Introduction
People who are trans (transgender) or gender diverse have a gender incongruent with the sex assigned to them at birth. In recent years, there has been an increase in the prevalence of trans and gender diverse (TGD) young people, evidenced through population-based studies and the higher number of young people seeking gender-affirming interventions at gender clinics worldwide (Cohen-Kettenis et al., Reference Cohen-Kettenis, Steensma and de Vries2011; Telfer et al., Reference Telfer, Tollit and Feldman2015). The number of trans and gender non-conforming young people in the population is currently estimated to be almost 2.7% of adolescents (Rider et al., Reference Rider, McMorris, Gower, Coleman and Eisenberg2018), higher than previous population estimates of 0.5–1.2% (Telfer et al., Reference Telfer, Tollit and Feldman2015; Winter et al., Reference Winter, Diamond, Green, Karasic, Reed, Whittle and Wylie2016; Flores et al., Reference Flores, Herman, Brown and Conron2017).
Research on the mental health of TGD populations tends to be conflated with research into LGBTIQ (lesbian, gay, bisexual, trans, intersex and queer) groups broadly. However, gender and sexuality are two very distinct aspects of a person's identity. LGBT (lesbian, gay, bisexual and trans) young people do experience poorer mental health than the general population, but these rates of poor mental health are even higher rates for trans youth compared to their lesbian, gay and bisexual peers (Hillier et al., Reference Hillier, Jones, Monagle, Overton, Gahan, Blackman and Mitchell2010; Veale et al., Reference Veale, Watson, Peter and Saewyc2017). It has been established that trans populations experience higher rates of poor mental health than their cisgender peers – those whose gender identity matches the sex assigned to them at birth (Bouman et al., Reference Bouman, Claes, Brewin, Crawford, Millet, Fernandez-Aranda and Arcelus2017; Veale et al., Reference Veale, Watson, Peter and Saewyc2017; Rider et al., Reference Rider, McMorris, Gower, Coleman and Eisenberg2018). Previous research shows that children who are gender non-conforming in childhood are more likely to experience depression through adolescence and young adulthood compared to those who are gender conforming, in part attributable to adverse life events such as increased exposure to bullying and child abuse (Roberts et al., Reference Roberts, Rosario, Slopen, Calzo and Bryn Austin2013). Reisner et al. (Reference Reisner, Vetters, Leclerc, Zaslow, Wolfrum, Shumer and Mimiaga2015) found that, in comparison to cisgender controls, trans young people experienced a two to threefold greater risk of anxiety disorders and depression.
Suicide attempts are relatively common in young trans populations – 37.8% of trans young people (aged 19–25) in Canada and 45% of trans adolescents in the UK have attempted suicide (Bradlow et al., Reference Bradlow, Bartram, Guasp and Jadva2017; Veale et al., Reference Veale, Watson, Peter and Saewyc2017). TGD young people are significantly more likely than cisgender youth (regardless of sexuality) to self-harm and attempt suicide (Jones and Hillier, Reference Jones and Hillier2013; Smith et al., Reference Smith, Jones, Ward, Dixon, Mitchell and Hillier2014; Reisner et al., Reference Reisner, Vetters, Leclerc, Zaslow, Wolfrum, Shumer and Mimiaga2015; Testa et al., Reference Testa, Michaels, Bliss, Rogers, Balsam and Joiner2017). For example, trans young people are more likely to experience suicidal thoughts (31% compared to 11%) and to attempt suicide (17.2% compared to 6.1%) in comparison to matched cisgender controls (Reisner et al., Reference Reisner, Vetters, Leclerc, Zaslow, Wolfrum, Shumer and Mimiaga2015). Causes of suicidal ideation and risk in TGD populations are likely to be multifactorial, including being attributable to minority stress, transphobia and life crises (McDermott et al., Reference McDermott, Hughes and Rawlings2017; Testa et al., Reference Testa, Michaels, Bliss, Rogers, Balsam and Joiner2017). A previous national study of the mental health of TGD young people in Australia (n = 189) reported that, of the participants who had been exposed to abuse or discrimination, 70% had self-harmed and 37% had attempted suicide (Smith et al., Reference Smith, Jones, Ward, Dixon, Mitchell and Hillier2014). A history of physical and/or sexual violence has been associated with suicidal thoughts and attempts in adult trans populations (Testa et al., Reference Testa, Hendricks, Goldblum and Bradford2012).
There are multiple and interacting factors contributing to mental health difficulties in this population. Previous research has indicated that trans populations may experience additional stress in a variety of situations (such as bathrooms and identification documents not matching gender expression) stemming from the expectation of rejection (Rood et al., Reference Rood, Reisner, Surace, Puckett, Maroney and Pantalone2016). LGBT youth who experience peer victimisation experience higher levels of depressive symptoms, and have a lower sense of belonging within schools (Collier et al., Reference Collier, van Beusekom, Bos and Sandfort2013). As a young person's gender non-conformity increases, so too do their likelihood of being bullied (Gordon et al., Reference Gordon, Conron, Calzo, White, Reisner and Austin2018).
There has been limited research on the mental health of TGD young people within Australia. In particular, the impact of negative and/or traumatic events on mental wellbeing in this population has not been extensively examined (Reisner et al., Reference Reisner, Poteat, Keatley, Cabral, Mothopeng, Dunham, Holland, Max and Baral2016). The only previous national study of Australian TGD young people reported on some aspects of mental health but did not investigate the associations between potential drivers of poor mental health, such as discrimination and bullying, and adverse health outcomes; e.g. self-harm, suicidality and psychiatric diagnoses (Smith et al., Reference Smith, Jones, Ward, Dixon, Mitchell and Hillier2014). The earlier study focussed on suicide and self-harm after exposure to violence, but not wider patterns and predictors. This limits our understanding of why TGD young people experience elevated rates of mental health difficulties and constrains our ability to develop and implement appropriate intervention strategies (Reisner et al., Reference Reisner, Poteat, Keatley, Cabral, Mothopeng, Dunham, Holland, Max and Baral2016). This study aims to characterise mental health issues affecting TGD Australian young people, and to investigate the potential relationships between negative life events and adverse mental health outcomes.
Methods
Study population
The survey sample comprised 859 young people aged 14–25 years who self-identified as trans or gender diverse (TGD) and were currently residing in Australia between February and August 2016.
Study design
An online cross-sectional survey was undertaken. TGD young people and parents of TGD young people were consulted to determine their preferences for questions to be included in the survey, and to ensure that the questions were relevant and asked in a respectful manner. We held a focus group with TGD young people and a separate focus group with parents of TGD young people. These groups were provided with an initial draft of the questionnaire and the final version was shaped by their feedback from these sessions. The focus group members identified drivers and protective factors of mental health based on their own experiences and awareness of concerns raised within the community. Qualtrics online survey software was used to construct and host the questionnaire which utilised branch, display and skip logic based on participant responses. All questions were optional, except those used to determine eligibility (i.e. TGD identification, age, place of residence).
Recruitment and consent procedures
An anonymous online, self-report questionnaire was conducted between February and August 2016. Participants were largely recruited using social media (i.e. Twitter, Facebook and Tumblr), gender clinics, youth mental health services, support groups, parent and youth groups, and word of mouth. Participants were provided with an online participant information sheet and were instructed that by entering the online survey they were consenting to take part in the study. Parental consent was not required. The study was approved by the University of Western Australia ethics committee (RA/4/1/7958).
Outcomes and risk factors of interest
The questionnaire included both quantitative and qualitative components. Primary outcomes of interest were self-reported psychiatric diagnoses, adverse health outcomes, and current anxiety and depressive symptomatology. Exposures to a range of negative life events and stressors were also assessed.
Gender and demographics
Participants were asked for both their sex assigned at birth (male/female) and gender identity (open text box). Asking about gender in this way allowed participants to describe their gender in their own words. The study was advertised as a study for TGD young people. Participants were asked for their year of birth and whether they were living in Australia at the time of the survey to determine their eligibility. Participants were also asked about their current living situation.
Current psychopathology
Depressive symptoms were indexed on the Patient Health Questionnaire (PHQ-A) (Kroenke et al., Reference Kroenke, Spitzer and Williams2001). The PHQ-A is a nine-item scale that is scored from 0–27 and can be categorised into no depressive disorder (0–4); possible mild depressive disorder (5–9); possible moderate depressive disorder (10–14); possible moderately severe depressive disorder (15–19); and possible severe depressive disorder (20–27) (Kroenke et al., Reference Kroenke, Spitzer and Williams2001). Anxiety was measured using the Generalised Anxiety Disorder seven-item Scale (GAD-7) (Spitzer et al., Reference Spitzer, Kroenke, Williams and Lowe2006). The categories for the GAD-7 are based on scores suggestive of a generalised anxiety disorder (⩾5); moderate to severe anxiety (⩾10); and severe anxiety (⩾15) (Spitzer et al., Reference Spitzer, Kroenke, Williams and Lowe2006).
Self-reported psychiatric diagnoses
Psychiatric diagnoses (depression, anxiety disorders, post-traumatic stress disorder, eating disorders, autism spectrum disorder, personality disorders, psychosis and substance use disorders) were listed and participants were asked whether a health professional had ever diagnosed the individual with the specific psychiatric conditions.
Self-reported adverse health outcomes
The five self-reported adverse health outcomes measured were: wanting to self-harm, self-harming, reckless behaviour that purposely puts one's life at risk, suicidal thoughts and suicide attempts. These were measured by asking participants whether they had engaged in the outcome within the last 12 months, prior to the last 12 months or never. Here we report a lifetime prevalence of these adverse health outcomes.
Exposure to negative experiences
Participants were asked about a range of negative experiences that are potentially associated with poor mental health. Participants were asked to select all the factors that they had experienced from the list provided. These items included: issues with accommodation (including homelessness), body dysphoria, bullying, discrimination, employment issues, experiencing a significant loss, feeling isolated from not knowing other TGD people, feeling isolated from services, helping others with their issues with mental health, a lack of family support, peer rejection and issues with school, university or technical college (henceforth education settings).
Statistical analysis
IBM SPSS Statistics, version 24, and Stata, version 15, were used to obtain descriptive statistics (frequencies, means, standard deviations), and to develop regression models. Logistic regression models were used to evaluate associations between potential drivers and adverse health outcomes, psychiatric diagnoses, and current psychopathology using known cut off-scores on the PHQ-A and the GAD-7. Linear regression models were used to evaluate potential drivers of poor mental health and current psychopathology measured by the GAD-7 and the PHQ-A. All reported regressions are adjusted for age and sex assigned at birth. All regression models were evaluated using diagnostic testing and no major deviations in distributional assumptions were detected.
Results
Demographics
The majority of participants were assigned female at birth (74.4%). Aboriginal and/or Torres Strait Islander people comprised 3.7% of this sample, a proportion that is representative of Australian population demographics (Australian Bureau of Statistics, 2014). The mean age of participants was 19.37 years (s.d. = 3.15). A total of 29.7% (n = 255) of participants self-identified as trans male or male, 15% (n = 129) identified as trans female or female, and 48.6% (n = 417) identified as various non-binary identities including non-binary transmasculine, non-binary femme, agender, bigender, pangender and other non-binary identities.
Most participants were living with parents (60.3%), 18.7% were in shared accommodation, 4.7% were living with other family members, 4.3% were living with a partner, 3.7% were living alone, 3.4% were in a residential college, 2.3% in supported accommodation and 1.4% had no fixed accommodation. One quarter of participants lived in Victoria (25.2%), 20.0% in New South Wales, 17.2% in Queensland, 15.9% in Western Australia, 12.0% in South Australia, 6.5% in the Australian Capital Territory, 2.7% in Tasmania and 0.5% in the Northern Territory. There was slight overrepresentation in the Australian Capital Territory, South Australia, Tasmania, Victoria and Western Australia while New South Wales, the Northern Territory, Queensland were underrepresented compared to 2015 population estimates by the Australian Bureau of Statistics (Australian Bureau of Statistics, 2016).
Self-harm and suicidality
Table 1 reports the lifetime prevalence rates of adverse health outcomes among our sample. Self-harm was commonly reported, with 91.3% ever wanting to self-harm and 79.7% self-harming at some point during their life. A majority of participants had engaged in reckless behaviour to risk their life (62.8%). Over three quarters (82.4%) of participants reported ever having suicidal thoughts and 48.1% had ever attempted suicide. There were no statistically significant differences in the prevalence of all lifetime adverse health outcomes between TGD young people under the age of 18 compared to those aged 18 or older. However, there were significant differences between TGD young people who were birth-assigned female compared to those birth-assigned male as tested with a Pearson χ2 test. Participants assigned female at birth reported higher rates of wanting to self-harm (F = 13.724, p < 0.001), self-harming (F = 31.633, p < 0.001), reckless behaviour to purposely put one's life at risk (F = 6.323, p = 0.012) and suicidal thoughts (F = 4.139, p = 0.042). There was no statistically significant difference between these groups for suicide attempts.
Table 1. Lifetime prevalence of self-harm, suicidal thoughts and suicide attempts among trans young people

* χ2 test significant difference between the two comparative groups (p < 0.05).
** χ2 test significant difference between the two comparative groups (p < 0.01).
Self-reported psychiatric diagnoses
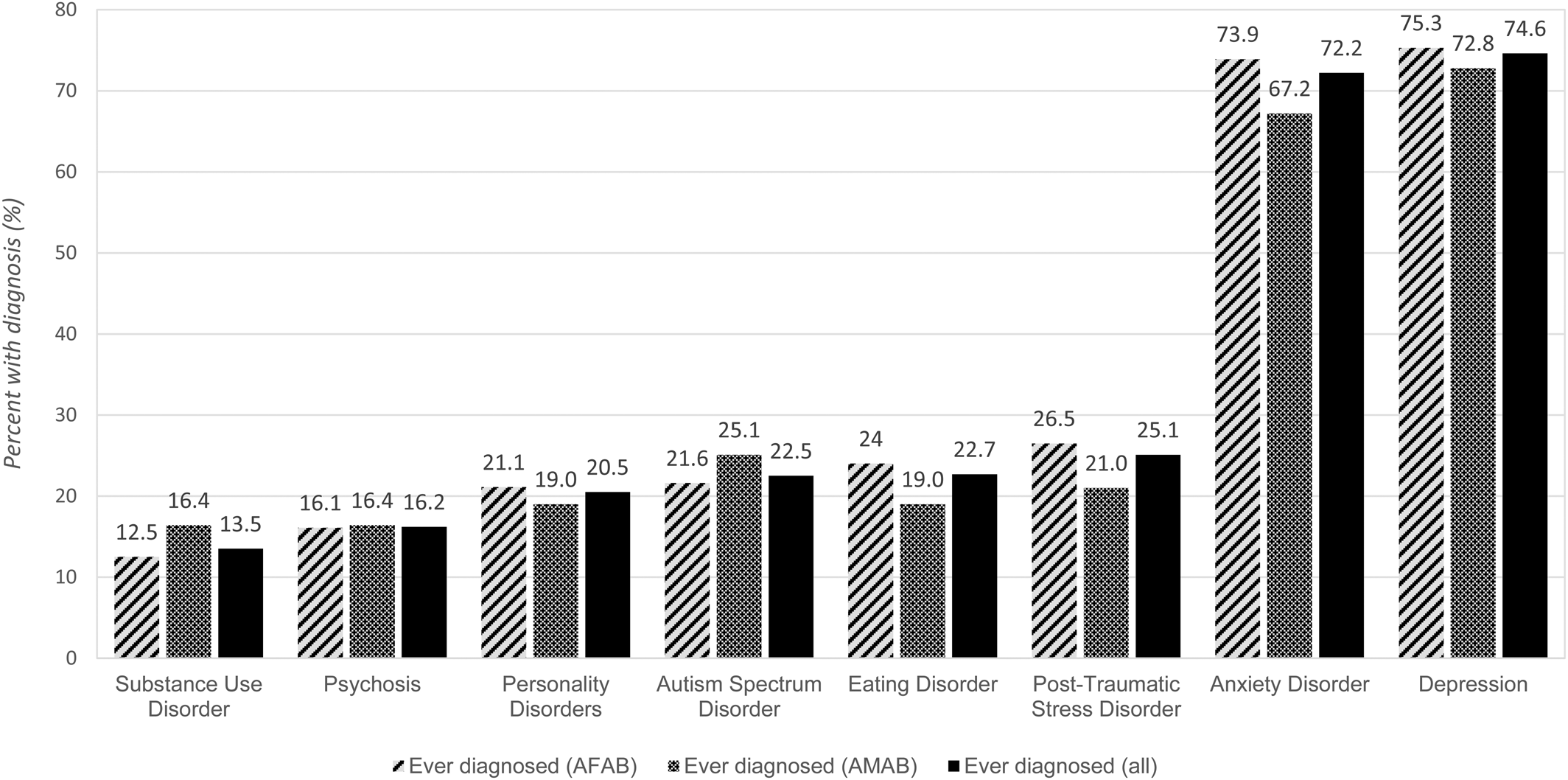
Figure 1 summarises the prevalence of self-reported psychiatric diagnoses ever received by a health professional. The most prevalent diagnoses were depression (74.6%) followed by anxiety (72.2%) and post-traumatic stress disorder (25.1%). There were no statistically significant differences in prevalence between participants assigned female at birth and those assigned male at birth across all diagnoses.
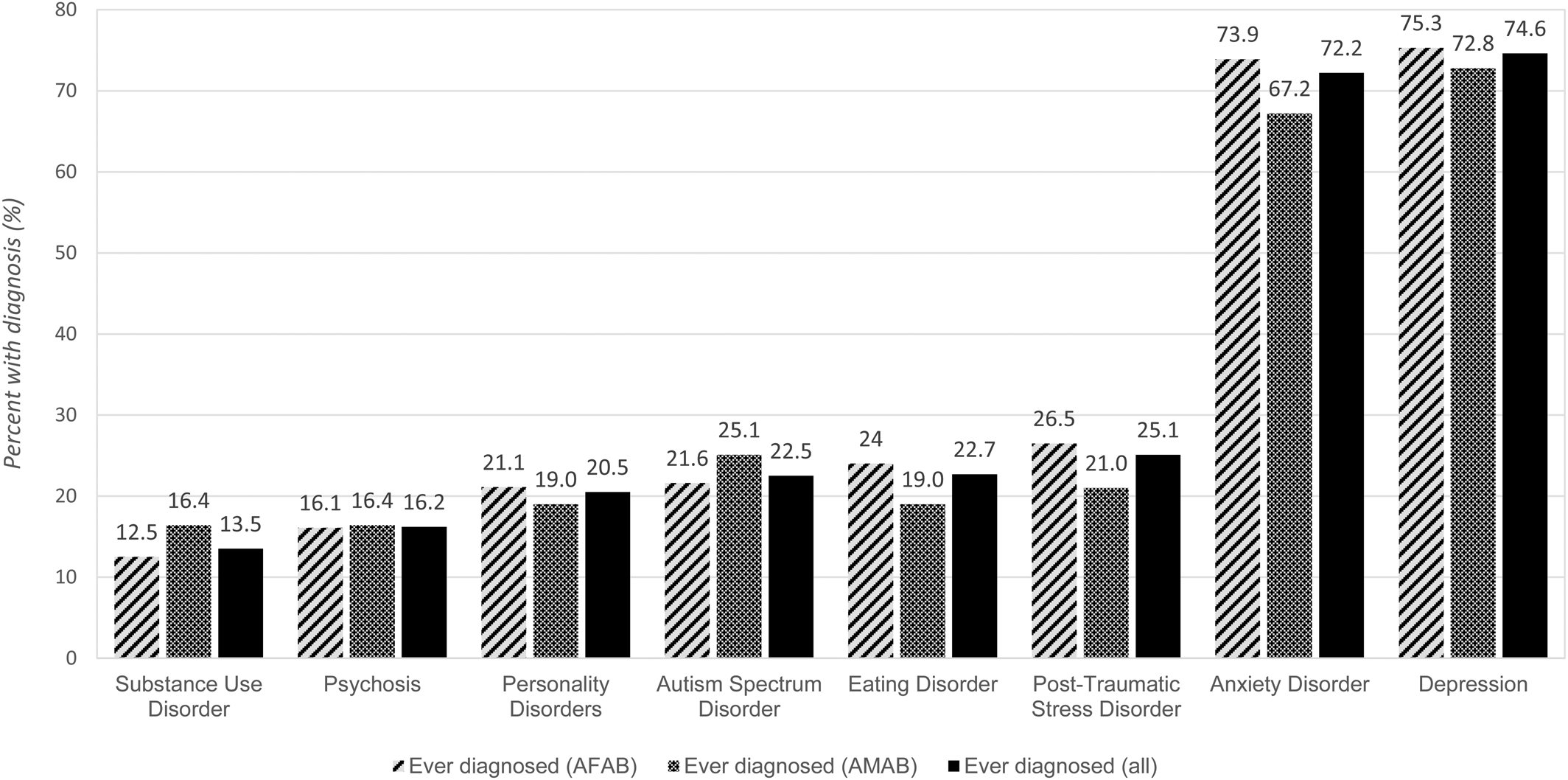
Fig. 1. Prevalence of self-reported psychiatric diagnoses among trans young people (n = 756).
Current psychopathology
More participants scored in the moderate to severe anxiety range with 11.8% of participants reporting minimal anxiety, 26.0% reporting mild anxiety, 30.5% reporting moderate anxiety and 31.6% reporting severe anxiety during the prior 2 weeks (n = 845). The mean GAD-7 score was 11.53 (s.d. = 5.65, n = 845). Based on the GAD-7 functional impairment scale, only 7.6% of the sample (n = 65) had no functional impairment, while 52.2% (n = 443) had some difficulties, 28.0% (n = 238) found it very difficult to carry out everyday tasks and 12.3% (n = 105) reported extreme difficulties. Depressive symptoms similarly increased in severity with 7.5% of participants reporting no depressive symptoms, 16.2% with mild depressive symptoms, 21.6% with moderate depressive symptoms, 24.6% with moderately severe depressive symptoms and 30.2% with severe depressive symptoms during the 2 weeks prior to completing the survey (n = 736). The mean PHQ-A score was 15.26 (s.d. = 7.04, n = 736).
Exposure to negative experiences
Young people in this population were commonly exposed to negative experiences, including peer rejection (89.0%), issues within educational settings (78.9%) and bullying (74.0%). Body dysphoria was commonly experienced (93.8%). These patterns of exposure are summarised in Tables 2–4.
Table 2. Potential predictors of self-harming and suicidal behaviours

Odds ratios adjusted for sex assigned at birth and age (by year of birth).
*p < 0.05; **p < 0.01.
Table 3. Psychiatric diagnoses and associations with negative experiences

Odds ratios adjusted for sex assigned at birth and age (by year of birth).
*p < 0.05; **p < 0.01.
Table 4. Self-reported current psychopathology and associations with negative experiences

Odds ratios adjusted for sex assigned at birth and age (by year of birth). Current severe anxiety defined as scoring a 15 or above on the GAD-7 and current moderately severe to severe depressive symptoms defined as scoring 15 or above on the PHQ-A.
*p < 0.05; **p < 0.01.
Associations between negative experiences and self-harm and suicidality
Table 2 reports the associations between potential drivers of poor mental health and the five adverse health outcomes of self-harm and suicide measured. The majority were associated with an adverse outcome. For example, participants with a history of self-harm had significantly elevated odds ratios for exposure to issues with accommodation (including homelessness) (OR 4.099, 95% CI 2.131–7.883) and within educational settings (OR 3.539, 95% CI 2.301–5.442). Participants with a prior suicide attempt had significantly elevated odds ratios for exposure to issues with accommodation (OR 5.716, 95% CI 3.617–9.031) and within educational settings (OR 3.892, 95% CI 2.528–5.992).
Associations between negative experiences and psychiatric diagnoses
Table 3 summarises the associations between potential drivers of poor mental health and psychiatric diagnoses. Participants who had been diagnosed with depression reported a greater than threefold increase in their likelihood of experiencing issues within educational settings (OR 3.604, 95% CI 2.424–5.359) and accommodation issues (OR 3.214, 95% CI 1.796–5.752). For participants who had been diagnosed with an anxiety disorder, odds ratios of 3.2 (95% CI 2.149–4.654) were estimated for educational settings and 2.7 for accommodation issues (95% CI 1.586–4.439). Participants who had ever been diagnosed with PTSD were more than three times as likely to have experienced accommodation issues (OR 3.285, 95% CI 2.173–4.965) and twice as likely to have experienced discrimination (OR 2.003, 95% CI 1.318–3.045).
Associations between negative experiences and current psychopathology
Both issues with accommodation and issues within educational settings had the largest effect on all associations between life experiences and current psychopathology. Participants with severe current anxiety (scoring 15 or higher on the GAD-7) had more than a twofold increase of odds of exposure to accommodation issues (OR 2.379, 95% CI 1.567–3.613) and issues within educational settings (OR 2.639, 95% CI 1.633–4.266). The results were similar for participants with more severe current depressive symptoms (scoring 15 or higher on the PHQ-A) for exposure to accommodation issues (OR 3.374, 95% CI 2.206–5.160) and issues within educational settings (OR 3.265, 95% CI 2.197–4.851). These results are reflected in the linear regression modelling of the GAD-7 and PHQ-A instruments, as seen in Table 4.
Discussion
In the current study, we present the findings from a large sample of TGD young people and the indicators of their mental health. Results demonstrated high rates of current depressive and anxiety symptoms, and of self-reported psychiatric diagnoses. Rates of self-harm and suicidality were exceptionally high, with almost four in every five participants having a history of self-harm and nearly one in two having attempted suicide. Negative experiences, including experiencing unstable accommodation, discrimination, bullying, feeling unsupported from family, and issues in education and employment, were associated with most poor mental health outcomes in this sample. The largest associations between life experiences and self-harming and suicide attempts related to issues with housing and education. These are two areas that can be improved through interventions with families and educational environments to make them more supportive of TGD young people.
Self-harm and suicidality
The lifetime percentages of reported self-harm and suicide attempts were 79.7% and 48.1%, respectively. This suicide attempt rate is over 14 times greater than the general Australian adult population rate (Australian Bureau of Statistics, 2007). These rates are strikingly similar to those recently reported in the UK, where 84% of trans adolescents report self-harming and 45% report attempted suicide (Bradlow et al., Reference Bradlow, Bartram, Guasp and Jadva2017). The lack of statistical difference between the rates of self-harm and suicidality between the under-18 and over-18 participants implies that self-harming and suicidal behaviours may tend to begin early and continue into young adulthood. Rates of suicidal ideation and suicide attempts are higher than rates seen internationally for trans adults, where a meta-synthesis averaged reported rates of suicidal ideation and attempts to be 55% and 29%, respectively (Adams et al., Reference Adams, Hitomi and Moody2017).
Mental health
Over three-quarters of participants reported exhibiting moderate to severe depressive symptoms during the previous 2 weeks (76.4%) and more than half of the participants reported moderate to severe anxiety during the previous 2 weeks (62.1%). These are consistent with the self-reported rates of diagnosed depression and anxiety. Current findings of depressive and anxiety symptomatology are higher than would be expected in the general population. Specifically, in comparison with the general Australian adolescent population, the rates of depressive symptoms are seven times higher and anxiety-related symptoms are over four times higher (Lawrence et al., Reference Lawrence, Johnson, Hafekost, Boterhoven De Haan, Sawyer, Ainley and Zubrick2015). Our results similar to other literature that shows rates of depression, anxiety and emotional distress in trans young people to be higher than both the general population and same-gender attracted youth (Hillier et al., Reference Hillier, Jones, Monagle, Overton, Gahan, Blackman and Mitchell2010; Hyde et al., Reference Hyde, Doherty, Tilley, McCaul, Rooney and Jancey2014).
Co-occurring psychiatric disorders in gender diverse populations are unlikely to be simply related to the person's gender identity, and may instead reflect the response of the individual's familial and social environment to that identity and its expression (Vrouenraets et al., Reference Vrouenraets, Fredriks, Hannema, Cohen-Kettenis and de Vries2015). It has been suggested that cisgender populations under the same incessant exposure to psychological stressors would in all likelihood experience comparable of rates of depression and anxiety as trans populations (Inch, Reference Inch2016). Higher rates of anxiety among transgender adult populations have also been reported, and have been attributed to low self-esteem and poor interpersonal functioning (Bouman et al., Reference Bouman, Claes, Brewin, Crawford, Millet, Fernandez-Aranda and Arcelus2017).
Exposure to negative experiences as potential drivers of poor mental health
Mental distress experienced by gender diverse populations does not intrinsically arise from the experience of an incongruent gender identity, but is more likely due to exposures to negative external events. Many of our participants were exposed to negative experiences known to be associated with poor mental health from other research (Mustanski and Liu, Reference Mustanski and Liu2013; Roberts et al., Reference Roberts, Rosario, Slopen, Calzo and Bryn Austin2013; Taliaferro et al., Reference Taliaferro, McMorris, Rider and Eisenberg2018), such as discrimination (68.9%), issues with accommodation (22.0%) and feeling isolated from other TGD people and services (66.1% and 60.1%, respectively). Notably, every potential driver of poor mental health was associated with participants reporting depressive symptoms at the more severe end of the spectrum. These risk factors are external (with the exception of body dysphoria) and are therefore potentially preventable. Previous research has indicated that prepubescent trans young people who are able to socially transition exhibit psychopathology similar to the general population. This suggests that if gender diverse children are supported to explore and affirm their gender identity they are more mentally healthy (Olson et al., Reference Olson, Durwood, Demeules and McLaughlin2016).
Accommodation issues and family support
The high rates of precarious accommodation in this population imply there is a need for better family support for TGD young people. We inferred that, because of the age range of our participants, family support will often form a vital component of stable accommodation. A high proportion of participants (65.8%) reported that they lacked family support, and this was associated with poor mental health outcomes. Research has shown that trans young people who are supported in their identity by their parents have fewer difficulties with mental health, are less likely to report suicidal ideation and are much more likely to have a secure/stable home to live in (Travers et al., Reference Travers, Bauer, Pyne, Bradley, Gale and Papadimitriou2012).
Educational environments (school, university and technical college)
Most participants in this study reported negative experiences within education environments, and these were significantly associated with all adverse health outcomes measured. This is in line with previous research that has established that LGBTIQ young people are not adequately supported in school settings, and that this lack of support is associated with negative health outcomes (Jones, Reference Jones2015; Bradlow et al., Reference Bradlow, Bartram, Guasp and Jadva2017). TGD young people in schools who are not supported by teachers are more likely to experience abuse at school and are more likely to have worse educational outcomes than gender diverse young people who do feel supported by their teachers; e.g. through the use of correct language (Jones et al., Reference Jones, Smith, Ward, Dixon, Hillier and Mitchell2016). Programs that proactively and equitably support TGD young people in educational settings are necessary to mitigate these transphobic experiences.
Bullying and discrimination
The high rates of bullying (74%) and discrimination (68.9%) reported by participants underscore the need for broader interventions that target public perceptions through promoting acceptance and understanding of gender diversity. Gender diverse young people in Australia are more likely to be exposed to homophobic and/or transphobic abuse, including physical abuse, than their same-gender attracted (LGB) peers (Jones and Hillier, Reference Jones and Hillier2013). These findings highlight the need for anti-discrimination and anti-bullying programs that are specific to gender diverse young people.
Implications
These results show that TGD young people are a marginalised group that urgently needs interventions specifically targeted to improve their mental health. The findings show the need for improved protections for TGD young people to reduce many of the factors that are associated with poor mental health, including policies to decrease discrimination, bullying, abuse and other negative experiences that TGD young people are exposed to. These policies should be considered for implementation in educational, clinical and support settings. There is also a need to improve general understanding and acceptance in the general public. Given these high rates of mental health difficulties, it is also vital that TGD young people are able to access effective, safe and TGD-friendly mental health care providers.
Study limitations
The study design was cross-sectional, and therefore causal pathways cannot be inferred. Longitudinal data are necessary to more fully investigate the temporal relationships between adverse life events and mental health outcomes. In addition, we surveyed only Australian TGD young people, and results may not be generalisable to other countries, although our findings are remarkably consistent with international literature. There is potential for self-selection bias due to the survey's online nature. In addition, people without internet access were automatically excluded from the survey. The majority of participants were assigned female at birth, and therefore these data may not be representative of the wider TGD population. Further research specific to Aboriginal and Torres Strait Islander TGD young person populations should be developed in collaboration with Aboriginal and Torres Strait Islander communities.
Conclusion
These findings support previous international research indicating that TGD populations experience mental health issues at higher rates than cisgender populations. It is significant that these rates of mental health issues are being reported in a community-based sample of young people, rather than a clinical sample. This study also demonstrates that TGD young people report alarmingly high rates of negative experiences, including discrimination and bullying. These negative and transphobic experiences are associated with poor mental health of TGD young people. Young people need to be supported by their peers, families, school and work peers to achieve optimal levels of mental wellbeing. Furthermore, services – including schools – need to ensure that they are gender inclusive to respond effectively and appropriately to the mental health needs of TGD young people outlined in this paper. These measures should be taken proactively as preventative measures, rather than as reactive measures, to create equitable spaces for all young people where they can thrive. This would help to prevent poor mental health in this population. As more TGD young people seek support from medical and mental health services in Australia and worldwide, it is crucial that clinical service providers are aware of the mental health issues faced by gender diverse young people and that they can offer TGD competent health care.
Author ORCIDs
Penelope Strauss, 0000-0002-4828-0983.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors. PS is supported by an Australian Government Research Training Program Scholarship at the University of Western Australia. AL is supported by an NHMRC Career Development Fellowship (#1148793).
Conflict of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.