Bechtold, Shelp, Lieberman and Coffey2019) and generate stigma (Hirschtritt & Binder, Reference Hirschtritt and Binder2018; Phelan & Link, Reference Phelan and Link1998). Thus, the potential relationship between mass shootings and mental illness constitutes a critical public health concern.
To date, efforts to understand the causes and impacts of mass shootings have generally involved descriptive reports or databases detailing perpetrators' biographical information, including mental health-related characteristics and various features of their attacks (Follman et al., Reference Follman, Aronsen and Pan2019; Gun Violence Archive, 2020; Mass Shootings in America: 2020; Peterson & Densley, Reference Peterson and Densley2019; Stanford Mass Shootings in America; Stone, 2015). Such efforts, while laudable, have been limited in several respects. First, relying on descriptive data, without incorporating a comparison group, renders the results particularly susceptible to various biases, including selection bias. Second, the definition of mass shooting as involving three v. four victims have been inconsistent across studies, with no attempts within a given report to determine whether alternative definitions alter results (Booty, O'Dwyner, Webster, McCourt, & Crifasi, Reference Booty, O'Dwyner, Webster, McCourt and Crifasi2019). Additionally, reports have generally focused on mass shootings occurring in the USA alone and no earlier than 1966, yielding varied sample sizes limited to several hundred events. Furthermore, few reports have carefully distinguished mass murders from spree murders, defined as the killing of two or more victims in one event in two or more locations, with no cooling-off period between murders (Krouse & Richardson, Reference Krouse and Richardson2015), despite potential differences between these types of murders (Douglas et al., Reference Douglas, Burgess, Burgess and Ressler2012; Morton, Reference Morton2008). Fifth, there has been inconsistency regarding whether cases involving gang violence or terrorism were included (Booty et al., Reference Booty, O'Dwyner, Webster, McCourt and Crifasi2019). Finally, reports have generally not considered mass shootings within the larger framework of mass murders by other means, such as stabbing, arson or explosives.
We sought to address these limitations by creating the Columbia Mass Murder Database, examining personal cause mass murders worldwide from 1900 to 2019, subsuming the subcategory of mass shootings. We used inferential statistics and comparison groups to better understand the prevalence of psychosis and mental illness in general in mass shooting incidents. We hypothesized that the majority of mass murders are committed by persons without a history of severe mental illness (i.e. psychosis) and that even fewer have a history of psychosis when the mass murder is committed with a firearm.
Methods
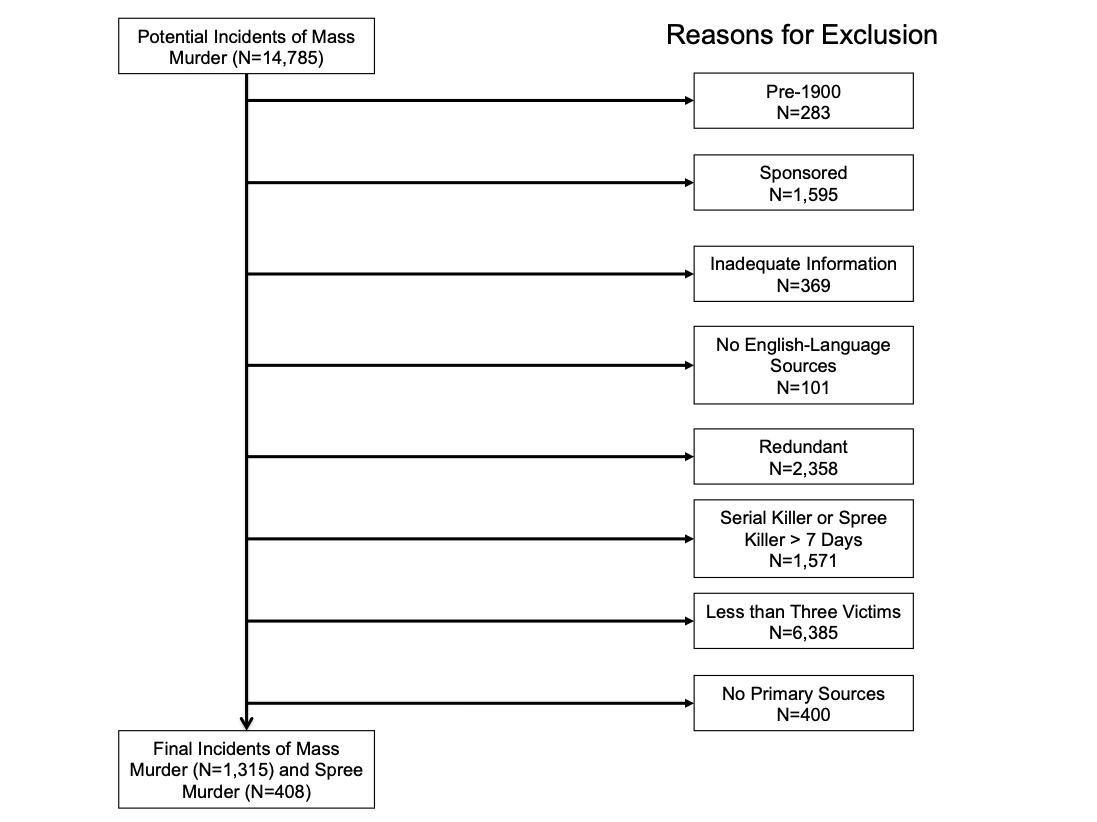
We collated potential incidents of mass murder worldwide between 1900 and 2019 and perpetrator names through an extensive review of English-language databases of murderers and mass murderers publicly available in print and online. Some databases included only mass murderers (e.g. Everytown for Gun Safety, Stanford), while others also included killings involving less than three victims in single incidents, or spree and serial killers (e.g. Murderpedia.org). For the present study, we focused on personal-cause mass murders, meaning those driven by personal motivations and not occurring within the contexts of war, state- or group-sponsored terrorism, gang activity, or organized crime. Mass murders stemming from family matters and other killings of close associates were not excluded. Felonious mass homicides with automobiles or other vehicles, related to impairment or recklessness, were excluded. Additionally, we employed the Congressional definition of mass murder, involving three or more fatalities, excluding perpetrators. We reviewed 14 785 cases of murder in total for potential cases of mass murder. For a complete description of our methods, sources examined, and a flow diagram of our search results, see the online Supplement, Supplementary Table S1 and Fig. S1.
Perpetrators better categorized as spree killers, due to having killed two (three for the current analyses) or more people in more than one location or at more than one point in time, with no cooling-off period (which we defined as killing across one week or less) between murders, were retained for separate analysis. To be conservative, perpetrators who committed any two episodes of murder with any victim count more than 7 days apart were excluded, irrespective of any connections between murders.
Critically, while we gathered names and incidents from academic (e.g. Stanford University), governmental/public (e.g. FBI data), and lay/popular (e.g. Murderpedia, Mother Jones) sources, all other information in our database was obtained from contemporaneous, primary sources and reports (i.e. we did not use any information from the non-primary sources listed in online Supplementary Table S1, beyond perpetrator names, except for the Everytown for Gun Safety report). This was done to reduce the possibility of misclassifying cases of mass murder in which psychotic symptoms had been overlooked or mischaracterized by previous reports. All data came from contemporaneous, English-language media reports, as well as court/police reports when available online (11%). When information was available in one of these other sources (e.g. Stanford database) or on a website (e.g. Wikipedia, Mother Jones), but no English-language, contemporaneous, primary source was available, we excluded the case (N = 501). We also excluded mass murders for which we lacked information on victim count or method (N = 369), the minimal amount of information required for inclusion. While we did not require demographic information, per se, this was available for most perpetrators.
Please see the online Supplement for additional methods.
Statistical analyses
Descriptive statistics were used to characterize demographic (age, gender, race) and clinical features [history of psychotic symptoms (i.e. hallucinations, delusions, and/or thought disorganization), drug use] of the sample. We examined mass murderers, separating them into two groups: those who used firearms (i.e. mass shooters) and those who did not (i.e. mass murderers of other types). Our primary dependent variable was the proportion of individuals with a reported history of psychotic symptoms in each group. Differences in demographics and clinical features between those who used v. did not use firearms were tested using Pearson χ2 tests for categorical variables (e.g. history of psychotic symptoms, gender), and two-sample t tests for continuous variables. Graphical display of the frequency of mass murders across every decade from 1900 to 2019 is presented normalized by the world population (https://en.wikipedia.org/wiki/World_population; https://www.census.gov/data/tables/time-series/demo/international-programs/historical-est-worldpop.html; https://www.worldometers.info/world-population/world-population-by-year/) providing the rate of mass murders per one billion people. Poisson regression tested trends over time in the rate of mass murder by type (firearm or not) with an inflection point at 1970, based on visual inspection. Adjustment to standard errors in the Poisson regression due to overdispersion was made using the square root of the Pearson chi-square divided by the degrees of freedom. Additionally, multiple logistic regression was performed to examine the independent effects of variables of interest, while controlling for year, on the odds of using v. not using a firearm to commit mass murder. Further analyses examined mass shootings and compared demographic and clinical feature differences between the USA v. elsewhere in the world. Finally, we subdivided the data even further to include only those mass shootings in the USA since 1970 and compared differences between those using non-automatic v. semi- or fully-automatic weapons. Similar to the previous analyses, differences in demographics and clinical features were tested using Pearson chi-square for categorical variables and two-sample t tests for continuous variables. Significance was set at p < 0.05 for all tests.
Results
We originally included in our dataset 1315 mass and 408 spree murders (total N = 1723) that occurred worldwide between 1900 and 2019. While almost two-thirds (855, 65%) of mass murders were committed using firearms, they were used in a significantly greater proportion (330, 81%) of spree murders (χ2 = 36.5, p < 0.001). This difference indicates that spree and mass murders substantially diverge in how they are perpetrated. Thus, subsequent analyses were focused on mass murders.
Characteristics of mass murders and their perpetrators
The 1315 cases of mass murder accounted for 10 877 fatalities (average = 8.3 fatalities per event, s.d. = 22.1). See Tables 1 and 2 for a description of the entire sample and Fig. 1 for the frequency of events by decade. When normalized by the worldwide population, the average rate of mass murders remained steady from 1900 until 1970 at 6.5 mass-shootings per billion people (95% confidence interval 3.6–11.7) and 6.6 (95% confidence interval 3.7, 11.8) non-firearm mass murders per billion. In the later period from 1970 to 2019, there was a four-fold increased relative risk (RR) = 4.38 (p < 0.001) in mass shootings compared to the earlier epoch to 28.5 mass shootings per billion (95% confidence interval 23.4–35.2) and a two-fold increase (RR = 2.07, p = 0.032) in non-firearm mass murders to 13.6 per billion (95% confidence interval 10.0–18.5). Thus, since 1970, mass shootings have occurred at more than twice the rate of other non-firearm mass murders (RR = 2.10, p < 0.001). Although approximately two-thirds of all mass murders were mass shootings, mass murders involving other means were responsible for more fatalities (6229 v. 4648). An average of 13.5 fatalities occurred per event for mass murder committed by means other than firearms v. 5.4 fatalities per event for mass shootings (p < 0.01). The majority of cases involved four or more victims (946, 72%) and occurred after 1970 (1112, 85%). The vast majority of mass murderers were male (92%). Over half of the cases included were US-based (63%) and just over half were committed by Caucasian individuals (52%). The average age of perpetrators was 32.3 (s.d. = 11.2), with a range of 11–76 years. Approximately 28% of mass murderers completed suicide at the time of their offenses. A lifetime history of psychotic symptoms was identified in 11% of mass murderers and 30% had histories of symptoms of any psychiatric or severe neurologic disorder (Tables 1 and 2), excluding those with only lifetime histories of drug use (primarily marijuana) or alcohol misuse, which were observed in 22% of all individuals. Of the total, 20% of mass murderers had histories of being subject to a restraining order, arrest or incarceration. Online Supplementary Table S2 describes the sample when limited to the post-1970 era of mass murder in the USA [i.e. following the period when several semi-automatic firearms became commercially available (Fallows, Reference Fallows2017); N = 734], which is similar to the overall sample. For additional results on changes in the frequency and fatality rates of mass murder in the USA between 1900 and 2019, see the online Supplement.
Table 1. Description of sample

a Differences between firearms and non-firearms are assessed using χ2 tests for categorical measures, except age (continuous) which was tested using a two-sample t test. Separate levels of categorical measures with more than two-categories were tested by multiple χ2 tests dichotomizing into the specific level v. all others (e.g. the χ2 test of the association between firearms and Asia v. all other locations have p < 0.01).
N/A χ2 test was not a valid test due to low expected cell counts.
The bold values are the significance levels.
Table 2. Frequencies of all psychiatric and neurologic symptoms of mass murderers


Fig. 1. Frequency of usage of firearms and non-firearms in mass murders worldwide by decade, 1900–2019, normalized by population, frequency per 1 billion people.
Mass shooters v. mass murderers of other types
Although the prevalence of a history of psychotic symptoms among mass murderers is much higher than that in the general population (11% v. approximately 0.3–1%), we note that it was lower (8%) among those who used firearms to commit mass murder than those who used other means (18%, χ2 = 28.0, p < 0.01). Findings were similar when limiting the sample to US-based mass murders (χ2 = 21.5, p < 0.01) and in males (χ2 = 15.4, p < 0.01) as well as females (χ2 = 7.3, p < 0.01). This finding also emerged when the four-victim definition of mass murder was used (χ2 = 20.9, p < 0.01), when only post-1970 cases were examined (χ2 = 21.6, p < 0.01), and when spree killers were included in the analysis (N = 1723; χ2 = 30.18, p < 0.01). Results were similar when we limited psychotic symptoms to those that were found to temporally coincide with the mass murder event, omitting cases in which psychotic symptoms were only present prior to the mass murder: active psychotic symptoms were identified among 5% of mass murderers who used firearms and 15% of those who used other means (χ2 = 33.40, p < 0.01). Results were similar when psychotic symptoms were delineated into delusions/hallucinations (χ2 = 12.52, p < 0.01) and disorganization (χ2 = 19.24, p < 0.01) subtypes.
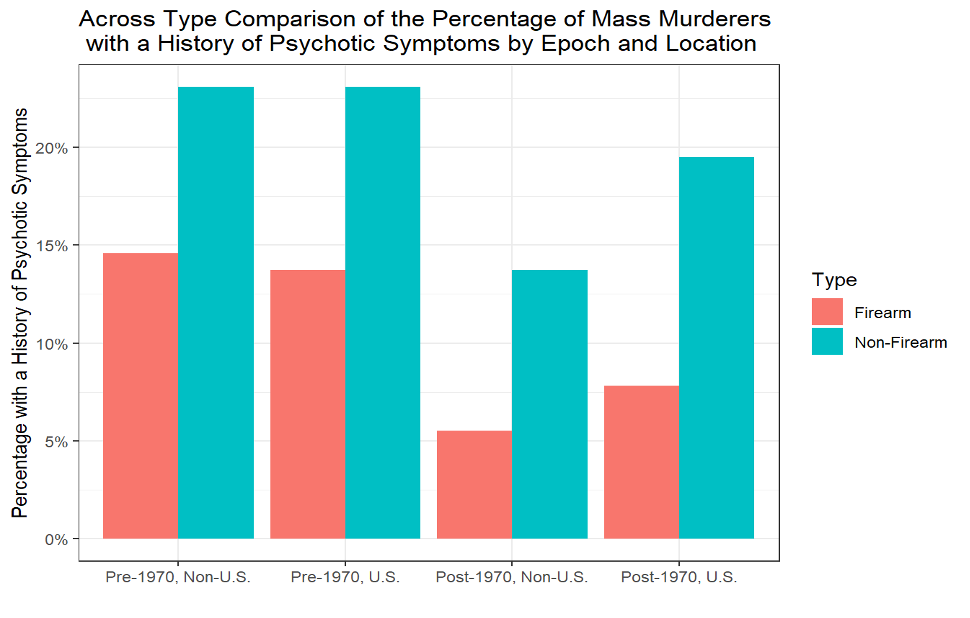
It is possible that differences in diagnostic patterns and increasing awareness and availability of mental health services in more recent decades, compared with earlier in the 20th century, might have confounded rates of psychiatric symptoms observed in this study. Changes in firearm availability and culture, methods used to perpetrate mass murder, or type of firearm used (i.e. non-automatic v. semi- or fully-automatic), when applicable, may also have changed over time. To address these potential limitations in part, we examined the prevalence of psychotic symptoms over time and found that pre-1970 mass murderers had a higher prevalence of persons with psychotic symptoms than the later period (p = 0.005). Nevertheless, the proportions of individuals with a history of psychotic symptoms were higher in the non-firearm group compared to the firearm group in both epochs, inside and outside of the USA. The percentages of mass murderers with a history of psychotic symptoms are pre-1970, non-US firearm 14.58, non-firearm 23.08; pre-1970, US firearm 13.73, non-firearm 23.08; post-1970, non-US firearm 5.52, non-firearm 13.71; post-1970, US firearm 7.83, non-firearm 19.50 (online Supplementary Fig. 2; see also Table 3 and online Supplementary Tables S2 and S4).
Table 3. Description of the sample when limited to only mass shootings post-1970 in the USA

a Differences are assessed using ANOVA for continuous measures and χ2 test for categorical measures.
N/A χ2 test was not a valid test due to low expected cell counts.
The bold values are the significance levels.
Other important differences between mass murderers who did and did not use firearms were observed (Table 1). Mass shooters compared to mass murderers without a firearm were more likely to be male (95% v. 87%; χ2 = 29.1, p < 0.01), Caucasian (55% v. 47%; χ2 = 7.5, p < 0.01) or African American (20% v. 13%; χ2 = 12.7, p < 0.01) and less likely to be Asian (10% v. 29%; χ2 = 75.38, p < 0.01). Mass murderers who used firearms were more likely to have a legal history (24% v. 15%; χ2 = 14.7, p < 0.01), complete suicide at the time of their attacks (31% v. 21%; χ2 = 14.1, p < 0.01), be injured or killed mid-attack by others and kill in the USA (73% v. 43%; χ2 = 116.4, p < 0.01). Similar findings emerged after we mutually controlled for these variables and adjusted for the year in multiple regression, including the association of history of psychotic symptoms with reduced odds of using a firearm v. not using a firearm to commit mass murder. The one exception was that, in the adjusted model, legal history was not significantly related to firearm usage (online Supplement and Supplementary Table S3).
For additional comparisons when the sample was limited to the 734 US-based post-1970 cases, see the online Supplement and Supplementary Table S2.
Mass shootings within and outside the USA
We conducted further analyses to compare mass shootings in the USA v. elsewhere in the world from 1900 to 2019. For these analyses, we included 855 mass shootings, which accounted for 4648 deaths (average 5.4 deaths per event, s.d. = 4.3). A description of the sample is given in Table 4. Mass shooters in the USA had a lower mean victim count (4.8 v. 7.2, p < 0.01). They were also more likely to use recreational drugs or misuse alcohol (χ2 = 9.5, p < 0.01), have a legal history (χ2 = 15.8, p < 0.01), and have symptoms of non-psychotic psychiatric or neurologic disorders (χ2 = 9.0, p < 0.01).
Table 4. Description of the sample when limited to only mass shootings, 1900–2019

a Differences are assessed using ANOVA for continuous measures and χ2 test for categorical measures.
N/A χ2 test was not a valid test due to low expected cell counts.
The bold values are the significance levels.
As fully described in Table 3, the online Supplement and Supplementary Table S4, the average number of fatalities per incident was higher when a semi- or fully-automatic firearm was used [mean 6.4 (5.6) v. 4.8 (3.7); p < 0.01]. The US-based mass shooters were much less likely to use semi- or fully-automatic firearms than those based in other countries (χ2 = 26.6, p < 0.01). Mass shooters using semi- or fully-automatic firearms were more likely to complete suicide at the time of their attacks (χ2 = 5.7, p = 0.02) than those using non-automatic firearms. When the sample was limited to the 431 post-1970 mass shootings based in the USA (Table 3), findings were similar to those in the full sample, except that individuals with symptoms of both psychotic (χ2 = 6.7, p < 0.01) and non-psychotic psychiatric or neurologic illness (χ2 = 5.7, p = 0.02) were more likely to use semi- or fully-automatic weapons when they used firearms to commit mass murder, while the opposite was true for individuals who used drugs or misused alcohol, at trend level (χ2 = 3.4, p = 0.06).
See the online Supplement and Supplementary Tables S5 and S6 for a complete description of the methods used to commit mass murder worldwide and, in the USA.
Discussion
Our study is presented at a time in which various worldwide locations, especially the USA are repeatedly and increasingly convulsed, at random intervals, by mass murder events, typically followed by attributions of blame to people with mental illness and calls for improved screening methods. In reality, while previous research has found severe mental illness to be somewhat overrepresented among those who carry out mass shootings, the most common type of mass murder, it appears to play a significant role in only a small fraction of cases, with the correlation depending on how broadly mental illness is defined (Parks et al., Reference Parks, Bechtold, Shelp, Lieberman and Coffey2019) – that is to say, whether the definition conservatively involves only severe mental illness, such as that characterized by psychotic symptoms, or more widely encompasses psychopathologies such as non-psychotic mood and anxiety disturbances, personality disorders, substance and alcohol use disorders, and maladaptive reactions to adverse life events. Persons with mental illness, moreover, are far more likely to be victims of violence (Hiday, Swartz, Swanson, Borum, & Wagner, Reference Hiday, Swartz, Swanson, Borum and Wagner1999) than to perpetrate it. Unfortunately, previous efforts to explore the potential relationship between mass shootings and mental illness, a topic of considerable public health interest, have been hampered by methodological limitations and inconsistencies.
In accord with our hypothesis, we found that mass murderers who used firearms were significantly less likely to have a lifetime history of psychotic symptoms than mass murderers who use other methods: 18% of mass murderers who did not use firearms had a history of psychotic symptoms, compared to 8% of mass shooters. Our results are consistent with prior reports of rates of mental illness (Parks et al., Reference Parks, Bechtold, Shelp, Lieberman and Coffey2019; Peterson & Densley, Reference Peterson and Densley2019; Silver et al., Reference Silver, Simons and Craun2018; Stone, Reference Stone2015) among mass murderers when the definition is limited to severe psychiatric disturbances, such as those involving psychotic symptoms, and excludes recreational drug use and alcohol use, and symptoms of personality disorders, anxiety and non-psychotic affective disorders. This finding is also consistent with work by Swanson et al. (Reference Swanson, Easter, Robertson, Swartz, Alanis-Hirsch, Moseley and Petrila2016) who reported firearm involvement in just 13% of violent crime arrests among 81 704 adults with serious mental illness in Florida, compared to 24% in the general population of the same counties. Individuals with psychotic symptoms may be less likely to acquire firearms for a number of reasons, including greater disability, lower financial means, less access to social networks that might facilitate firearm acquisition, or disqualification from firearm purchase due to involuntary psychiatric commitment. One might also suggest that persons with psychotic symptoms may, in some instances, be too disorganized to carry out mass shootings, although those with paranoid delusions might be more focused and capable of doing so. Our findings that mass murder perpetrated with means other than firearms are associated with both disorganization and delusions or hallucinations may suggest otherwise. However, persons experiencing only delusional beliefs may demonstrate high levels of functionality and conceal their beliefs well, thereby going undetected by mental health services and being underreported by the media. Future research delineating subtypes of mass murders that involve delusions or hallucinations, which we were unable to examine due to insufficient data, may identify subtypes which are specifically linked with mass murder or method of mass murder. Also, our results do not support or disprove the notion that mass murder is, in general terms, uniquely linked with psychosis, relative to other violent behaviors, since our data focus exclusively on mass murder. Future studies in which mass murder is examined alongside other types of violent behavior, including other types of murder, would allow an informed approach to this important question.
Our definition of mental illness also excluded acute distress following catastrophic life events, such as loss of a job or relationship. Thus, wider definitions – particularly those including legal history, drug use and alcohol misuse, which we found to be significantly more common among mass shooters relative to mass murderers of other types – may imply a stronger association between mental illness and mass murder. This has the potential to exaggerate public and professional belief in the relationship between severe mental illness, characterized by psychotic symptoms and mass shooting events, thereby prompting undue stigmatization and blame of persons with psychotic symptoms following these tragedies. We are unaware of prior research examining the relationship between symptoms of psychiatric/neurologic illness and specific means of carrying out a mass murder and believe that these findings warrant further exploration.
However, persons committing mass murder with means other than firearms were responsible for more fatalities per event and more total fatalities, suggesting murders that are less focused in terms of targets, reflecting the use of methods such as setting fires, explosives, and crashing cars, buses, or trucks to kill passengers or people outside the vehicles. Some such attacks may be impulsive, involving whatever means are immediately available. We note that non-firearm mass murders constitute a highly heterogeneous category, including some methods that carry the potential for large numbers of casualties, such that a small number of these incidents might skew the fatality rate associated with this category.
The relationship between psychiatric symptoms and mass murder may be less associated with psychotic symptoms than with subacute, more common psychopathology, such as depressive symptoms, personality-based symptoms, drug or alcohol use, and reactions to adverse life events. Included here are individuals who, for reasons unrelated to psychosis, may harbor extreme anger or resentment due to feelings of exclusion or social rejection.
One of the primary limitations of this study, and this type of work in general, is the uncertain validity of psychiatric symptoms or diagnoses gleaned from media reports and court/police records. However, in the absence of carefully collected and validated datasets based on prospective analyses of information collected from perpetrators of mass murder and other informants, which do not exist and are difficult to imagine, studies based on media reports and court/police records currently provide the only path towards better understanding the role of psychotic symptoms in mass murders. Another limitation of our findings is the restriction of our dataset to information available in English, which is likely to have underrepresented mass murders in non-English-speaking countries, introducing some degree of sampling bias and reducing the comprehensiveness of our data. Cases identified in our sources may have been more likely to involve psychiatric symptoms, given their news value, or may have involved other unusual elements associated with psychosis, potentially leading to an overestimate of the association with psychotic symptoms. Since our dataset covers more than a century, further potential limitations of this study include possible changes in the prevalence of psychotic symptoms or the attention given to them in media reports over time. Changes in firearm availability and culture, and methods used to perpetrate a mass murder, including types of firearms (i.e. non-automatic v. semi-automatic), may also have affected our findings. To address these limitations, we separately analyzed mass murders during the pre-and post-1970 epochs and observed similar results. There are, however, many other potential sociocultural determinants of mass murder not addressed by the current study, such as firearm laws and secular trends in firearm possession, which warrant further research.
Another limitation is that we found mass murder incidents outside of the USA to be too infrequent to allow for a meaningful statistical comparison of methods with US cases. Cases outside the USA were, indeed, so infrequent that, to permit statistical analyses, we needed to collectively examine non-USA cases according to the regions in which they transpired.
Despite potential limitations, our study reflects several key strengths, including its large dataset, which we believe may now constitute the most comprehensive to date; the use of inferential statistics; inclusion of mass murderers who used means other than firearms, which is an area previously underexplored in the literature; examination of cases from around the globe from 1900 to 2019; and meticulous examination of psychiatric symptom history, wherever available. We believe that our findings may have important implications for a better understanding of what drives mass shootings and shaping policies aimed at preventing them.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291721000076
Acknowledgements
The authors thank Dr Michael H. Stone of Columbia University for reviewing an earlier version of this manuscript. The authors were supported by R01 MH113861 (RRG); New York State Office of Mental Hygiene; and the Elizabeth K. Dollard Charitable Trust.
Conflict of interest
R. Girgis acknowledges research support from Otsuka, Allergan/Forest, BioAvantex and Genentech as well as royalties and/or advances from books on mental health published by Wipf and Stock and Routledge/Taylor and Francis. He has consulted for Noble Insights. Dr Brucato receives royalties and/or advances from the book The New Evil: Understanding the Emergence of Modern Violent Crime and an upcoming book from Routledge/Taylor and Francis. No other authors have disclosures. The sources of funding had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. We were not paid to write this article by a pharmaceutical company or other agency.