



Introduction
Individuals with schizophrenia or schizophrenia spectrum disorders (SSD)Footnote 1Footnote †, and those experiencing their first episode of psychosis, are characterised by robust cognitive impairments spanning general intelligence (IQ), memory, processing speed, and executive functions (Sheffield, Karcher, & Barch, Reference Sheffield, Karcher and Barch2018). Similar, though less severe, cognitive impairments, alongside changes in social, emotional, and behavioural functioning, are also present before the onset of the first symptoms of the disorder (Laurens & Cullen, Reference Laurens and Cullen2016; Sheffield et al., Reference Sheffield, Karcher and Barch2018). Using routinely collected data on academic achievement (such as performance in national exams) to identify the cognitive precursors of schizophrenia in the population may provide a feasible alternative to the administration of extensive cognitive batteries (Frey, Reference Frey2019).
Two prior systematic reviews of antecedents of schizophrenia in population and birth cohort studies, now over a decade old, provided inconsistent evidence for poorer academic achievement among individuals who later developed schizophrenia relative to those who did not (MacCabe, Reference MacCabe2008; Welham, Isohanni, Jones, & McGrath, Reference Welham, Isohanni, Jones and McGrath2009). More recently, our meta-analyses of data from prospective longitudinal studies of population cohorts, prospective studies of individuals with a family history of schizophrenia, and ‘follow-back’ studies of adults with schizophrenia reported that low IQ, but not poor general academic or mathematics achievement, precedes illness onset (Dickson, Laurens, Cullen, & Hodgins, Reference Dickson, Laurens, Cullen and Hodgins2012). Inconsistency in findings across these three previous reviews might reflect differences in educational systems, the few studies available to inform the reviews, or that academic achievement is an indirect and less sensitive measure of cognitive function than standardised neurocognitive tests. Since the publication of our meta-analyses, there have been additional investigations demonstrating that poor academic achievement in childhood and adolescence is associated with the later development of schizophrenia (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; Sørensen et al., Reference Sørensen, Debost, Agerbo, Benros, McGrath, Mortensen and Petersen2018). The first aim of the present study was thus to update our earlier meta-analyses comparing general academic and mathematics achievement in youth who later developed schizophrenia and those who did not. As in our earlier work, we included only studies of children aged 16 years or younger to minimise the likelihood of identifying a prodromal-related decline in academic achievement.
Alongside measures of academic achievement, other school-related risks and protective factors for schizophrenia have been reported. High educational attainment has been observed to be associated with protection against cognitive decline (Stern, Reference Stern2002) and improved cognitive performance (Holthausen et al., Reference Holthausen, Wiersma, Sitskoorn, Hijman, Dingemans, Schene and van den Bosch2002) among individuals with the disorder. Conversely, recent evidence shows that lower educational attainment is associated with subsequent schizophrenia, and, to a lesser extent, bipolar disorder, but not with adulthood depression (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; Tempelaar, Termorshuizen, MacCabe, Boks, & Kahn, Reference Tempelaar, Termorshuizen, MacCabe, Boks and Kahn2017; Vreeker et al., Reference Vreeker, Boks, Abramovic, Verkooijen, van Bergen, Hillegers and Investigators2016). Thus, the second aim of the study was to undertake a meta-analysis to examine the level of education attained in individuals with and without schizophrenia. As compulsory secondary schooling extends to age 18 years in some countries, for this analysis only, we did not restrict included studies to those of children aged ⩽16 years but required that studies used samples of individuals with adult-onset schizophrenia (i.e. ⩾18 years of age).
Research indicates that impaired cognitive function during childhood may index vulnerability to schizophrenia (Matheson, Shepherd, Laurens, & Carr, Reference Matheson, Shepherd, Laurens and Carr2011). If poor academic achievement does precede illness onset and represents a readily identifiable risk marker for schizophrenia, we would expect to see evidence of poor academic achievement among at-risk youth. Indeed, a recent systematic review and meta-analysis found lower self-reported education level among help-seeking youth at ultra high-risk (UHR) for psychosis compared to healthy controls (Fusar-Poli et al., Reference Fusar-Poli, Tantardini, De Simone, Ramella-Cravaro, Oliver, Kingdon and McGuire2017). However, strategies identifying individuals based on UHR criteria identify only help-seeking adolescents or young adults who may be at imminent risk of developing psychosis and cannot provide information about whether low academic achievement is an antecedent of the disorder or an early prodromal disease process. It is currently not known whether poor academic achievement characterises children and adolescents identified as at-risk because they present with psychotic-like experiences (PLEs, an established risk marker for psychosis; Healy et al., Reference Healy, Brannigan, Dooley, Coughlan, Clarke, Kelleher and Cannon2019) or by virtue of having a family history of the disorder (Agnew-Blais & Seidman, Reference Agnew-Blais and Seidman2013). The third aim of the study was thus to conduct additional meta-analyses to examine general academic achievement aged 16 years or younger in youth at-risk for schizophrenia compared to typically developing peers.
Methods
A series of meta-analyses were conducted assessing: (1a) general academic and (1b) mathematics achievement in youth aged 16 years and younger who later developed schizophrenia compared to those who did not; (2) level of educational attainment among adults with and without schizophrenia; and, (3a) general academic achievement in at-risk youth aged 16 years or younger who presented with PLEs or (3b) had a first-degree relative with schizophrenia, relative to youth without PLEs or family history, respectively.
Selection procedure
A systematic review protocol was registered with PROSPERO: CRD42017067438. The literature search followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Moher, Liberati, Tetzlaff, & Altman, Reference Moher, Liberati, Tetzlaff and Altman2009). Two authors (EH and SYM) independently searched MEDLINE, PsycINFO, and Embase to identify articles published up to December 2019. Articles were screened for eligibility in three stages. First, records were reviewed by title and abstract for possible inclusion. Next, the full-text of relevant studies was examined. Third, a manual search of reference lists from eligible articles was conducted to locate additional studies not identified in the database searches.
Search strategy and eligibility
Schizophrenia and schizophrenia spectrum disorders
General academic and mathematics achievement. The literature search, adopted from the original review (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012), identified articles published between January 2011 and December 2019 using the following search terms: ‘schizophrenia’ AND (‘IQ’ OR ‘intelligence’ OR ‘motor’ OR ‘school’ OR ‘scholastic’ OR ‘academic’) AND (‘premorbid’ OR ‘prospective’ OR ‘cohort’ OR ‘high risk’). Inclusion criteria were: (1) written in English; (2) published or unpublished prospective birth cohort or genetic high-risk (i.e. family history) studies, or retrospective population sample studies; (3) an objective measure of cognitive functioning of youth aged 16 or younger; (4) results provided for participants who did and who did not develop schizophrenia in adulthood; and (5) sufficient data to determine effect sizes.
Educational level attained. An electronic database search was carried out, without date limitations, using the search terms ‘schizophrenia’ AND ('school’ OR ‘scholastic’ OR ‘education’ OR ‘academic’) AND (‘achievement’ OR ‘level’ OR ‘stage’ OR ‘years’). The inclusion criteria were: (1) written in English; (2) a sample of individuals with adult-onset diagnosis (aged 18 years or older) of schizophrenia and healthy control or general population comparison individuals; (3) summary data reported for educational level of both groups; and (4) sufficient data to calculate effect sizes.
Youth at-risk for schizophrenia and schizophrenia spectrum disorders
Two further literature searches were undertaken to identify published studies examining academic achievement in at-risk youth. Searches identified relevant articles using the key terms (‘psychotic-like experiences’ OR ‘psychotic-like symptoms’ OR ‘subclinical psychotic symptoms’ OR ‘auditory hallucinations’) or [‘schizophrenia’ AND (‘family history’ OR ‘genetic risk’ OR ‘offspring’ OR ‘first-degree relatives’] AND ('school’ OR ‘scholastic’ OR ‘academic’ OR ‘education’).
Inclusion criteria for both searches were: (1) published studies written in English; (2) objective measure of general academic achievement consisting of scores on at least two core academic subjects (e.g. literacy and mathematics) at age 16 years or younger. If the age range exceeded 16 years, studies were only included if at least two-thirds of participants were aged 16 years or younger (mean age + 1s.d. ⩽16 years); (3) scores recorded for youth reporting PLEs or having at least one first-degree relative with the disorder; (4) scores reported for a comparison group not at-risk for schizophrenia (i.e. not reporting PLEs in childhood or family history of the disorder, respectively); and (5) sufficient data to calculate effect sizes. No date limitations were applied.
Data extraction and risk of bias
Data were extracted from eligible studies using a structured coding form. Where additional data were needed, corresponding authors were contacted via email (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; Ramsay et al., Reference Ramsay, Barnett, Murray, Miettunen, Mäki, Järvelin and Veijola2018; Ranning et al., Reference Ranning, Laursen, Agerbo, Thorup, Hjorthøj, Jepsen and Nordentoft2017; Stramecki et al., Reference Stramecki, Kotowicz, Piotrowski, Frydecka, Rymaszewska, Beszłej and Misiak2018; Vreeker et al., Reference Vreeker, Boks, Abramovic, Verkooijen, van Bergen, Hillegers and Investigators2016). In the case of studies with overlapping samples, those with the greatest sample size were retained (Diaz, Velásquez, Susce, & de Leon, Reference Diaz, Velásquez, Susce and de Leon2008; Gurpegui et al., Reference Gurpegui, Martínez-Ortega, Aguilar, Diaz, Quintana and de Leon2005; Meesters et al., Reference Meesters, Schouws, Stek, de Haan, Smit, Eikelenboom and Comijs2013), except where there was insufficient data to undertake meta-analysis (Kendler, Ohlsson, Mezuk, Sundquist, & Sundquist, Reference Kendler, Ohlsson, Mezuk, Sundquist and Sundquist2016) and an alternative study was retained (MacCabe et al., Reference MacCabe, Lambe, Cnattingius, Torrång, Björk, Sham and Hultman2008). Study quality was rated by two authors using the Newcastle-Ottawa Scale for cohort and case-control studies (NOS; Wells et al., Reference Wells, Shea, O'Connell, Petersen, Welch, Losos and Tugwell2011). Using a star rating scale, the tool assesses three categories of study quality: selection, comparability, and exposure/outcome. Total possible scores range from zero to nine stars. There is no threshold for determining ‘good’ and ‘poor’ quality studies but accumulating stars index increasing study quality.
Statistical analyses
Meta-analyses were conducted in Stata 15 statistical package (StataCorp., 2017) using the METAN command which implements (Bradburn, Deeks, & Altman, Reference Bradburn, Deeks and Altman1999) a random-effects model (DerSimonian & Laird, Reference DerSimonian and Laird1986). This model accounted for variation in the true effect, assuming that the observed effects within each study constituted a random sample from a larger population. For all meta-analyses examining general academic or mathematics achievement, effect sizes were calculated as the standardised mean difference (SMD, Cohen's d) and interpreted as ‘small (0.2)’, ‘medium (0.5)’ and ‘large (0.8)’ (Cohen, Reference Cohen1992). The summary effect size for the educational level meta-analysis was an odds ratio (OR), and interpreted as ‘small (1.5)’, ‘moderate (2.5)’, ‘large (4.0)’ and ‘very large (10)’ (Rosenthal, Reference Rosenthal1996). An OR value of 1.0, or 95% confidence interval (CI) crossing 1.0, indicated no difference between the groups. To determine the magnitude of final pooled effect sizes for OR<1.0, OR was converted to 1.0/OR (Chen, Cohen, & Chen, Reference Chen, Cohen and Chen2010). For each pooled effect size, at a 95% significance level, a z-value and p-value were computed to provide an indication of the two-sided statistical significance of the association. For meta-analyses comprising six or more studies (Sutton, Duval, Tweedie, Abrams, & Jones, Reference Sutton, Duval, Tweedie, Abrams and Jones2000), small sample bias was assessed statistically utilising the Egger's Test.
Heterogeneity between studies was estimated using Cochran's Q (X 2 and p-value), and the degree of heterogeneity was measured by the I 2 statistic. I 2 values of 0–40% may be considered unimportant, 30–60% as moderate, 50–90% substantial, and 75–100% considerable (Higgins, Thompson, Deeks, & Altman, Reference Higgins, Thompson, Deeks and Altman2003). Heterogeneity was investigated using meta-regression for analyses with 10 studies or more implemented using the METAREG (Sharp, Reference Sharp1998) command in Stata 15. Four potential moderator variables were explored for general academic achievement: (i) type of academic assessment (i.e. national examination or other tests), based on the rationale that it may be less appropriate to compare the results of standardised academic achievement tests with those from national exams; (ii), the educational system of countries in which data were collected (i.e. Scandinavian/Nordic countries v. all other countries); (iii) the age at academic assessment (i.e. 7–12 years v. 13–16 years), as 12 years reflects the approximate age at which primary (elementary) school education concludes and we wished to determine any differences in academic underperformance between primary and secondary schooling; and (iv) NOS study quality score.
For the meta-analysis of educational level attained, in order to create equivalency across educational systems, we examined whether individuals with schizophrenia, compared to those without the disorder, were more or less likely to enter into higher education [i.e. continue education past secondary/high school (Bulgaria, France, India, Jamaica, Qatar, South Korea, Turkey, USA), past upper secondary or vocational (Denmark, Finland, Poland), past secondary senior (Netherlands), or complete greater than 12 years of education (Greece, Spain)]. Three potential effect size moderators were examined. One, in primary studies, educational level attained was measured either as a study outcome or as a socio-demographic characteristic of the sample. In the case of the former, these were objective measures of attainment, whereas the latter derived from self-reported attainment levels. Self-report may be less reliable than information derived from, or cross-referenced with, objective records; in comparison to objective measures, students self-report higher grades (Herman & Nelson, Reference Herman and Nelson2009). Two, we compared primary studies that utilised data from countries that have different ages for the end of compulsory education (i.e. 14–16 years v. 18 years). Evidence has highlighted the potential importance of secondary school attendance and attainment in influencing decisions to enter higher education. Three, we also examined the NOS study quality score.
Results
Schizophrenia and schizophrenia spectrum disorders
Search results – general academic and mathematics achievement
The literature search identified 2751 unique records, of which 27 full-text articles were assessed for eligibility (see online Supplementary Fig. S1 for screening procedure and search results). By adopting the search strategy from the original review (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012), which was not specific to academic achievement, the articles identified in the literature search included non-relevant studies of IQ and motor function which were therefore excluded during the first screening stage. One author was successfully contacted to provide summary statistics on general academic and mathematics achievement scores for youth aged 12 years who did and did not later develop schizophrenia (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017). Six new published studies met inclusion criteria for the meta-analyses: six in the general academic achievement domain (Chong et al., Reference Chong, Subramaniam, Lee, Pek, Cheok, Verma and Wong2009; Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; Schulz, Sundin, Leask, & Done, Reference Schulz, Sundin, Leask and Done2014; Seidman et al., Reference Seidman, Cherkerzian, Goldstein, Agnew-Blais, Tsuang and Buka2013; Sørensen et al., Reference Sørensen, Debost, Agerbo, Benros, McGrath, Mortensen and Petersen2018; Ullman, Hornik-Lurie, & Reichenberg, Reference Ullman, Hornik-Lurie and Reichenberg2017); and three in the mathematics achievement domain (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; Sørensen et al., Reference Sørensen, Debost, Agerbo, Benros, McGrath, Mortensen and Petersen2018; Ullman et al., Reference Ullman, Hornik-Lurie and Reichenberg2017). Table 1 outlines the details of each study, including sample characteristics, age at assessment, domain measure, and effect size of difference between youth who subsequently developed schizophrenia compared to those who did not. All studies contained mixed-gender samples, except for two that included only men (Ang & Tan, Reference Ang and Tan2004; Chong et al., Reference Chong, Subramaniam, Lee, Pek, Cheok, Verma and Wong2009). Assessments of academic achievement included results of standardised achievement tests and national examinations, as well as school tests administered at the end of the academic year. Participants were 7–16 years old at the time of the academic assessment.
Table 1. Study details and effect sizes for meta-analyses examining academic achievement in youth who subsequently developed schizophrenia or a schizophrenia spectrum disorder and in youth at-risk for schizophrenia or a schizophrenia spectrum disorder
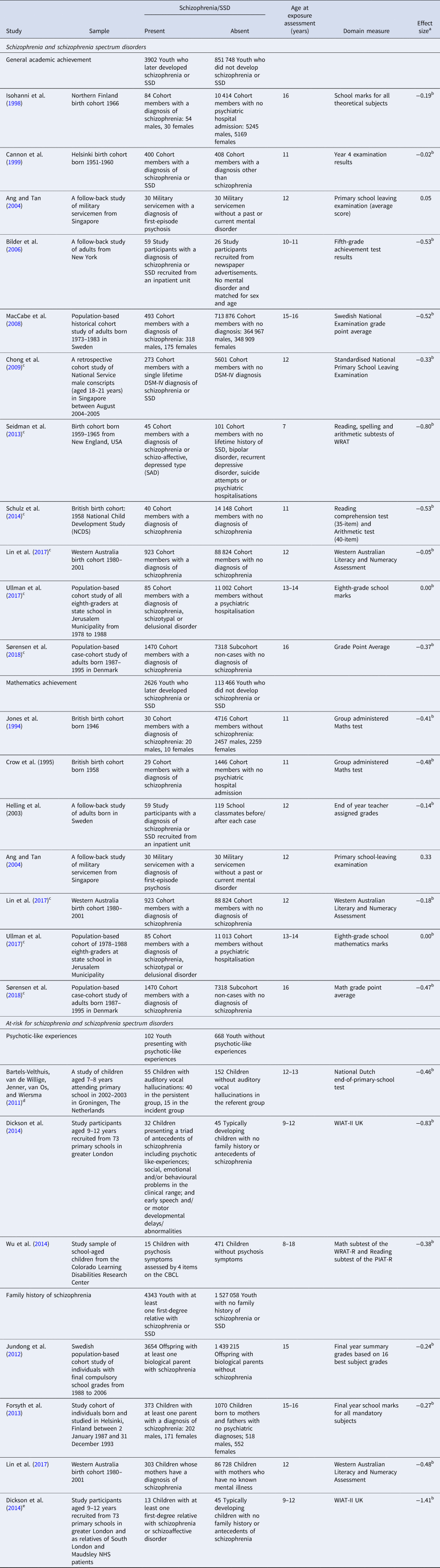
SSD, Schizophrenia spectrum disorder; WRAT, Wide Range Achievement Test; WRAT-R, Wide Range Achievement Test – Revised; PIAT-R, Peabody Individual Achievement Test – Revised; CBCL, Child Behaviour Checklist; WIAT-II UK, Wechsler Individual Achievement Test – Second UK Edition.
a Effect sizes were estimated using Cohen's d, obtained using sample sizes, means and standard deviations for a group who later developed schizophrenia or an SSD, or a group at-risk for schizophrenia or an SSD, and a comparison group, except for the following: (1) Academic performance: Mathematics : for both Jones et al. (Reference Jones, Murray, Jones, Rodgers and Marmot1994) and Helling et al. (Reference Helling, Öhman and Hultman2003), samples size and f statistics were used; and for Crow et al. (Reference Crow, Done and Sacker1995), t statistic was calculated from degrees of freedom and p value given in paper; effect size was then estimated from sample size and t statistic.
b Negative values indicate better performance in the comparison group.
c New studies included in meta-analysis.
d (i) Persistent group: Hearing voices at 7–8 years old and at least occasionally during one other year over the 5-year follow-up period (up to 12–13 years old). (ii) Incident group: Not hearing voices at 7–8 years old but positive for auditory vocal hallucinations over the 5-year follow-up period (up to 12–13 years old). (iii) Referent group: Not hearing voices at 7–8 years old and the 5-year follow-up period (up to 12–13 years old).
e The sample included two children with at least two second-degree relatives with schizophrenia or schizoaffective disorder.
General academic achievement
A meta-analysis of 11 studies, including six new studies since our previous meta-analysis (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012), indicated that individuals aged 16 years or younger who subsequently developed schizophrenia attained significantly lower general academic achievement scores than those who did not develop the disorder. Figure 1a illustrates the small effect size (d = −0.29, 95% CI −0.43 to −0.14, z = 3.95, p < 0.0001). Significant and substantial heterogeneity was identified (Q = 120.77, df = 10, p < 0.001/I 2 = 91.7%). Meta-regression analyses indicated that heterogeneity was not associated with the type of academic assessment, educational system, age at assessment, nor study quality. No small sample bias was detected (p = 0.80).

Fig. 1. Forest plots for general academic (a) and mathematics (b) achievement among youth aged 16 years or younger who subsequently developed schizophrenia or a schizophrenia spectrum disorder.
Mathematics achievement
A meta-analysis of seven studies, including three new publications since our last meta-analysis (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012), showed that individuals aged 16 years or younger who later developed schizophrenia, compared to those who did not, performed worse on tests of mathematics. Figure 1b illustrates the small effect size differences (d = −0.23, 95% CI −0.41 to −0.05, z = 2.46, p = 0.01). The results highlighted significant and substantial heterogeneity across the studies (Q = 63.54, df = 6, p < 0.001/I 2 = 91%). No small sample bias was observed (p = 0.43).
Educational level attained
The search yielded 13 088 unique studies (see online Supplementary Fig. S2 for screening procedure and search results) and 472 articles underwent full-text review. Three studies reported insufficient data to calculate an effect size: two were able to provide additional data (Stramecki et al., Reference Stramecki, Kotowicz, Piotrowski, Frydecka, Rymaszewska, Beszłej and Misiak2018; Vreeker et al., Reference Vreeker, Boks, Abramovic, Verkooijen, van Bergen, Hillegers and Investigators2016), but one was unable (Ranning et al., Reference Ranning, Laursen, Agerbo, Thorup, Hjorthøj, Jepsen and Nordentoft2017). Overall, 22 studies met inclusion criteria for the meta-analysis (see Table 2 for study details). Most studies obtained data on educational level attainment by self-report via structured interview or questionnaire, but four studies extracted data from population registers (Burgess, Curtis-Downes, & Gibson, Reference Burgess, Curtis-Downes and Gibson2013; Greve et al., Reference Greve, Mors, Mortensen, Meier, McGrath and Petersen2017; Isohanni et al., Reference Isohanni, Jones, JÄrvelin, Nieminen, Rantakallio, Jokelainen and Isohanni2001; Tempelaar et al., Reference Tempelaar, Termorshuizen, MacCabe, Boks and Kahn2017). All studies had mixed-gender samples. The comparison group of one study included first- and second-degree relatives (Duarte, Mamani, Rosales, & Kymalainen, Reference Duarte, Mamani, Rosales and Kymalainen2008). Online Supplementary Table S3 provides a description of stages of educational systems for the 15 countries of origin included within the analysis.
Table 2. Study details and effect sizes for meta-analysis examining educational level attained in individuals with an adulthood diagnosis of schizophrenia or a schizophrenia spectrum disorder

SSD, Schizophrenia spectrum disorder; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th Edition.
a Effect sizes were estimated using an odds ratio, obtained using the number of participants with higher education and total number of participants in each group of those who later developed schizophrenia or an SSD and a comparison group.
b Primary study inclusion criteria required participants to have at least two years of high school attendance (Johnson-Greene et al., Reference Johnson-Greene, Dehring, Adams, Miller, Arora, Beylin and Brandon1997) or a minimum formal education of 8 years (Veleva et al., Reference Veleva, Stoimenova and Valkova2019).
c Values below 1.00 indicate better performance in the comparison group.
Results showed that individuals with schizophrenia, compared to those without the disorder, were significantly less likely to enter into higher (post-secondary) education. As illustrated in Fig. 2, a moderate effect size was found (OR 0.49, 95% CI 0.38–0.63, z = 5.65, p < 0.0001). Significant and substantial heterogeneity was identified across studies (Q = 182.88, df = 21, p < 0.001/I 2 = 88.5%). For the meta-regression analysis of school leaving age, five studies were excluded because school leaving age could not be accurately determined (Bener, Al-Hamaq, & Dafeeah, Reference Bener, Al-Hamaq and Dafeeah2014; Burgess et al., Reference Burgess, Curtis-Downes and Gibson2013; Cohen, Dembling, & Schorling, Reference Cohen, Dembling and Schorling2002; Duarte et al., Reference Duarte, Mamani, Rosales and Kymalainen2008; Johnson-Greene et al., Reference Johnson-Greene, Dehring, Adams, Miller, Arora, Beylin and Brandon1997). Meta-regression indicated that neither the measure of educational level used, school leave age, nor study quality were associated with heterogeneity. No significant small sample bias was detected (p = 0.60).

Fig. 2. Forest plot for educational level attained among individuals with an adulthood diagnosis of schizophrenia or a schizophrenia spectrum disorder.
Youth at-risk for schizophrenia and schizophrenia spectrum disorders
Psychotic-like experiences
From 414 unique articles detected, full-text screening was carried out for seven studies (see online Supplementary Fig. S4 for screening procedure and search results). One study reported insufficient data to calculate an effect size and, upon contact, was unable to provide the necessary data (Ramsay et al., Reference Ramsay, Barnett, Murray, Miettunen, Mäki, Järvelin and Veijola2018). Table 1 provides details of the three studies included in the meta-analysis. Academic achievement scores were collected concurrently with symptoms and included the results of national exams and standardised achievement tests. The results demonstrated poorer overall academic achievement in youth with PLEs compared to youth without PLEs (see Fig. 3a). A moderate effect size was obtained (d = −0.54, 95% CI −0.77 to −0.30, z = 4.41, p < 0.001). No significant heterogeneity was detected (Q = 2.09, df = 2, p = 0.35/I 2 = 3.6%).
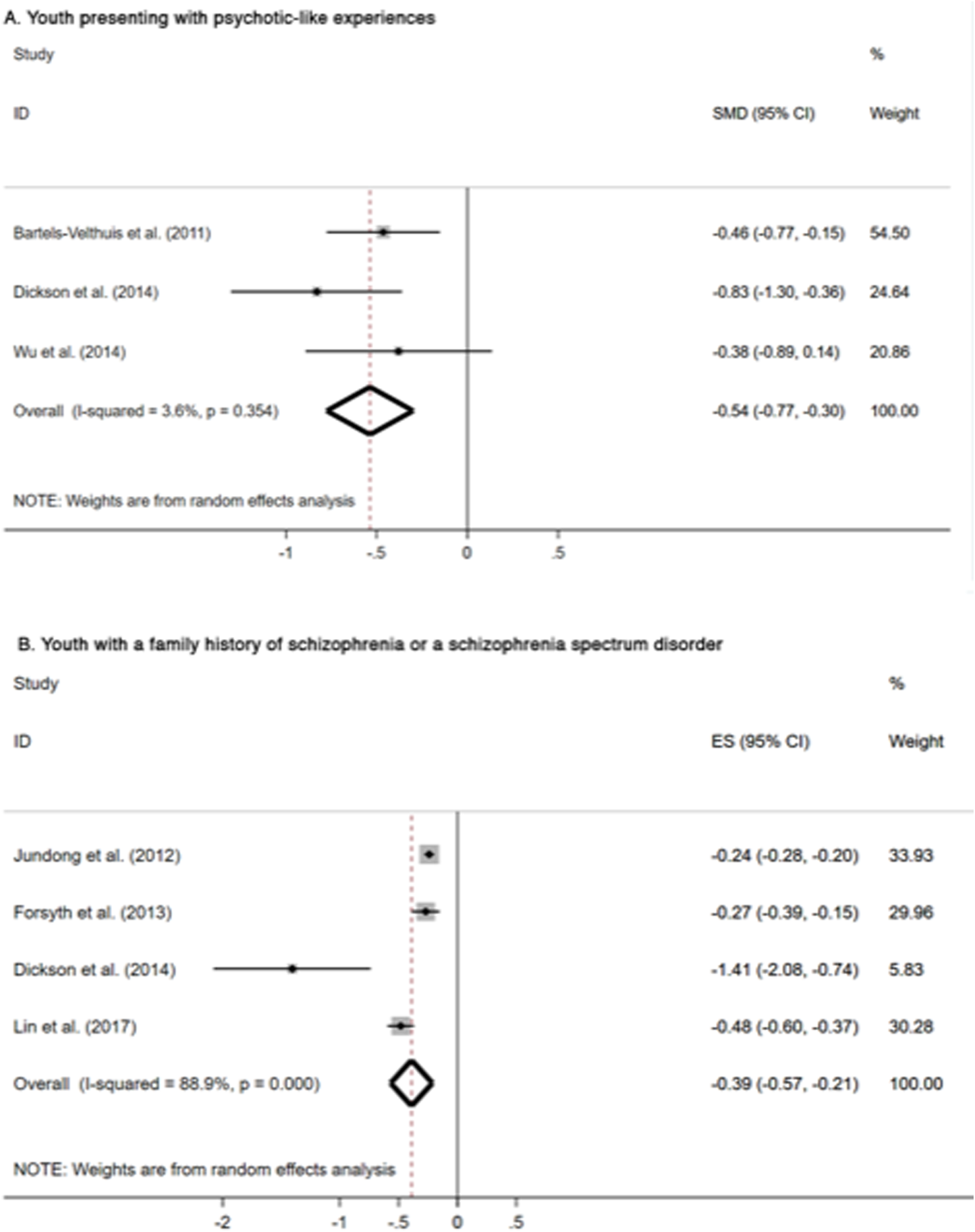
Fig. 3. Forest plot for general academic achievement among youth presenting with psychotic-like experiences (a) and youth with a family history of schizophrenia or a schizophrenia spectrum disorder (b).
Family history of schizophrenia
The literature search identified 1403 unique articles. Following the full-text screening of 19 articles, 15 were excluded for reasons detailed in online Supplementary Fig. S5. Two authors were contacted for additional information (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; Ranning et al., Reference Ranning, Laursen, Agerbo, Thorup, Hjorthøj, Jepsen and Nordentoft2017), one provided data suitable for meta-analysis (Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017). Four studies met inclusion criteria and are described in Table 1. Assessments of academic achievement included standardised assessments or exams, and grades from the final year of compulsory school. The meta-analysis indicated that youth with at least one first-degree relative with schizophrenia, compared to those without, obtained lower general academic achievement scores. Figure 3b demonstrates the moderate effect size of group difference (d = −0.39, 95% CI −0.57 to −0.21, z = 4.31, p < 0.0001). Significant and substantial heterogeneity was detected across the studies (Q = 26.99, df = 3, p < 0.001/I 2 = 88.9%).
Quality of included studies
For the updated general and mathematics achievement and educational level meta-analyses, total scores from NOS assessment ranged from three (Burgess et al., Reference Burgess, Curtis-Downes and Gibson2013; Rathor, Dave, Mehta, Oswal, & Gupta, Reference Rathor, Dave, Mehta, Oswal and Gupta2008) to nine (Ang & Tan, Reference Ang and Tan2004; Isohanni et al., Reference Isohanni, JÄrvelin, Nieminen, Jones, Rantakallio, Jokelainen and Isohanni1998, Reference Isohanni, Jones, JÄrvelin, Nieminen, Rantakallio, Jokelainen and Isohanni2001), with the most common score being seven. For the meta-analysis of individuals at-risk for schizophrenia, all studies achieved a total score of seven or eight (see online Supplementary Tables S6 and S7).
Discussion
These meta-analyses, comprising data from more than four million individuals, comprehensively explored whether individuals with a diagnosis of schizophrenia and children/adolescents at-risk for the disorder are characterised by academic underachievement. The findings demonstrated that, by age 16 years, children and adolescents who later develop the disorder presented with significantly poorer general academic and mathematics achievement compared to individuals who did not develop schizophrenia. Individuals with schizophrenia were also less likely to enter higher education than individuals without the disorder. Furthermore, youth considered to be at-risk for schizophrenia because they reported PLEs or had an affected first-degree family member performed more poorly at school relative to their typically developing peers. Together, these findings suggest that poor academic achievement may represent a readily identifiable premorbid cognitive marker of vulnerability for later schizophrenia.
Although effect sizes were small in magnitude, our finding of poor general academic (d = -0.29) and mathematics achievement (d = -0.23) among individuals who later developed schizophrenia is inconsistent with the results of our previous meta-analyses (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012). This may be due to increased statistical power afforded by the additional studies (n = 6) in random-effects meta-analyses (Jackson & Turner, Reference Jackson and Turner2017). Some studies reported poor performance in children who developed schizophrenia relative to those who do not in specific academic subjects only (Bilder et al., Reference Bilder, Reiter, Bates, Lencz, Szeszko, Goldman and Kane2006; Fuller et al., Reference Fuller, Nopoulos, Arndt, O'Leary, Ho and Andreasen2002; Lin et al., Reference Lin, Di Prinzio, Young, Jacoby, Whitehouse, Waters and Morgan2017; MacCabe et al., Reference MacCabe, Lambe, Cnattingius, Torrång, Björk, Sham and Hultman2008). Our findings instead support a more generalised cognitive deficit preceding the diagnosis of schizophrenia (Sheffield et al., Reference Sheffield, Karcher and Barch2018). Meta-regression analyses comparing studies examining general academic achievement between 7–12 and 13–16 years indicated that age was not an effect modifier, suggesting that this underachievement may be measurable from middle childhood among individuals who go onto develop schizophrenia in adulthood. This observed deficit spanning 7–16 years (i.e. where lower academic achievement is present early and continues), contrasts with other research suggesting that poor academic achievement may be detectable only later in adolescence, closer to the putative prodromal period immediately preceding illness onset (Ang & Tan, Reference Ang and Tan2004; Cannon et al., Reference Cannon, Jones, Huttunen, Tanskanen, Huttunen, Rabe-Hesketh and Murray1999; Fuller et al., Reference Fuller, Nopoulos, Arndt, O'Leary, Ho and Andreasen2002; Jones, Murray, Jones, Rodgers, & Marmot, Reference Jones, Murray, Jones, Rodgers and Marmot1994; Ullman, Levine, Reichenberg, & Rabinowitz, Reference Ullman, Levine, Reichenberg and Rabinowitz2012). Our meta-analyses utilised cross-sectional data, and only longitudinal studies can truly determine whether a child who goes onto develop schizophrenia displays poor academic achievement at different ages and developmental stages (Dickson et al., Reference Dickson, Cullen, Jones, Reichenberg, Roberts, Hodgins and Laurens2018).
In the present study, we observed significant heterogeneity in both general and mathematics achievement domains, which has been suggested previously to reflect differences in educational systems (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012; MacCabe, Reference MacCabe2008). Scandinavian and Nordic countries form a small set of educational systems that are each relatively culturally and linguistically homogenous that are reported to be among the best in the world (Gustafsson & Blömeke, Reference Gustafsson and Blömeke2018). In the present study, heterogeneity in the general academic achievement domain was not due to differences between studies originating from Scandinavian/Nordic countries and those from UK, USA, Australia, Israel, and Singapore although differences between the educational systems coded as ‘other’ may have obscured our results. Possibly, the heterogeneity reflects differences in the organisation and governance of school systems (Woessmann, Reference Woessmann2016) and/or unobserved country-level heterogeneity such as cultural traits and the value placed on academic achievement (Gustafsson & Blömeke, Reference Gustafsson and Blömeke2018). We also found that assessment type (i.e. national exams v. standardised measures of academic achievement) was not an effect modifier. Standardised academic achievement tests like the Wide Range Achievement Test (WRAT; Wilkinson and Robertson, Reference Wilkinson and Robertson2006) and Wechsler Individual Achievement Test (WIAT; Wechsler, Reference Wechsler1992) are used in both educational and research settings to assess academic achievement in children and adolescents with and without special educational needs and correlate moderately with exam performance (Langberg et al., Reference Langberg, Molina, Arnold, Epstein, Altaye, Hinshaw and Hechtman2011). There is robust evidence that individuals with schizophrenia show premorbid cognitive impairments (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012; Sheffield et al., Reference Sheffield, Karcher and Barch2018), but it is not generally feasible to administer cognitive batteries that include measures of academic achievement at a population-level. It is increasingly recognised that schools have the potential to serve as a universal access point for the early detection of mental health difficulties (Levitt, Saka, Hunter Romanelli, & Hoagwood, Reference Levitt, Saka, Hunter Romanelli and Hoagwood2007; McCormick, Thompson, Stoep, & McCauley, Reference McCormick, Thompson, Stoep and McCauley2009). Our meta-analyses imply that it may be possible to use academic achievement, measured by performance in national examinations undertaken before pupils transition to secondary school, in conjunction with other known risk factors (Laurens & Cullen, Reference Laurens and Cullen2016), to develop screening programmes aimed at identifying vulnerable pupils who may experience elevated risk for the later development of schizophrenia.
Consistent with findings from the meta-analyses of academic achievement, individuals with an adulthood diagnosis of schizophrenia were less likely to enter higher education compared to those without the disorder. As individuals generally enter higher education aged 18 years and older, our results may be associated with the emergence of prodromal symptoms, typically during late adolescence and early adulthood. Measures of educational level as a study outcome (objective measures v. self-reported socio-demographic variable), and compulsory school leaving age, were not found to effect modifiers. This was unexpected, as self-report methods are reported to less reliably measure academic achievement than routinely collected administrative information on exam performance (Herman & Nelson, Reference Herman and Nelson2009), and increases in the compulsory school leaving age have historically led to increases in enrolment in higher education (Messacar & Oreopoulos, Reference Messacar and Oreopoulos2013). Meta-regression analyses are typically under powered even with at least 10 studies available, and the lack of effect modification here may reflect the presence of type II errors (Hempel et al., Reference Hempel, Miles, Booth, Wang, Morton and Shekelle2013). Our present findings indicate that the attainment deficit is observed regardless of the measure used.
We found medium effect size differences in general academic achievement among 4445 at-risk youth aged 16 years and younger (PLEs: d = −0.54; affected first-degree relative: d = −0.39) compared to 1 527 726 youth not at-risk for the disorder. The magnitude of cognitive impairments is suggested to increase across illness stages in schizophrenia; that is, increasing in size across premorbid, prodromal, first-episode, and chronic stages (Mollon & Reichenberg, Reference Mollon and Reichenberg2017; Sheffield et al., Reference Sheffield, Karcher and Barch2018). Although only a minority of youth with PLEs or a family history of schizophrenia will go onto develop schizophrenia (Mortensen, Pedersen, & Pedersen, Reference Mortensen, Pedersen and Pedersen2009; Werbeloff et al., Reference Werbeloff, Drukker, Dohrenwend, Levav, Yoffe, van Os and Weiser2012), we observed larger effect size differences among at-risk youth relative to their typically developing peers than was obtained for the prospective assessments of youth who went onto develop schizophrenia relative to youth who did not. There are four possible explanations for these findings. One, given the small number of studies included in both at-risk meta-analyses, our results may reflect the inclusion of a study with a small sample size that utilised standardised measures of academic achievement and reported large effect sizes differences (Dickson et al., Reference Dickson, Cullen, Reichenberg, Hodgins, Campbell, Morris and Laurens2014). Two, children experiencing PLEs and children with a family history of schizophrenia are more likely to present with externalising and internalising psychopathology (Lancefield, Raudino, Downs, & Laurens, Reference Lancefield, Raudino, Downs and Laurens2016; Laurens et al., Reference Laurens, Tzoumakis, Dean, Harris, Carr and Green2020; Sandstrom et al., Reference Sandstrom, MacKenzie, Pizzo, Fine, Rempel, Howard and Pavlova2019), which in turn has been reported to be associated with academic achievement and educational attainment (Masten et al., Reference Masten, Roisman, Long, Burt, Obradović, Riley and Tellegen2005; Melkevik, Nilsen, Evensen, Reneflot, & Mykletun, Reference Melkevik, Nilsen, Evensen, Reneflot and Mykletun2016). Three, some evidence suggests that type of comparison group (e.g. healthy selected controls v. unselected cohorts) maybe an effect modifier of the association between premorbid general intelligence and schizophrenia (Dickson et al., Reference Dickson, Laurens, Cullen and Hodgins2012; Woodberry, Giuliano, & Seidman, Reference Woodberry, Giuliano and Seidman2008); however, due to the small number of studies included in the at-risk meta-analyses, it was not possible to investigate this potential source of heterogeneity. Four, the effect of an unmeasured publication bias in which published negative findings from samples of at-risk youth are less likely relative to prospective longitudinal studies of individuals who later develop schizophrenia.
Our study comprehensively examined both academic achievement and education level attained among individuals with schizophrenia, and academic achievement in those at-risk for the disorder and, in doing so, examined over four million individuals, of whom 13 179 had a diagnosis of schizophrenia and 4445 were deemed to be at-risk. That we were able to examine a range of potential effect modifiers (i.e. educational system, assessment type, age, measurement of educational level, school leaving age, and study quality) was a further strength of the study. However, three limitations must be noted. One, our findings for meta-analyses examining academic achievement may reflect differences in marking systems employed in the countries included. For example, a peer-referencing system (i.e. comparing the performance of a pupil to peers) was used widely in schools in the USA and Sweden up to 1997, but a criterion-referencing system (i.e. performance that is measured against pre-determined criteria) is used to assess pupils' performance in UK primary schools. A peer-referencing system may be associated with grade inflation (Kendler et al., Reference Kendler, Ohlsson, Mezuk, Sundquist and Sundquist2016). It was not possible to account for these changes to, and differences in, marking systems in the present study, so the impact on our results is not clear. Two, our search strategy highlighted the different ways in which educational attainment is reported as a sample descriptive variable and will have failed to identify some relevant studies reporting level of educational attainment. Nonetheless, the electronic database search identified over 13 000 articles, and it was not feasible to further broaden our search strategy. Three, our findings may be confounded by the age of onset of schizophrenia, as the typical age range of individuals in higher education overlaps with the peak period of onset of the disorder.
Conclusion
Our meta-analyses show that academic and educational underachievement precedes adult-onset schizophrenia. Youth at-risk for the disorder, compared to those who are not, are likewise characterised by poor academic achievement. Although we observed significant heterogeneity across studies, and effect sizes were small to moderate in magnitude only, future research could investigate whether it is feasible to develop a tool using academic achievement and other known antecedents of the disorder to help identify at-risk pupils and thereby facilitate their access to early treatment and preventative inventions well before the onset of schizophrenia.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291720002354.
Acknowledgements
The authors would like to thank A. Lin, A. Vreeker, F. Stramecki, R. Kahn and M. Boks for providing the additional data necessary to complete the meta-analyses. HD, JHM and MJK are affiliated with the National Institute for Health Research (NIHR) Specialist Biomedical Research Centre for Mental Health at the South London and Maudsley NHS Foundation Trust and Institute of Psychiatry, Psychology & Neuroscience, King's College London, United Kingdom. AEC was supported by a Sir Henry Wellcome Postdoctoral Fellowship (107395/Z/15/Z) and a NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation (28336). JD is supported by NIHR Clinician Science Fellowship award (CS-2018-18-ST2-014) and has received support from a Medical Research Council (MRC) Clinical Research Training Fellowship (MR/L017105/1) and Psychiatry Research Trust Peggy Pollak Research Fellowship in Developmental Psychiatry. KRL was supported by an Australian Research Council Future Fellowship (FT170100294).
Conflicts of interest
None.







