



Introduction
Previous literature has characterized hospitals as vulnerable targets for terrorist attacks.Reference De Cauwer, Somville, Sabbe and Mortelmans1 Unfortunately, the very characteristics that make hospitals so valuable to their communities are also what make them “soft targets.” Hospitals are valued for their role as a social safety net, where people of all races, religious beliefs, and backgrounds can safely seek health care. As a result, hospitals are easily accessible to the public and are typically crowded with patients, staff, and care providers, 24 hours a day, 365 days a year, and often with less security than a government or military building.Reference Martin2 In addition, hospitals contain a dense array of resources, both physical and personal, which allows them to simultaneously provide advanced specialty care, operative interventions, and other health care resources. In previous work, researchers have analyzed attacks on health care facilities and infrastructure in general.Reference Cavaliere, Alfalasi, Jasani, Ciottone and Lawner3,Reference Jasani, Alfalasi, Cavaliere, Ciottone and Lawner4 This analysis seeks to review the data and trends on terrorist attacks involving hospitals specifically.
When a terrorist attack occurs in the community, hospitals mobilize staff and resources to provide care to the wounded. When hospitals themselves become the target, however, this fundamental component of disaster response is undermined.Reference Tin, Hart and Ciottone5 The resultant chaos and destruction of hospital staff, supplies, and infrastructure disrupts the hospital’s capability to provide emergent medical attention to the wounded. In addition, pre-existing patients that were already being treated within the facility are particularly vulnerable during an attack, both due to their underlying medical conditions as well as their limited mobility.Reference Ganor and Wernli6 They may also have unique and complicated medical needs, making it difficult to coordinate continued care, transport, or transfer of care.Reference Hancock and Johnson7
Terrorist attacks on hospitals have unique second- and third-order effects.Reference O’Reilly, Brohi, Shapira, Hammond and Cole8 Among these are interruptions to the routine care of patients that were not the primary victims of the attack. This can come as a result of the destruction of infrastructure and personnel as well as the depletion or destruction of medical supplies. There can also be significant psychological effects when hospitals are attacked. As in any terrorist attack, there is the post-traumatic stress inflicted on the survivors and witnesses of the attack as well as those who responded to it.Reference Ellenberg, Taragin and Ostfeld9,10 However, the unique perversity of attacking a hospital, combined with the prominence that hospitals occupy within the community, all but guarantees that the impact of the attack will be amplified by wide-spread media coverage.Reference Ganor and Wernli6 This may contribute to an additional psychological toll on the greater community due to personalization, a phenomenon in which the viewer’s familiarization with the target evokes a fear that they could have easily been a victim.Reference Ganor and Wernli6 Indeed, prior research has revealed that there is a decrease in health care utilization following a terrorist attack.Reference Green, Buehler and Silk11,Reference Ekström, Eng-Larsson and Isaksson12 While it is unclear if this decline is due to an undermining of the public’s sense of security when seeking medical attention, it nonetheless has the potential to lead to additional indirect causalities as a consequence of unnecessary delays in care.
Hospitals represent high-value, vulnerable targets. Proactive steps must be taken on both the community and national level in order to protect hospitals against future terrorist attacks. Reviewing past attacks against health care facilities is the first step in identifying patterns that could help mitigate or prevent future attacks.
Methods
A focused search of the Global Terrorism Database (GTD) was performed to identify terrorist attacks against hospitals throughout the world. The GTD is made available by the National Consortium for the Study of Terrorism Response (START; University of Maryland; Baltimore, Maryland USA) and is part of the US Department of Homeland Security (Washington, DC USA).13 The GTD is an unclassified, open-source database which has documented the terrorist events that have occurred around the world dating back to 1970.
The START program provides an open-source link to the GTD database as well as its dictionary, inclusion/exclusion criteria, and descriptions of how it sources raw data. The GTD data are collected at a lag behind real time in order to ensure accurate reporting, and entries are not added unless they are documented by at least one independent, highly valid source. The validity of each source document is scored and taken into account at each stage of the data collection process. Missing information is left blank in the database, and the GTD is regularly updated as new information becomes available. Coding is completed by teams, each specializing in a particular domain of the GTD Codebook. Each team is led by a full-time research assistant who is responsible for training and supervising the team members as well as ensuring the quality of the coded data.
In order to satisfy the database’s inclusion criteria, the incident must meet the following broad definition: a threatened or actual use of illegal force and violence by a non-state actor to attain a political, economic, religious, or social goal through fear, coercion, or intimidation. Additional inclusion criteria are outlined in Table 1. Incidents that satisfied inclusion criteria were evaluated manually by GTD coders for definitional overlap with other forms of crime and political violence (eg, insurgency, hate crime, and organized crime).
Table 1. Inclusion Criteria

The initial review/query yielded 191,465 results in total. These entries were then searched for incidents that contained the term “hospital” within one or more of the columns designated for target description. This yielded 430 separate terrorist attacks, with accompanying data regarding attack type, date, armament, country, casualties, affiliated group, and more. These data were then fully extracted to be further analyzed.
The study was reviewed by the University of Maryland, Baltimore Institutional Review Board and deemed to be exempt from review.
Results
A total of 430 attacks were identified in the GTD involving the purposeful targeting of hospitals by terrorist groups. In total, the direct impact of these attacks resulted in 1,291 deaths and an additional 1,921 wounded. Almost two-thirds of these attacks (n = 276) occurred in the final decade of this study, between the years 2009-2018. By comparison, there were only 154 terrorist attacks on hospitals that occurred during the first 39 years of this study, between 1970-2008 (Figure 1).

Figure 1. Cumulative Number of Terrorist Attacks on Hospitals: 1970-2018.
Between 1970 and 1999, there was an average of 3.3 hospital attacks per year with no more than nine attacks occurring in any single year (Figure 2). In the following decade from 2000-2009, the average number of attacks rose to 7.8 with an inflection point around the year 2008, which recorded 15 hospital attacks. From 2010-2018, the average climbed to 28.2 attacks per year, over eight-times higher than the average prior to the turn of the century. The year 2014 saw the largest number of attacks of any single year with 49 attacks recorded. While there was an increase in terrorist attacks against all target types over the past two decades, there had been a disproportionate increase in the occurrence of attacks on hospitals specifically (Figure 3).14

Figure 2. Terrorist Attacks Against Hospitals Per Year: 1970-2018.
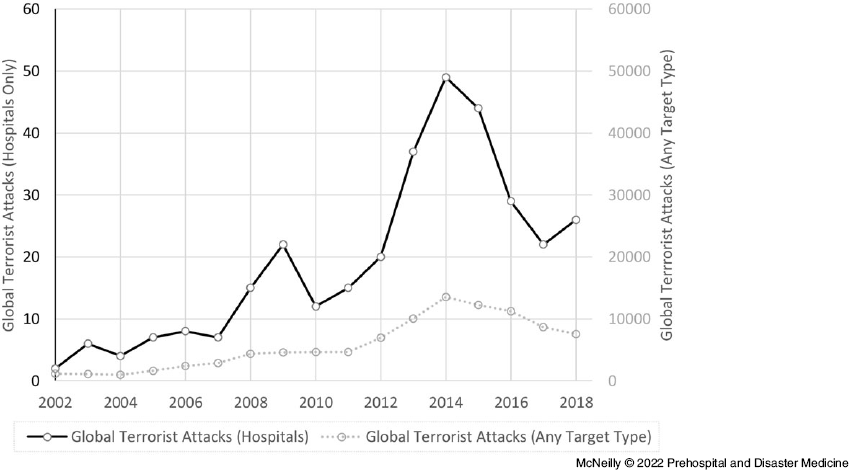
Figure 3. Global Terrorist Attacks Per Year: 2002-2018.
Attacks had been carried out against hospitals in 61 countries (Figure 4). Iraq had recorded the greatest number of attacks on hospitals with 64 recorded, all occurring after 2004. Pakistan had seen the second most attacks with 48 recorded. Attacks had occurred on every inhabited continent except Australia.

Figure 4. Terrorist Attacks Against Hospitals, by Country (Top 22).
The most commonly used method to carry out terrorist attacks on hospitals was “bombing/explosion,” which accounted for 299 of the attacks (Figure 5). Other methods employed included “armed assault” (75), “hostage taking” (17), “facility/infrastructure attack” (5), and “unarmed assault” (3). Terrorist groups used a variety of armaments to carry out their attacks (Figure 6). Explosive devices of unspecified type were the most frequently employed armament, accounting for 121 of the attacks. Projectiles, including rocket-propelled grenades (RPGs), rockets, and others, were used in 69 separate attacks, while grenades were used in 28 attacks. Vehicle-borne bombs accounted for 51 of the attacks and suicide bombers carried out an additional 23 attacks. In those attacks which utilized firearms, semi-automatic and fully automatic rifles (24) were used more frequently than handguns (8).

Figure 5. Method of Terrorist Attacks Against Hospitals.

Figure 6. Armament Employed in Terrorist Attacks Against Hospitals.
Abbreviation: RPG, rocket-propelled grenade.
Over 90 different organizations had carried out attacks against hospitals. The majority of attacks against hospitals were carried out by unknown entities (227). Of the specific groups that have been identified in the GTD, “Houthi extremists (Anshar Allah)” had carried out 21 attacks killing 28 and wounding 118 (Figure 7). “Islamic State of Iraq and the Levant (ISIL)” carried out 18 attacks killing 135 and wounding 213, while “Boko Haram” carried out nine attacks that killed 39 and wounded 15. “Al-Qaida” affiliates carried out seven attacks killing 21 and wounding 17. The Taliban carried out seven attacks against hospitals, killing 25 and wounding 62.

Figure 7. Most Commonly Cited Groups Responsible for Terrorist Attacks on Hospitals.
Discussion
Hospitals provide critical services to their surrounding communities. Life-saving and life-sustaining functions of hospitals are in a state of continuous operation. The need for all-hours access by the general public renders these facilities vulnerable to direct hostile action. Damage from a terrorist attack extends beyond immediate civilian casualties. A significant attack can cripple a community’s health care infrastructure and affect future emergency response functions.
From 1970 through 2018, 430 terrorist attacks were carried out on hospitals across 61 different countries, killing 1,219 people and wounding 1,921 others. Iraq suffered the largest number of terrorist attacks on hospital with 64 recorded in the GTD; however, attacks have occurred on every inhabited continent with the exception of Australia (Figure 4). The majority of all attacks were carried out by unaffiliated or unidentified groups (Figure 7). Of the attacks waged by known terrorist groups, Houthi extremists and ISIL carried out the greatest number of attacks.
Looking at the number of attacks shows a troubling trend. The occurrence of hospital attacks has increased drastically over the last two decades (Figure 2). Between the years 2010-2018, the average rate of terrorist attacks rose to 28.2 attacks per year. This represents over an eight-fold increase from the average taken prior to the turn of the century between the years 1970-1999. While it is true that the rate of global terrorist attacks against all target types has increased in general over the past two decades, there has been a disproportionate rise in the rate of attacks on hospitals (Figure 3).
This trend points to the overall vulnerability of hospitals as well as the need to further consider how and why terrorists prioritize targeting hospitals over other targets. Terrorist organizations, unlike traditional military forces, are not bound by the Geneva Convention, which prohibits the intentional targeting of hospitals. As discussed above, the vulnerability of hospitals to attack is well-known and these concerns have been raised in both medical and security capacities.
Unfortunately, hardening hospital defenses and developing robust response plans will be challenging as terrorist organizations have utilized a myriad of methods to carry out their attacks (Figure 3). The majority of the attacks listed in the GTD were carried out with explosives. This is an important consideration when planning for future improvements to the security of hospitals as it may warrant different screening methods at hospital entrances than those which would be used for concealed weapons, such as handguns, which surprisingly were used in the minority of cases (Figure 6). Vehicle-borne explosive devices and suicide attacks, which were both common methods of attack (51 and 23 instances, respectively), are particularly challenging to prevent, especially if the parking structures and screening areas are located within the footprint of the hospital building. Additionally, as Jasani, et al have previously highlighted, terrorist organizations have used ambulances to carry out attacks.Reference Jasani, Alfalasi, Cavaliere, Ciottone and Lawner4 This would present a major security concern as ambulances frequently come to and from the hospital and are rarely the subject of security screening. Projectiles such as RPGs, rockets, and mortars were also frequently used and pose a challenge in that even if the hospital grounds have a robust security system in place, an attack can still be launched from outside its perimeter (Figure 4).
Strategies for hardening hospital defenses against terrorist attacks are numerous and a full discussion of them is beyond the scope of this paper; however, a brief discussion of several key considerations is offered here. These include increasing the visibility of uniformed security personnel and surveillance cameras in order to deter both terrorist reconnaissance and attacks.Reference Schmid15 Given that explosives are the most commonly employed weapons in hospital attacks, the creation of buffer zones between patient care areas and parking structures, as well as vehicle and pedestrian traffic, may help mitigate the effects of any bomb planted on the perimeter of the facility. Similarly, patient and visitor foot traffic could be channeled in a way that reduces walkway congestion and crowding in waiting rooms. Given the follow-on affects that occur in the aftermath of a hospital attack (as discussed above), an inter-facility plan of action should be considered in addition to any intra-facility plan so that surrounding hospitals can shift and cover-down on patient care when a nearby hospital is attacked. The increasing incidence of terrorist attacks on hospitals and their current vulnerability warrant a more in-depth and comprehensive discussion of these defense hardening strategies, as well as others, and is part of the basis for the emerging health care initiative for the development of Counter-Terrorism Medicine (CTM) as a distinct sub-specialty of Disaster Medicine (DM), as laid out by Court, et al.Reference Court, Edwards, Issa, Voskanyan and Ciottone16 Efforts to harden hospital defenses carry with them the significant risk of hindering the public’s access to patient care. As such, patient accessibility needs to be deliberately considered while developing future security and defense strategies.
Limitations
This retrospective analysis focuses only on those hospital attacks that meet GTD criteria for an act of terror. As a result, this study under-estimates the overall vulnerability of hospitals to attack. For example, attacks that are perpetrated by lone gunmen acting on personal motivations are not deemed as acts of terror. A quantitative content analysis of reports involving shootings in US hospitals from 2012-2016 found a total of 88 attacks, most of which were motivated by a “grudge” or “suicide” and none of which met the criteria for an act of terrorism.Reference Wax, Cartin, Craig and Pinette17 Similarly, the current review excluded nationally sponsored attacks on hospitals. These include attacks that occurred within the broader scope of conflicts recognized as political wars, including civil wars. For example, during the Syrian Civil War, Physicians for Human Rights (Boston, Massachusetts USA) documented 600 attacks on 350 separate health care facilities, leading to the death of 930 medical personnel, most of which were perpetrated by nationally sponsored actors and were therefore not included in this review.18 Additionally, in resource-poor regions of the world, there may be a degree of under-reporting due to a lack of media and/or government agencies that keep records of such occurrences. Finally, only direct casualties of terrorist attacks are reported, though as discussed above, hospital attacks have delayed secondary and tertiary impacts on the health of the communities they serve. In light of the above omissions, it is important to recognize that this analysis significantly under-estimates the overall vulnerability of hospitals to violent attacks.
Conclusion
There has been a disproportionate rise in the frequency of terrorist attacks on hospitals when compared to other target types, highlighting the vulnerability of these key structures. Unsurprisingly, these attacks have inflicted large casualty counts in addition to disrupting community health care and disaster response. Attacks against hospitals have been reported on every inhabited continent except Australia, making their protection a matter of international security. The rate of terrorist attacks on hospitals has increased dramatically over the last two decades, creating an urgent need to develop improved defense strategies that will better ensure their protection.
Conflicts of interest
The authors declare none.








