


Introduction
An influential view on the psychopathology of schizophrenia proposes that auditory hallucinations and other positive symptoms are produced by the external misattribution of internally generated events (Frith, Reference Frith1992). The ability to correctly remember the origin of events has been termed source monitoring (Johnson et al. Reference Johnson, Hashtroudi and Lindsay1993). Deficits in source monitoring have been demonstrated in schizophrenia, and patients tend to attribute self-produced items to an external source (Keefe et al. Reference Keefe, Arnold, Bayen and Harvey1999). Additionally, there seems to be a particular association with auditory hallucinations and delusions (Bentall et al. Reference Bentall, Baker and Havers1991; Brébion et al. Reference Brébion, Gorman, Amador, Malaspina and Sharif2002, Reference Brébion, Gorman, Malaspina and Amador2005; Brunelin et al. Reference Brunelin, Poulet, Bediou, Kallel, Dalery, d'Amato and Saoud2006).
However, it is clear that not all internal events are perceived as auditory hallucinations or delusions. It has been postulated that the perception only becomes abnormal for intrusive thoughts that are aversive to the individual, and the external attribution is a mechanism to reduce anxiety (Bentall, Reference Bentall1990a, Reference Bentall and Bentallb; Morrison et al. Reference Morrison, Haddock and Tarrier1995). In support, a classic observation is that auditory hallucinations in schizophrenia have a derogatory content (Fish, Reference Fish1967), although they may also be affirmative or benevolent (Miller et al. Reference Miller, O'Connor and DiPasquale1993; Chadwick et al. Reference Chadwick, Lees and Birchwood2000). In addition, when subjects speak aloud but hear a distorted version of their own voice, actively psychotic individuals with schizophrenia, but not healthy subjects, show the greatest external misattributions with negative adjectives (Johns et al. Reference Johns, Rossell, Frith, Ahmad, Hemsley, Kuipers and McGuire2001). In the experiment of Johns et al. (Reference Johns, Rossell, Frith, Ahmad, Hemsley, Kuipers and McGuire2001), however, subjects had read aloud adjectives that were visually presented, whereas source monitoring tasks typically require subjects to generate an individual response to a given probe. The effect of negatively valenced stimuli on source monitoring in schizophrenia has not been examined.
In the present study, we sought to determine whether the external misattribution bias was modulated by the affective content of the material. We expected that negative stimuli would exacerbate the bias of individuals with schizophrenia with auditory hallucinations and delusions to attribute self-produced words to an external source.
Method
Thirty male individuals meeting DSM-IV criteria for schizophrenia (APA, 1994) on stable antipsychotic doses were recruited from the South London and Maudsley NHS Trust. From the Scale for the Assessment of Positive Symptoms (SAPS; Andreasen, Reference Andreasen1984a), 20 patients were classified as experiencing active hallucinations or delusions (having a minimum rating of 3 on each subscale of hallucinations or delusions, which reflected the experience of symptoms at least daily with a significant impact on behaviour; referred to here as ‘psychotic’ patients) and 10 patients were not suffering from either of these symptoms at the time of the testing (with a rating of  2 on each subscale; referred to as ‘remitted’ patients) but having a history of psychotic symptoms. For an exploratory subgroup analysis of interactions, psychotic patients were subdivided into 14 patients with auditory hallucinations (minimum hallucinations score of 3, irrespective of rating on the delusions scale) and six with delusions (minimum rating of 3 on the delusion subscale and a maximum of 2 on any hallucinations subscale). Symptoms were also assessed with the Scale for Negative Symptoms (SANS; Andreasen, Reference Andreasen1984b) and the Calgary Depression Scale for Schizophrenia (CDSS; Addington et al. Reference Addington, Addington and Schissel1990). IQ was estimated using the National Adult Reading Test (NART; Nelson, Reference Nelson1991). The clinical assessment and source monitoring task were performed on the same day.
2 on each subscale; referred to as ‘remitted’ patients) but having a history of psychotic symptoms. For an exploratory subgroup analysis of interactions, psychotic patients were subdivided into 14 patients with auditory hallucinations (minimum hallucinations score of 3, irrespective of rating on the delusions scale) and six with delusions (minimum rating of 3 on the delusion subscale and a maximum of 2 on any hallucinations subscale). Symptoms were also assessed with the Scale for Negative Symptoms (SANS; Andreasen, Reference Andreasen1984b) and the Calgary Depression Scale for Schizophrenia (CDSS; Addington et al. Reference Addington, Addington and Schissel1990). IQ was estimated using the National Adult Reading Test (NART; Nelson, Reference Nelson1991). The clinical assessment and source monitoring task were performed on the same day.
In the source monitoring task, the subject and experimenter alternately produced words from neutral (e.g. kitchen utensils) and negative (e.g. swear words) categories, presented in a counterbalanced order for alternate subjects. There were six categories for each valence (neutral, negative), and each source (patient, experimenter) generated two words for each category, for a total of 48 words. To demonstrate the task, there was a practice with the category ‘fruits’, in which the subject and experimenter alternately generated two words each. The patient was not informed that he would be required to recall the source of the words. Following the word generation, the experimenter rated the subject in the psychopathology scales above. The experimenter then presented the same words randomly, maintaining a neutral prosody for all words (Shea et al. Reference Shea, Sergejew, Burnham, Jones, Rossell, Copolov and Egan2007), and the subject decided on the source.
The data were analysed as a repeated measures ANOVA with a between-subject factor (symptoms group) and two within-subject factors (source and emotional valence). The outcome variable was the proportion of errors for each combination of the within-group factors, following arcsine transformation to improve normality (Howell, Reference Howell1992). Statistical analysis was performed using the R statistical package (R Development Core Team, 2005). Univariate summary statistics presented in the results section are given as mean±standard error of the mean (s.e.m.). Because of the small sample size, we also confirmed the results for the main hypothesis, concerning the statistical significance of the interaction source by symptom group by emotional valence, with a non-parametric randomization test that does not rely on asymptotic arguments, balanced groups or assumptions of normality and variance homogeneity (Good, Reference Good2000). Group demographic features are reported as the mean and s.e.m. and were analysed with t tests.
Results
There were no significant differences between symptomatic patients and remitted patients in mean age (psychotic 33.7±2.3 years, remitted 35.5±2.9; t=0.46, df=28, p=0.65), SAPS ratings, apart from hallucinations and delusions (psychotic 1.2±0.3, remitted 0.6±0.3; t=1.24, df=28, p=0.22), depressive symptoms as measured by the CDSS (psychotic 5.0±0.9, remitted 2.8±1.7; t=1.28, df=28, p=0.21), or duration of illness (psychotic 9.7±2.3 years, remitted 11.5±3.8). Negative symptoms were significantly higher in psychotic (SANS ratings: 2.8±0.3) than in remitted patients (1.3±0.4) (t=2.60, df=28, p<0.05), and IQ was significantly lower in psychotic (108±1.7) than in remitted patients (115±2.0) (t=2.29, df=27, p<0.05).
Consistent with the literature, external misattributions were significantly more frequent than self-misattributions [main effect of source: F(1, 28)=33.0, p<0.01]. Patients erroneously attributed the source to the interviewer in 24% of the responses they generated themselves, whereas they misattributed the origin to themselves in 11% of those produced by the interviewer. The bias towards external misattributions varied by symptom group, being greater for psychotic than remitted patients [source by symptom group interaction: F(1, 28)=5.6, p<0.05]. Psychotic patients externally misattributed 29% of their self-generated words but wrongly attributed to themselves only 11% of the interviewer responses. In remitted patients, this difference was smaller: 15% for external misattributions and 10% for self-misattributions.
Psychotic patients but not remitted patients were more likely to generate external misattributions for negative as compared to neutral probes [source by symptom group by emotional valence interaction: F(1, 28)=5.1, p<0.05], which was also confirmed by the permutation test (p<0.05). Symptomatic patients externally misattributed 35% of the responses with a negative connotation, but only 22% of the neutral responses. By contrast, remitted patients wrongly attributed the source to the interviewer in 15% and 14% of neutral and emotional stimuli respectively (Fig. 1). The effect of emotional valence was similar for hallucinator and non-hallucinator psychotic patients. External misattributions were made for 21% of neutral and 35% of negative probes in hallucinators, and 25% of neutral and 36% of negative stimuli in non-hallucinators.
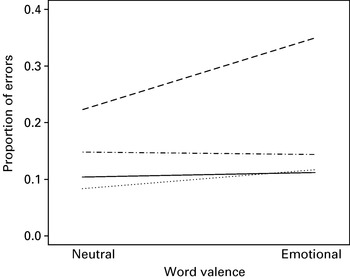
Fig. 1. Percentage of misattribution errors by patient group (psychotic versus remitted), source of the word (self versus other) and emotional valence (neutral versus emotional word). Psychotic patients produced more external misattribution than remitted patients, and this effect was significantly higher for negative than for neutral words. – – –, Psychotic, other; —, psychotic, self; · – · – ·, remission, other;........, remission, self.
Covarying by IQ and negative symptoms did not alter the results. In particular, the interaction between symptoms group (psychotic versus remitted), source and emotional valence remained significant [F(1, 22)=5.7, p<0.05], indicating that the modulation effect of affective valence on external misattributions for psychotic patients was not confounded by IQ and SANS score.
Discussion
Consistent with previous literature, we found that individuals with schizophrenia showed greater external misattributions than self-misattributions, which was particularly evident in patients with hallucinations and delusions who made more external misattributions than patients in remission. Moreover, source monitoring errors were modulated by a negative affective valence in actively psychotic patients as they showed a significant increase in external misattribution errors for negative stimuli relative to neutral probes. The affective modulation was not evident in patients without hallucinations or delusions.
The present work adds to the growing body of research linking external misattributions with positive symptoms in schizophrenia (Bentall et al. Reference Bentall, Baker and Havers1991; Brébion et al. Reference Brébion, Gorman, Amador, Malaspina and Sharif2002, Reference Brébion, Gorman, Malaspina and Amador2005; Brunelin et al. Reference Brunelin, Poulet, Bediou, Kallel, Dalery, d'Amato and Saoud2006). In addition, we observed an affective modulation of the misattribution errors in these patients. Negative probes were associated with more external misattributions in patients with hallucinations and delusions. Morrison et al. (Reference Morrison, Haddock and Tarrier1995) suggested that it is intrusive thoughts regarded as incompatible or aversive to the individual that are attributed to an external source. In addition, the resultant reduction in anxiety helps to maintain the external misattributions (Bentall, Reference Bentall1990a, Reference Bentall and Bentallb). The affective probes in the present study were designed to elicit more negative responses, which may have been particularly salient to patients with hallucinations and delusions who developed a heightened state of aversive arousal that was ameliorated by external misattributions. However, this is a tentative interpretation that requires further evidence from measures of the change in anxiety before and after the external misattributions.
Malevolent and distressful auditory hallucinations are more commonly reported, but comforting or supportive hallucinations have also been described (Miller et al. Reference Miller, O'Connor and DiPasquale1993; Chadwick et al. Reference Chadwick, Lees and Birchwood2000). Although the content of a hallucination may be negative or positive, the experience may nonetheless be perceived as intrusive. If both negatively and positively valenced stimuli elicit high arousal (Costafreda et al. Reference Costafreda, Brammer, David and Fu2007) and perhaps anxiety, they may thus be attributed to an external source (Bentall, Reference Bentall1990a, Reference Bentall and Bentallb).
We found no evidence of a differential bias for patients with auditory hallucinations relative to those with predominantly delusions, suggesting that the affective modulation is related to both hallucinations and delusions. The small numbers in our study, however, have limited power to detect possible differences, and the data will require replication in larger samples. In addition, all the subjects were male, which limits the generalizability of the findings. Our results are unlikely to be explained by differences in the other patient group variables as covarying for IQ and negative symptoms did not alter the findings and there were no significant differences in level of depressive symptoms, which has been associated with greater self-misattributions (Morrison & Haddock, Reference Morrison and Haddock1997). In addition, although formal measures of memory function were not acquired, any difference in memory function would not necessarily account for the negative affective modulation of the externalizing cognitive bias in source monitoring.
In summary, greater external misattributions were produced by individuals with schizophrenia, in particular those with hallucinations and delusions. External misattributions were increased by negative affective stimuli in actively psychotic patients. Thus, there was affective modulation by negatively valenced stimuli of the externalizing cognitive bias evident in patients with hallucinations and delusions.
Acknowledgements
This work was supported by a Wellcome Trust Travelling Fellowship to C.H.Y.F.
Declaration of Interest
None.

