


Introduction
This paper addresses the levels of psychological distress experienced in mid-life (at age 42 years) by men and women born in 1958 and 1970. Comparing these cohorts born 12 years apart, we ask whether psychological distress has increased, and, if so, whether this increase can be explained by differences between the cohorts in their childhood conditions, including differences in their social and emotional adjustment during adolescence. While the huge costs to society, and to the economy, of poor mental health are undisputed (Layard, Reference Layard2013), the idea that experiences of mental distress in adulthood are increasing across generations has not been much discussed, and yet if true, is of major societal and population health significance, also considering the effects of population ageing. Younger cohorts in the UK have gained years of life expectancy (Leon, Reference Leon2011; Anonymous, 2015), but if the added years are to be lived healthily, a necessary condition is that they are healthier compared with older cohorts. In order for healthy life expectancy to grow faster than total life expectancy and for morbidity to be compressed, the age-specific prevalence of major drivers of mortality has to be lower in younger cohorts. If not, morbidity will expand and more years will be lived in poor health, a scenario with wide implications for public policy.
A small number of previous studies have noted that psychological distress during adult life has been increasing across cohorts in Britain (Sacker & Wiggins, Reference Sacker and Wiggins2002; Spiers et al. Reference Spiers, Bebbington, Mcmanus, Brugha, Jenkins and Meltzer2011). However, a common feature of these studies is that the cross-cohort equivalence of mental health measures was not established and the reported findings could – at least partly – be attributed to between-cohort differences in the comprehension of items and response tendencies, or other sources of measurement error. In this paper we use the latest available data from the 1970 cohort to compare psychological distress across the 1958 and 1970 cohorts at age 42 years, after formally establishing the equivalence of psychological distress measures in the two cohorts. Second, in acknowledgement that the roots of adult psychological distress often lie in childhood (Power et al. Reference Power, Stansfeld, Matthews, Manor and Hope2002; Krause et al. Reference Krause, Mendelson and Lynch2003; Colman et al. Reference Colman, Ploubidis, Wadsworth, Jones and Croudace2007), we exploit the rich longitudinal data available in these studies since birth and across childhood and attempt to understand whether any observed major differences in childhood conditions between the two cohorts appear to explain differences in psychological distress in mid-life.
Method
Sample
The National Child Development Study (NCDS) follows the lives of 17 416 people born in England, Scotland and Wales in a single week of 1958 (Power & Elliott, Reference Power and Elliott2006). Also known as the 1958 Birth Cohort Study, it collects information on physical and educational development, economic circumstances, employment, family life, health behaviour, wellbeing, social participation and attitudes. Since the birth survey in 1958, there have been 10 further surveys of all cohort members at ages 7, 11, 16, 23, 33, 42, 44, 46, 50 and 55 years. Despite attrition, the study remains largely representative of the original sample (Hawkes & Plewis, Reference Hawkes and Plewis2006). At age 42 years 11 419 participants (65.5% of the original productive sample) took part in the survey. The 1970 British Cohort Study (BCS70) follows the lives of 16 569 people born in England, Scotland and Wales in a single week of 1970 (Elliott & Shepherd, Reference Elliott and Shepherd2006). In 2012 at age 42 years 9354 study members participated in the survey (56.45% of the original sample). Despite attrition the study remains representative of the original sample's characteristics (Mostafa & Wiggins, Reference Mostafa and Wiggins2015). Over the course of cohort members’ lives, the BCS70 has collected information on health, physical, educational and social development, and economic circumstances among other factors. Since the birth survey in 1970, there have been eight surveys at ages 5, 10, 16, 26, 30, 34, 38 and 42 years. Our analytic sample included participants that had at least four valid – not missing – responses on the Malaise Inventory at age 42 years (n = 9976 women and n = 9270 men). This limited the presence of participants with missing data due to item non-response to <5% of the overall sample. We employed multiple imputation with a conditional specification and derived 20 imputed datasets using all variables (year of birth, hypothesized mediators and outcome) in the imputation process as has been suggested in the literature (Carpenter & Kenward, Reference Carpenter and Kenward2012) to impute missing data in the hypothesized mediators and the <5% of the analytic sample that was missing on the outcome. Multiple imputation operates under the missing at random assumption (Little & Rubin, Reference Little and Rubin2002), which in this case implies that our estimates are valid if missingness is due to variables included in our models.
Measures
Outcome
Psychological distress was measured by self-report at age 42 years in both cohorts using the nine-item version of the Malaise Inventory (Rutter et al. Reference Rutter, Tizard and Whitmore1970; Rodgers et al. Reference Rodgers, Pickles, Power, Collishaw and Maughan1999). In both surveys the Malaise items were assessed via written self-completion, by the 1970 cohort on paper, and by the 1958 cohort via computer. More information on the administration of the Malaise Inventory in the two surveys is available in online Supplementary Appendix SI. Representative items enquire whether the participants often ‘feel miserable and depressed’, ‘get worried about things’ and ‘get easily upset or irritated’. The Malaise Inventory has been shown to have good psychometric properties (McGee et al. Reference McGee, Williams and Silva1986) and has been used in general population studies as well as investigations of high-risk groups (Furnham & Cheng, Reference Furnham and Cheng2015). In both studies at age 42 years the nine-item version has very good reliability as indicated by the Kuder–Richardson-20 (KR20) formula (Kuder & Richardson, Reference Kuder and Richardson1937): KR20NCDS = 0.77 and KR20BCS70 = 0.79. The nine-item version correlates highly with the 24-item version (r NCDS = 0.91 at age 42 years and r BCS70 = 0.92 at age 30 years). Descriptive statistics of the prevalence of psychological distress symptoms indicated by positive responses in the nine items of the Malaise Inventory are presented in Table 1.
Table 1. Prevalence of psychological distress symptoms indicated by positive responses in the nine items of the Malaise Inventory
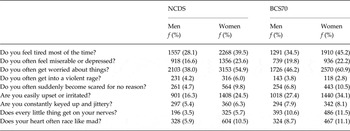
NCDS, National Child Development Study; BCS70, 1970 British Cohort Study.
Mediators
The mediators we included in our analysis were divided into four groups, birth characteristics, parental characteristics, child characteristics and adult characteristics. All hypothesized early-life mediators that are described below have been shown to influence adult mental health in the NCDS and other longitudinal studies (Robins & Price, Reference Robins and Price1991; Rutter, Reference Rutter1995; Power et al. Reference Power, Stansfeld, Matthews, Manor and Hope2002; Colman et al. Reference Colman, Ploubidis, Wadsworth, Jones and Croudace2007). The birth characteristics included in the models were birth weight (‘normal’ ⩾2500 g v. ‘low’ <2500 g), maternal smoking during pregnancy and breastfeeding (ever breastfed and breastfed for more than 1 month). The parental characteristics were paternal social class at age 10 years for the BCS70 and 11 years for the NCDS (manual v. non-manual), whether the mother of the participants was employed (birth to age 5 years), divorce (by age 10 years), and years of education of both parents of the participants. The child characteristics we included in the analysis were nocturnal enuresis (wet at night after age 5 years) and the Rutter mental health assessment at age 16 years, using the same modified version of the Rutter ‘A’ scale (Rutter et al. Reference Rutter, Tizard and Whitmore1970) in both cohorts. This version of the scale was completed by the mothers of the participants in both cohorts as part of the home interview. It generates an overall behavioural adjustment score in addition to four subscales: conduct problems, hyperactivity, emotional and peer problems. Although not the main focus of this paper, we also included some adult characteristics that vary between the two cohorts (Ferri et al. Reference Ferri, Bynner and Wadsworth2003) and have also been linked to psychological distress (Prince et al. Reference Prince, Beekman, Deeg, Fuhrer, Kivela, Lawlor, Lobo, Magnusson, Meller, Van Oyen, Reischies, Roelands, Skoog, Turrina and Copeland1999; Miech et al. Reference Miech, Power and Eaton2007; Paul & Moser, Reference Paul and Moser2009). These were: participants’ highest education at age 33 years, partnership status at age 33 years, number of children by age 42 years and employment status at age 33 years.
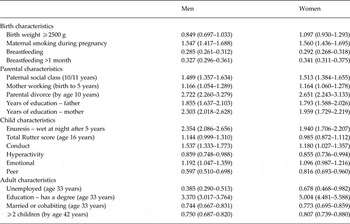
Descriptive statistics of all mediators in our analysis stratified by cohort and gender are presented in Table 2. Some maternal health behaviours deteriorated between the 1958 and 1970 cohorts. The proportion of children who were never breastfed roughly doubled from 31–32% in the 1958 cohort to 63–64% in the 1970 cohort. Smoking during pregnancy rose from 34% to 46%. The proportion of children experiencing parental divorce by age 10 years increased from 5% in the earlier cohort to 11–12% in the later cohort. Bed-wetting after the age of 5 years rose from 10% of girls and 12% of boys in the 1958 cohort to 18% of girls and 25% of boys in the 1970 cohort. A modest increase was observed in the overall Rutter behavioural adjustment score, as well as in conduct and emotional problems. In adulthood, key changes are a substantial increase in educational levels, with 11% of women and 14% of men having a degree by age 33 years in the 1958 cohort, rising to 37% of women and 34% of men in the 1970 cohort, and a decline in those living with a partner (defined as cohabitation including marriage) from 78–80% to 74–76% at age 33 years. In Table 3 we present the odds ratios (ORs) and corresponding 95% confidence intervals (CIs) of the associations (direct effects) between year of birth (cohort dummy variable) and all hypothesized mediators.
Table 2. Descriptive statistics of all hypothesized mediators

Data are given as percentage.
NCDS, National Child Development Study; BCS70, 1970 British Cohort Study.
Table 3. Association (direct effect) between year of birth and the hypothesized mediators
Data are given as odds ratio (95% confidence interval).
Statistical analysis
Measurement invariance
We modelled the probability of response to the binary Malaise Inventory items with a two-parameter probit unidimensional latent variable measurement model (Muthén, Reference Muthén1984; Rabe-Hesketh & Skrondal, Reference Rabe-Hesketh and Skrondal2008). The general form of the measurement model is presented in online Supplementary Appendix SII. In order to obtain a meaningful comparison between the NCDS and BCS70 with respect to psychological distress, strong measurement invariance between the two cohorts has to be established (Meredith, Reference Meredith1993). This implies that the measurement parameters of the model need to function equivalently between the two cohorts and gender in order for the latent psychological distress means to be comparable. To empirically test this assumption and control for systematic sources of measurement error that may arise in between-cohort and/or between-gender comparisons, from differences in the comprehension of items, in response tendencies or random sources of error, we estimated a multigroup confirmatory factor analysis, where measurement model parameters, in this instance factor loadings and thresholds, were not allowed to vary between the two cohorts as well as gender. In the literature this type of invariance is usually referred to as scalar or strong invariance and is the only form of invariance that allows the comparison of latent means (Meredith, Reference Meredith1993; Muthén & Asparouhov, Reference Muthén and Asparouhov2002, Reference Muthén and Asparouhov2013).
Causal mediation analysis
Preliminary results showed strong evidence of effect modification by gender of the association between year of birth and psychological distress (results available from corresponding author; G.B.P.). We thus report results separately for each gender. In order to quantify the association between year of birth and psychological distress we estimated a stratified by gender multiple causes multiple indicators (MIMIC) model using the already established invariant model of the Malaise Inventory as the outcome and year of birth (1958 v. 1970) as the predictor. In the final stage of the analysis and in order to investigate whether early-life experiences and behavioural adjustment until age 16 years account for between-cohort differences in psychological distress at age 42 years we extended the MIMIC model to include mediators. The indirect effect of year of birth captures the proportion of the between-cohort difference in psychological distress that is due to – or is transmitted by – the intermediate variables (‘mediators’). In the causal mediation literature several approaches have been proposed for the estimation of direct and indirect effects with an emphasis on different aspects of mediation (Ten Have & Joffe, Reference Ten, ve and Joffe2012). In this instance we report natural indirect effects (NIEs) that evaluate the action of potential mediating mechanisms and have been shown to be appropriate for the quantification of mediation effects in non-linear systems (Pearl, Reference Pearl, Breese and Koller2001; Myers, Reference Myers2003; Robins, Reference Robins, Green, Hjort and Richardson2003; Imai et al. Reference Imai, Keele and Tingley2010, Griffiths et al. Reference Griffiths, Cortina-Borja, Sera, Pouliou, Geraci, Rich, Cole, Law, Joshi, Ness, Jebb and Dezateux2013, Valeri & VanderWeele, Reference Valeri and Vanderweele2013; Muthén & Asparouhov, Reference Muthén and Asparouhov2015). Our approach allowed the computation of formal mediation estimates (NIEs) while simultaneously controlling for measurement error in psychological distress. Directed acyclic graphs that further clarify our model specification strategy are presented in online Supplementary Appendix SIII.
All our models were estimated with Mplus 7.4 (Muthén & Muthén, Reference Muthén and Muthén1998–2015). The multigroup measurement model was estimated with the weighted least squares, mean and variance adjusted (WLSMV) estimator with delta parameterization (results with the alternative theta parameterization were very similar, available from the corresponding author; G.B.P.). Stratified by gender MIMIC models were estimated as mixture models with the ‘known class’ option, with the robust maximum likelihood ratio (MLR) estimator with Monte Carlo integration (200 integration points).
Results
Between-cohort and -gender measurement invariance of the Malaise Inventory at age 42 years
The multigroup confirmatory factor analysis model representing strong (scalar) invariance had very good fit [comparative fit index (CFI) = 0.984, Tucker Lewis index (TLI) = 0.982, root mean square error of approximation (RMSEA) = 0.037, 95% CI 0.035–0.039], indicating the measurement equivalence of the Malaise Inventory in the four groups (two cohorts by two genders). A less restrictive multigroup model representing configural invariance (factor loadings and thresholds freely estimated) had only minimally better fit (CFI = 0.987, TLI = 0.982, RMSEA = 0.037, 95% CI 0.035–0.040). The difference (Δ) in model fit was well within the criteria for not rejecting the null hypothesis of invariance (ΔCFI < 0.01, ΔRMSEA < 0.015 and overlapping RMSEA CIs), further reinforcing our interpretation (Cheung & Rensvold, Reference Cheung and Rensvold2002; Sass, Reference Sass2011). The standardized factor loadings (λ i ) of the multigroup model representing scalar invariance were all satisfactory and ranged between 0.600 and 0.894, whereas the item thresholds (τ i ) were mostly located as expected towards the high end of the latent psychological distress continuum (−0.116 to 1.605). The parameters of all models and model fit criteria are presented in online Supplementary Appendix SII. The very good fit of the multigroup model with identical measurement parameters across the four groups and the minimal difference in model compared with less restrictive models suggest that the comprehension of items and response tendencies can be assumed to be uniform between cohorts as well as genders and therefore cohort and gender differences in latent psychological distress can be attributed to valid variation.
Between-cohort differences in psychological distress at age 42 years
Once measurement invariance was established, we proceeded to estimate the total effect of the cohort dummy variable encoding year of birth (1958 or 1970) on psychological distress (between-cohort differences) at age 42 years. For comparison purposes with other studies, we report results from models on three versions of the outcome: the latent variable derived from the measurement invariant model, the sum score (nine-point Malaise scale) and a binary version that captures participants that have scored >3. Descriptive statistics of the sum and binary versions are presented in Table 4. Amongst those born in 1958, women were considerably more likely to be defined as showing signs of psychological distress at 42 years than men (16% compared with 10%). Measured 12 years later, among those born in 1970 at age 42 years, levels of psychological distress were higher among both men and women, and although it remained the case that women were more likely to show signs of psychological distress than men, a larger increase in levels of distress amongst men born in 1970 compared with in 1958 led to the difference between men and women being reduced between the two cohorts (20% of women compared with 16% of men). In men, the BCS70 cohort scored b = 0.314 (95% CI 0.252–0.375) standard deviations higher on the latent psychological distress variable, b = 0.419 (95% CI 0.342–0.495) points higher on the nine-point Malaise scale and were more likely compared with the NCDS cohort to score more than 3 on the Malaise Inventory (OR 1.788, 95% CI 1.577–2.026). As expected from the descriptive statistics, the between-cohort difference in psychological distress was less pronounced in women. Women born in 1970 scored b = 0.147 (95% CI 0.076 to 0.218) standard deviations higher on the latent score, b = 0.253 (95% CI 0.176–0.330) higher on the nine-point Malaise score and were more likely to score more than 3 on the Malaise Inventory (OR 1.299, 95% CI 1.172–1.440).
Table 4. Summary descriptive statistics of the Malaise Inventory

CI, Confidence interval.
Associations between mediators and psychological distress
In Table 5 we present latent regression parameters and corresponding 95% CIs of the association between each mediator and the between-cohort invariant psychological distress outcome. The associations between the mediators and the outcome were similar in magnitude in both cohorts and in the expected direction. For example, the total score as well as the dimensions of the Rutter scale were as expected strongly and positively associated with psychological distress at age 42 years in both cohorts. On the contrary, having a university degree had a strong negative association with psychological distress in men and women of both cohorts. Exceptions to the between-cohort homogeneity of the mediator–outcome associations were the differences in magnitude observed in the associations between parental and maternal education, as well as unemployment at age 33 years with psychological distress. When formally tested, we obtained weak evidence of interaction between the mediators and year of birth.
Table 5. Association (direct effects) between the hypothesized mediators and latent psychological distress at age 42 years
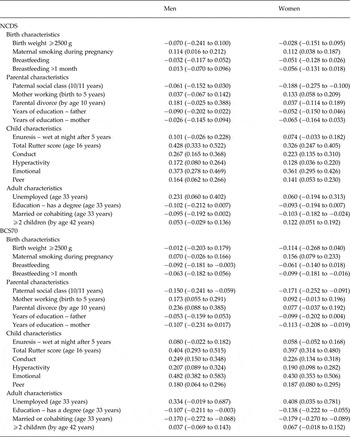
Data are given as latent regression parameter b (95% confidence interval).
NCDS, National Child Development Study; BCS70, 1970 British Cohort Study.
Mediation
In Table 6, we present the total effect of the cohort dummy that encodes year of birth on psychological distress at age 42 years and the NIEs for all hypothesized mediators. In both men and women some NIEs were positive while others were negative. The presence of negative NIEs, as for example the NIE for the mediating effect of having a university degree in women, b = −0.032 (95% CI −0.048 to −0.015), is evidence for inconsistent mediation or regression suppression (MacKinnon et al. Reference MacKinnon, Krull and Lockwood2000; Maassen & Bakker, Reference Maassen and Bakker2001; Friedman & Wall, Reference Friedman and Wall2005). Similarly, paternal social class, paternal and maternal education, peer problems and being unemployed at age 33 years were all also found to be inconsistent mediators. We note that inconsistent mediators or suppressors do not explain the observed difference between cohorts, as consistent mediators do. On the contrary, they might inflate the observed difference when they are included in the model, or ‘suppress’ it when they are excluded. For example the observed difference of b = 0.147 (95% CI 0.076–0.218) between the two cohorts in women increases to b = 0.206 (95% CI 0.150–0.261) when women's education at age 33 years is included in the model. Intuitively, this can be explained as follows – psychological distress is higher among the BCS70 cohort than the NCDS cohort, despite the increase in education among the younger cohort, which in itself is associated with lower psychological distress.
Table 6. Natural indirect effects
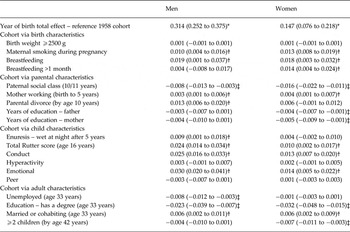
Data are given as standardized latent regression parameters b (95% confidence interval).
* p < 0.01.
† Significant consistent mediating effect (p < 0.001).
‡ Significant inconsistent mediating effect (p < 0.001).
In men, maternal smoking during pregnancy and ever being breastfed were consistent mediators of the association between year of birth and adult psychological distress that reached conventional levels of statistical significance (b = 0.010, 95% CI 0.004 to 0.016) and b = 0.019 (95%CI = 0.001 − 0.037). Similarly, parental divorce at age 10 years (b = 0.013, 95% CI 0.006–0.020) was the only parental characteristic with a consistent mediating effect in men. Among child characteristics, conduct and emotional problems both consistently mediated the association between year of birth and psychological distress (b = 0.025, 95% CI 0.016–0.033; and b = 0.030, 95% CI 0.020–0.041), as did the total score of the Rutter scale (b = 0.024, 95% CI 0.014–0.034). Partnership status at 33 years was the only adult characteristic with a consistent mediating effect (b = 0.006, 95% CI 0.002–0.011). In women, maternal smoking during pregnancy, ever breastfed as well as breastfeeding for more than 1 month were consistent mediators (b = 0.013, 95% CI 0.008–0.019; b = 0.018, 95% CI 0.003–0.032; and b = 0.014, 95% CI 0.004–0.024, respectively). Maternal employment by age 5 years (b = 0.004, 95% CI 0.001–0.007) was the only parental characteristic with a consistent mediating effect in women. We found that conduct and emotional problems at 16 years and general behavioural adjustment as captured by the total score of the Rutter scale at the same age were consistent mediators (b = 0.013, 95% CI 0.007–0.020; b = 0.014, 95% CI 0.005–0.022; and b = 0.010, 95% CI 0.002–0.017). With respect to adult characteristics, partnership status at 33 years was found to be a consistent mediator (b = 0.006, 95% CI 0.002–0.009).
Discussion
We observed differences in psychological distress between the 1958 (NCDS) and 1970 (BCS70) cohorts at age 42 years. Men and women born in 1970 report more psychological distress symptoms than those born in 1958, but the observed differences were more pronounced in men, with the magnitude of the year of birth effect being almost twice as strong compared with women. The establishment of between-cohort measurement invariance of the Malaise Inventory implies that the observed differences were due to valid between-cohort variation in levels of psychological distress and not an artefact of cohort differences in random or systematic sources of measurement error such as response style, item comprehension and social desirability. This implies that the passage of 12 years has not differentially affected the interpretation of the survey questions that comprise the Malaise Inventory. A common bias might still have influenced the location of the latent mean of psychological distress equally in both cohorts, but not the magnitude of the observed difference. This relatively large difference in levels of psychological distress was observed despite the protective effect of the generally improved social and economic conditions that the 1970 cohort enjoyed, compared with the 1958 and older cohorts (Ferri et al. Reference Ferri, Bynner and Wadsworth2003). Our formal approach to mediation allowed us to empirically capture this protective effect in the form of ‘inconsistent mediation’ or ‘regression suppression’ (MacKinnon et al. Reference MacKinnon, Krull and Lockwood2000; Maassen & Bakker, Reference Maassen and Bakker2001; Friedman & Wall, Reference Friedman and Wall2005), a finding that would have been overlooked if standard methods were employed.
The observation that the 1970 cohort have higher levels of psychological distress compared with an earlier-born cohort in midlife has implications for public health policy, especially considering that depression is one of the leading causes of disability-adjusted life years worldwide (Ferrari et al. Reference Ferrari, Charlson, Norman, Patten, Freedman, Murray, Vos and Whiteford2013). Taking into account that due to increases in life expectancy younger (more recently born) cohorts are expected to live longer, a necessary condition for compression of morbidity – in order for the added years to be lived healthily – is that controlling for age differences (or at a fixed age as in our paper), more recently born cohorts are healthier, so the average onset of morbidity is postponed (Fries, Reference Fries1980; Fries et al. Reference Fries, Bruce and Chakravarty2011). On the contrary, expansion of morbidity will occur if younger cohorts are less healthy, whereas similar health levels between cohorts will most probably lead to equilibrium or mild expansion of morbidity (Gruenberg, Reference Gruenberg1977; Manton, Reference Manton1982; Olshansky et al. Reference Olshansky, Rudberg, Carnes, Cassel and Brody1991). Our observation of a higher average level of psychological distress in the 1970 cohort at age 42 years increases the likelihood of expansion of mental health-related morbidity, assuming that the observed difference will persist in the future. Therefore, unless as both cohorts age, those born in 1958 catch up and surpass the 1970 cohort on average levels of psychological distress, our findings imply that the average onset of mental health-related morbidity will not be postponed in the 1970 cohort.
A reversal of the observed differences in the future, so that the 1958 cohort experiences higher levels of psychological distress, appears – in theory – not likely. First, the association between age and mental health outcomes is complex, but arguably weak (Prince et al. Reference Prince, Beekman, Deeg, Fuhrer, Kivela, Lawlor, Lobo, Magnusson, Meller, Van Oyen, Reischies, Roelands, Skoog, Turrina and Copeland1999; Jorm et al. Reference Jorm, Windsor, Dear, Anstey, Christensen and Rodgers2005; Yang, Reference Yang2007; Wu et al. Reference Wu, Schimmele and Chappell2012). Furthermore, a very strong association between early-life behavioural adjustment, mid-life mental health and later-life depression has been reported in the literature (Robins & Price, Reference Robins and Price1991; Rutter, Reference Rutter1995; Lara et al. Reference Lara, Fayyad, De Graaf, Kessler, Aguilar-Gaxiola, Angermeyer, Demytteneare, De Girolamo, Haro, Jin, Karam, Lepine, Mora, Ormel, Posada-Villa and Sampson2009). Lastly, the 1970 cohort reported higher levels of psychological distress than the 1958 cohort also at age 33 years (Sacker & Wiggins, Reference Sacker and Wiggins2002), as well as at age 16 years as we have shown in this paper. Both findings imply a relatively stable trend in between-cohort differences over time.
We attempted to explain the observed between-cohort variation by investigating the explanatory power of ‘consistent’ mediators (rather than ‘inconsistent mediators’ or ‘suppressors’) focusing on early-life characteristics and behavioural adjustment. The magnitude of the effect of all early-life consistent mediators was modest in both men and women. In men the observed between-cohort differences were mostly due to breastfeeding and behavioural adjustment at age 16 years, with the 1970 cohort less likely to have been breastfed, and reporting more conduct and emotional problems which were related to higher levels of psychological distress at 42 years. The between-cohort increase in parental divorce and in maternal smoking during pregnancy also explain the increase in psychological distress between cohorts in men, but less prominently. In women, birth characteristics, such as ever being breastfed, breastfed for more than 1 month and maternal smoking during pregnancy, along with conduct and emotional problems in adolescence were the strongest consistent mediators of the association between year of birth and psychological distress at 42 years. Similarly with the early-life characteristics, the adult social and demographic factors that were included in our study did not explain a substantial fraction of the association between year of birth and psychological distress. Partnership status at 33 years was the only consistent mediator in both men and women, such that the decline in cohabiting and married relationships by age 33 years in the 1970 cohort has contributed to increased distress levels at age 42 years.
Strengths of this study are the availability of two population-based birth cohorts with various measures taken at the same stages of the life course, our modelling strategy that allowed us to establish measurement invariance/equivalence across the two cohorts and the computation of formal mediation estimates while simultaneously controlling for measurement error. Limitations include our reliance on self-reported data in the assessment of psychological distress. Despite our efforts, common to both cohorts random or systematic error could have influenced the location of the latent psychological distress means, but not the observed differences between those means. Furthermore, we assumed an identical missing data-generating mechanism in both cohorts, which implies that an identical set of observables (year of birth, all the mediators and the outcome in this instance) are responsible for missing data in both studies. It should also be noted that the BCS70 had a higher prevalence of missing data in both mediators and the outcome. Taking into account that by definition the only ‘complete’ (without missing data) variable in our analysis was year of birth, it follows that as more missing data in the mediators and outcome are included the observed between-cohort difference tends to marginally increase. We report estimates allowing only a small fraction of missing data in the outcome in our models, and note that similar results were obtained in analyses with varying missing data inclusion criteria, including imputation of all missing data (including unit non-response) in the outcome and the hypothesized mediators (results available from corresponding author G.B.P.).
Our results showcase the association between year of birth and psychological distress, but our analysis could not disentangle whether the observed difference is due to ‘cohort’ or ‘period’ effects (Keyes et al. Reference Keyes, Utz, Robinson and Li2010), since only one time point was considered. However, it is well known that even in studies with more time points, age–period–cohort models cannot be identified without added constraints, since no statistical model can simultaneously estimate age, period and cohort effects because of the collinearity among these variables (Keyes et al. Reference Keyes, Utz, Robinson and Li2010). We note that establishing the association between year of birth and psychological distress is sufficient as an empirical test of compression of morbidity. Understanding whether the association between year of birth and psychological distress is due to ‘cohort’ or ‘period’ effects is a further step beyond the scope of this paper, which – under assumptions – would provide us with valuable insights on the mechanism that underlies the observed association between year of birth and psychological distress.
Although not explicitly of interest in our study, the associations between the various mediators and year of birth may result in intermediate confounding (De Stavola et al. Reference De Stavola, Daniel, Ploubidis and Micali2015). Further analyses showed that our results are unlikely to be biased by the presence of intermediate confounders (see online Supplementary Appendix SII for further discussion). Another limitation is that our estimates depend on the assumption of no omitted variables/unmeasured confounders, which is we believe reasonable for the year of birth–mediators and year of birth–psychological distress associations. However, mediator–outcome confounding is possible.
Overall, we find that despite the secular changes that resulted in important differences between the two cohorts in early-life characteristics, these account for a modest fraction of the between-cohort variation in psychological distress at age 42 years. This finding indicates that other factors in early adulthood and mid-life are responsible for the observed between-cohort differences. The observed increase in the levels of psychological distress experienced by people in mid-life in Britain has major policy implications, given that the increase has occurred despite economic growth. The 1958 cohort is part of the ‘lucky generation’ of post-war baby boomers, who experienced high absolute levels of social mobility, and lower levels of social inequality in their early lives, whereas the 1970 cohort are part of ‘Generation X’, who have experienced greater uncertainty and insecurity over the whole of their adult lives and a more individualistic ideological climate (Sullivan et al. Reference Sullivan, Brown and Bann2015). If these generational changes lie behind the increase in psychological distress, then we would predict that future generations will be worse off still if such trends were to continue. An alternative explanation is that the elevated levels of psychological distress in the 1970 cohort at age 42 years were mostly due to the social context at the timing of the interview. The year 2012 was a post-recession year with austerity measures already being in place in the UK. This is in stark comparison with 2000 – when the 1958 cohort were aged 42 years – that can generally be described as a post-millennial year of cultural and economic boom. The unemployment rate in 2000 fluctuated between 5.2% and 5.5%, whereas in 2012 it had increased to 8.1%. Furthermore, previous studies suggest that recessions are expected to affect men more severely (Hoynes et al. Reference Hoynes, Miller and Schaller2012; Katikireddi et al. Reference Katikireddi, Niedzwiedz and Popham2012) and unemployment has been linked to poor mental health in both men and women (Gallo et al. Reference Gallo, Bradley, Siegel and Kasl2000; Booker & Sacker, Reference Booker and Sacker2012). Nevertheless, we believe that it is not plausible that the increase in psychological distress between the 1958 and 1970 cohorts at age 42 years is largely due to a time of interview/period effect, as a similar cross-cohort increase in psychological distress was observed in this study in adolescence and has also been found in earlier adulthood (Sacker & Wiggins, Reference Sacker and Wiggins2002).
In future work we will employ more time points to capture adult trajectories of mental health and to establish whether the elevated level of psychological distress in the 1970 cohort represents a general trend in more recently born cohorts. We will also consider what other factors – especially in adulthood – may explain the observed between-cohort difference. Furthermore, the fact that men appear to be closing the gap on women's historically higher levels of psychological distress is also troubling, and demands further investigation.
Supplementary material
The supplementary material for this article can be found at http://dx.doi.org/10.1017/S0033291716002464
Acknowledgements
This research was conducted under the auspices of the Cross-Cohort Research Programme and was funded by the Economic and Social Research Council (grant number ES/M008584/1).
Declaration of Interest
None.








