


Introduction
In jurisdictions that follow international trauma guidelines, the treatment for any patient with a suspected traumatic spine injury has long been standardized and uniform: immobilization on a long backboard with a cervical collar and head blocks.Reference Pryce and McDonald 1 , 2 This treatment is presumed to protect patients from additional traumatic injury – that is, new or worsened neurologic deficit caused by movement of an injured spinal column. This standard of care currently is undergoing fundamental revision. A number of recent position statements have suggested that alternative forms of immobilization may be appropriate for certain low-risk patients.Reference McSwain, Salomone and Pons 3 - Reference Moss, Porter and Greaves 7 In some jurisdictions, patients who meet low-risk criteria are now transported with a cervical collar only, or with alternative forms of spinal motion restriction. 4 , Reference Alson and Copeland 8
In this context of evolving standards, current guidelines call for more research, or specifically for Emergency Medical Services (EMS) medical directors to provide evidence-based protocols and procedures for the treatment of potentially spine-injured patients. 4 - Reference Connor, Greaves, Porter and Bloch 6 , Reference Morrissey, Kusel and Sporer 9 The existing research on immobilization techniques, however, shows a number of gaps in the evidence base in terms of both practice and theory. At a practical level, Voss et al systematically review the methodology of immobilization studies and identify several limitations in the current research. 10 These include, among others: a lack of information about subject characteristics; a lack of standardized instructions for patient movement and effort; and a general lack of experimental design that replicates the experience of actual trauma patients in realistic settings. With regard to patient movement, there is no consensus on whether to investigate passive or active motion. Among those that measure active motion, few explore the significance of instructions given to participants or of the amount of effort they apply. The effect of participant effort has been postulated as a source of variance in published results.Reference Voss, Page and Benger 11 - Reference Manix 13 With regard to setting, trends toward investigating motion in real-life scenarios (examining, for example: vehicle extraction,Reference Sarig-Bahat, Weiss and Laufer 14 - Reference Engsberg, Standeven, Shurtleff, Eggars, Shafer and Naunheim 16 athletic equipment,Reference Shafer and Naunheim 17 , Reference Decoster, Burns and Swartz 18 vehicle motion,Reference Treme, Diduch, Hart, Romness, Kwon and Hart 19 and uncooperative patients Reference Perry, McLellan, McIlroy, Maki, Schwartz and Fernie 20 ) are in some cases limited by measurement techniques that cannot be applied practically outside of the laboratory.
At a theoretic level, it remains unclear what type of motion has the potential to cause additional traumatic injury. Existing research almost exclusively measures angular displacement (rotation of the head in relation to the body). 10 Angular displacement alone, however, does not describe the variety of observed patient movements fully in actual immobilization conditions. Patients can, for example, move quickly or slowly, with great force or little, without moving far. Recognizing this, it has also been argued that displacement does not explain additional traumatic injury, but rather that the amount of force applied across an unstable segment is the key determinant of neurologic deterioration. 4 , Reference Boissy, Shrier and Briere 21 In addition to displacement, then, other variables are required to describe patient movement while immobilized, whether this motion is passive (from events such as jostling, drops, or vehicle motion) or active (non-compliant patients working against immobilization devices). Outside of the spine-immobilization literature, linear acceleration is used to quantify a diverse array of human motion. The techniques to measure acceleration are well established and have been used in studies examining gait,Reference Hauswald 22 physical activity,Reference Tao, Liu, Zheng and Feng 23 upper extremity motion,Reference Troiano, Berrigan, Dodd, Masse, Tilert and McDowell 24 head trauma,Reference Gottlieb, Corcos and Agarwal 25 , Reference Rowson and Duma 26 and even the movement of lumbar vertebrae.Reference Wilcox, Beckwith and Greenwald 27 Investigations of potentially harmful motion in spine-injured patients would benefit from including acceleration to complement displacement as a descriptive variable.
The aim of the current study was to develop a technique for measuring head and neck motion that would both investigate spinal immobilization (SI) in clinically relevant ways and address identified methodological limitations. To do so, it attempted to standardize participant motion by specifying gradations of effort and controlling for participant characteristics. It gathered data on realistic, continuous movements that approximate actual patient movement while immobilized. Additionally, it aimed to characterize active motion in terms of both displacement and acceleration. To meet these goals, this study used a system of wireless, triaxial accelerometers, which, along with other inertial measurements units (IMUs – devices comprised of accelerometers, gyroscopes, and/or magnetometers), have seen comparatively limited use in SI literature.Reference Perry, McLellan, McIlroy, Maki, Schwartz and Fernie 20 These techniques have the potential to answer a call for “portable or multiple-modality technology that can be used to accurately evaluate devices and procedures that are designed to protect the cervical spine in trauma care.” 10 (p Reference White, Domeier and Millin 5 )
Methods
A sample of 13 participants (male=10; characteristics described in Table 1) provided informed consent. Ethical approval was obtained from the institutional Human Research Ethics Board at the University of Winnipeg (Winnipeg, Manitoba, Canada; #00609).
Table 1 Participant Characteristics

Abbreviation: BMI, body mass index.
Protocol
Participants performed a series of single- and multi-planar head movements across three conditions: no SI; wearing a cervical collar (Ambu Perfit ACE, Ambu, Inc.; Ballerup, Denmark); and full immobilization, consisting of a rigid backboard (Pro-lite Spine Board, Rapid Deployment Products; Ivyland, Pennsylvania USA) and cervical collar. Participants were fitted for the cervical collar and secured to the rigid backboard by a Primary Care Paramedic with eight years of emergency medicine experience.
The single-plane movements consisted of: head flexion, extension, side-flexion, and rotation, as well as atlanto-occipital (AO) flexion. Head/neck and AO flexion motions were differentiated using the cues “chin to chest” and “make a double chin,” respectively. For each motion, participants were instructed to perform a gradation of efforts, consisting of two repetitions each of low, moderate, high, and maximal exertions. Multi-plane movements (10-second duration) were chosen to mimic spontaneous, unscripted patient motion observed by EMS personnel in the field. These included: relieving an itch (intended to reflect low effort); using the hands to pull the cervical collar downwards and rolling the head to relieve discomfort (moderate effort); and a vigorous struggle against immobilization devices as in a combative or intoxicated patient (maximal effort). Two minutes rest was provided between each set of motions and five minutes rest was provided between immobilization conditions.
Accelerometers
Motion of the head/neck was quantified using a system of miniature, wireless, tri-axial accelerometers (range: ±10 g; resolution: 9 mg; mass: 0.047 kg; dimensions: 58×43×22 mm; Microstrain mXRS, Lord Sensing Systems; Williston, Vermont USA). The accelerometers were affixed to the anterior forehead (glabella) and superior sternum and aligned such that the x-, y-, and x-axes represented the anterior, lateral, and superior directions, respectively. The acceleration signals were sampled at 256 Hz and time-synchronized to ±32 μsec. Digital filters (zero-lag, 5th order Butterworth) were applied to isolate the low-frequency orientation changes (<0.5 Hz) and medium-frequency kinematics (0.5-4.5 Hz)Reference Wilcox, Beckwith and Greenwald 27 of the head and trunk segments from the higher-frequency tremor-related accelerations (>7 Hz). The resultant acceleration of the head was computed from the differences between the head and trunk accelerations across each axis. The peak and root mean square (RMS) accelerations were derived for the single- and multi-plane motions, respectively. Displacement was determined as the difference in pitch (orientation relative to YZ-plane, or flexion-extension) and roll (XZ orientation, or rotation) of the head and trunk, computed using trigonometric functions (atan2(y,x)). Data processing was performed using an open-source numerical computation program (GNU Octave, version 4.0, GNU Public License; FSF, Boston, Massachusetts USA).
Video
Video of each movement was recorded from two digital video cameras (30 fps, Casio Exilim, EX-FH100, Casio Computer Co, LTD.; Tokyo, Japan) positioned orthogonal to the sagittal (lateral view) and transverse (superior view) planes of each participant. Video-based angular displacements were derived from the angle subtended by three visible landmarks for AO flexion (lateral view: accelerometer – external meatus of ear – acromioclavicular joint), flexion and extension (lateral view: accelerometer – acromioclavicular joint – trunk midline), and rotation (top view: accelerometer – centre of head – accelerometer). Linear displacement of the head (mm) also was computed using a reference scale aligned with the plane of each motion.
Participant Characteristics
Neck length (cm) and girth (cm) were measured with a flexible tape as the distance from the strenoclavicular joint to angle of the mandible and circumference of the neck at the widest point, respectively. Neck strength was determined as the maximal isometric contractions (three seconds) against a handheld force transducer in the flexion, extension, and lateral flexion directions. The perpendicular distance from the line of action of the transducer to the C7 joint was recorded for computation of torque (Nm).
Statistical Analysis
The effects of effort and immobilization condition on head acceleration (peak, RMS) and displacement were evaluated using repeated measures ANOVA, with post hoc comparisons carried out for significant main effects. The relationship between accelerometer-derived measures (peak, orientation) and video-based measures (orientation) were determined using Pearson correlation. Statistical tests were carried out using SPSS19 (IBM Corp.; Armonk, New York USA) with P<.05 indicating statistical significance.
Results
Acceleration
As expected, head acceleration differed across the gradation of efforts (F(3,36)=26.08; P<.001; ηp 2=.69) with a mean (SD) of 62.7% (SD=6.7%) stepwise increase. Post hoc comparisons between efforts were significant for each motion (Figure 1; 1-4 above bars), with the exception of the high and maximal efforts for AO flexion (collar, board) and neck flexion (board), where the anticipated increase was not present or of lower magnitude (P>.08). Application of SI appliances reduced acceleration magnitude (F (2,24)=47.4; P<.001; ηp 2=.80), with attenuations of 23.5% (SD=4.8%) attributable to collar application (relative to unrestrained) and 44.6% (SD=5.4%) attributable to full SI (relative to collar). Post hoc comparisons across SI conditions were significant for each motion (Figure 1; 1-4 below bars), with the exception of collar application on maximal effort extensions (P>.10) and moderate through maximal effort side flexions (P>.11). Absolute acceleration magnitudes were similar for AO flexion, extension, and side flexion motions (P>.16) during both the collar-only (low: 0.77(0.13); medium: 1.24(0.23); high: 1.79(0.36); and max: 2.69(0.40) m/s2) and full-SI conditions (low: 0.49(0.10); medium: 0.74(0.18); high: 1.09(0.30); and max: 1.62(0.30) m/s2). Accelerations during neck flexion and rotation motions were 30.2% (SD=2.5%) greater (P<.05), at 1.23 (SD=0.21), 1.94 (SD=0.36), 3.34 (SD=0.74), and 5.12 (SD=0.76) m/s2 across the collar efforts, and 0.58 (SD=0.18), 0.89 (SD=0.25), 1.42 (SD=0.46), and 2.03 (SD=0.48) m/s2 across the board efforts (low through maximum efforts, respectively).
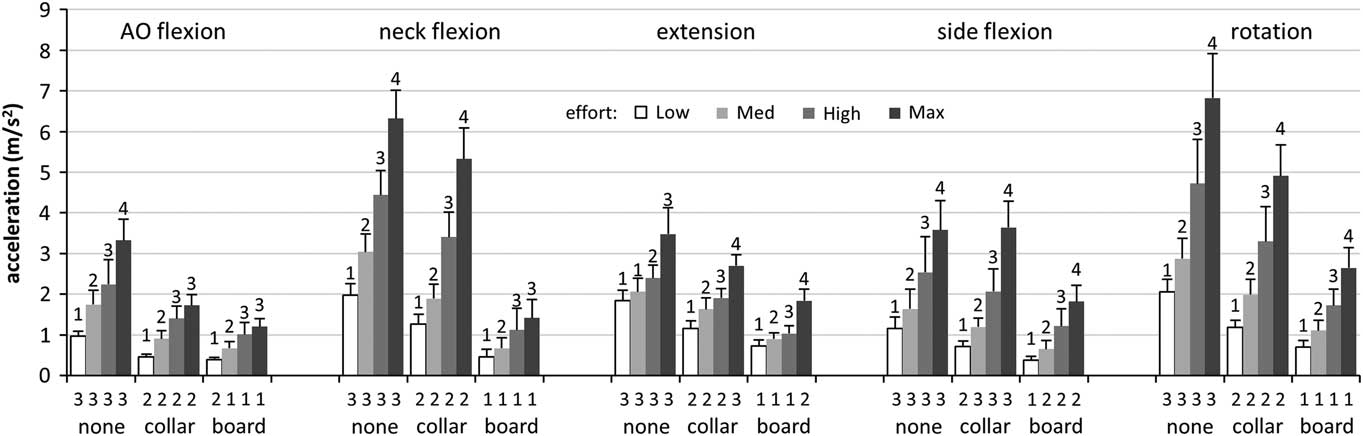
Figure 1 Acceleration (peak, M+SD) of the Head during Low, Medium, High, and Maximal Effort Voluntary Motions and across Unrestrained (none), Collar, and Full SI (boarded) Conditions. Post hoc comparisons are indicated by homogenous subsets (1-4), with the effect of effort (within-set) shown above the bars and the effect of immobilization (between-set) shown below. Abbreviations: AO, atlanto-occipital; SI, spinal immobilization.
Displacement
Similar large effects were apparent for effort (F(3,36)=88.8; P<.001; ηp 2=.88) and SI appliances (F(2,24)=73.5; P<.001; ηp 2=.86) on displacements derived from the accelerometers (Figure 2). Gradations of efforts were associated with significant increases in displacement across all conditions (38.6% (SD=9.0%) stepwise; P<.01), with the exception of neck flexion in full SI, where no change in displacement was detected across any of the effort levels (P>.17), and for AO flexion, where the effect was not as robust. Application of SI appliances resulted in a substantial decrease in displacement across all conditions (P<.01), with the exception of boarding on AO flexion (P>.30). Application of a collar was associated with a 36.1% (SD=8.0%) decrease in displacement (relative to no SI), and full SI a further 40.0% (SD=4.0%) decrease (relative to collar). Side flexion orientation/displacement could not be derived as there was no change in sensor orientation relative to the gravity vector when those motions were performed supine.
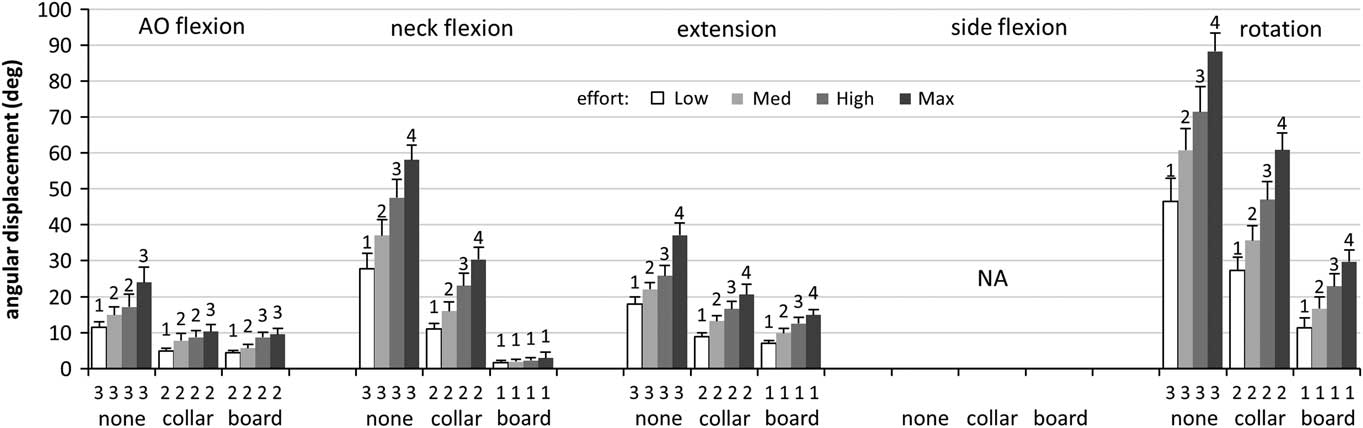
Figure 2 Displacement (peak, M+SD) of the Head Derived from Wireless, Triaxial Accelerometers during Low, Medium, High, and Maximal Effort Voluntary Motions and across Unrestrained, Collar, and Full SI (boarded) Conditions. Post hoc comparisons are indicated by homogenous subsets (1-4), with the effect of effort (within-set) shown above the bars and the effect of immobilization (between-set) shown below. Abbreviations: AO, atlanto-occipital; SI, spinal immobilization.
Relationship to Video-based Measures
Accelerometer-based displacements were related strongly to displacements derived from video (r=.83(.07), all motions), with comparatively low absolute differences across conditions (2.7° (SD=0.7°); Table 2). While absolute differences were comparatively low, relative differences for AO flexion and extension were larger (P<.05), due in part to smaller absolute displacements (16.8° (SD=0.8°)) compared to flexion and rotation (31.0° (SD=1.6°)). Acceleration magnitude was also predictive of video-based displacements, albeit with a slightly weaker relationship (r=.67(.06); range=.53 to .77; not shown). For side flexion motions, where no angular measures were obtained, the linear displacements derived from video were found to be related strongly to acceleration magnitude (r=.73(.03); P<.05; not shown).
Table 2 Relationship (Pearson r) and Difference (absolute, relative) of Angular Displacements Derived from Video- and Accelerometer-based Methods (M, SD shown). Positive differences indicate greater values for video-based estimates.

Abbreviation: AO, atlanto-occipital.
aP<.05.
Participant Characteristics
Kinematics (acceleration magnitude and displacement) were not related to participant anthropometrics (all r<.36; P>.22) or strength (all r<.33; P>.27).
Multi-dimensional Motions
The effects of effort (F(2,24)=33.4; P<.001; ηp 2=.74) and immobilization condition (F(2,24)=33.4; P<.001; ηp 2=.87) were apparent during multi-dimensional motions for both acceleration magnitude (Figure 3 a) and displacement (Figure 3 b). The stepwise increase in acceleration RMS across efforts was 70.2% (SD=10.7%), and the relative attenuation in acceleration associated with immobilization (38.7% (SD=3.1%)) was similar for both collar and full SI (P>.28). The average (RMS) accelerations during the multi-dimensional motions (Figure 3 a) were 89.5% ((SD=19.0%); (collar, P<.05)) and 109.3% ((SD=22.0%); (full SI, P>.17)) of the peak values observed during single-plane motions; however, acceleration magnitudes varied widely during individual multi-dimensional motions (Figure 4). The peak accelerations were 241.1% (SD=56.1%) and 176.5% (SD=40.7%) greater than those observed during the single-plane motions (P<.001). Therefore, the RMS was 47.4% (SD=4.4%) of peak values. The median frequency of the head accelerations during the maximal motions (2.6 (0.1) Hz) was slightly greater (P<.05) than both the itch (2.4 (0.1) Hz) and hands motions (2.2 (0.1) Hz), which did not differ (P>.22).
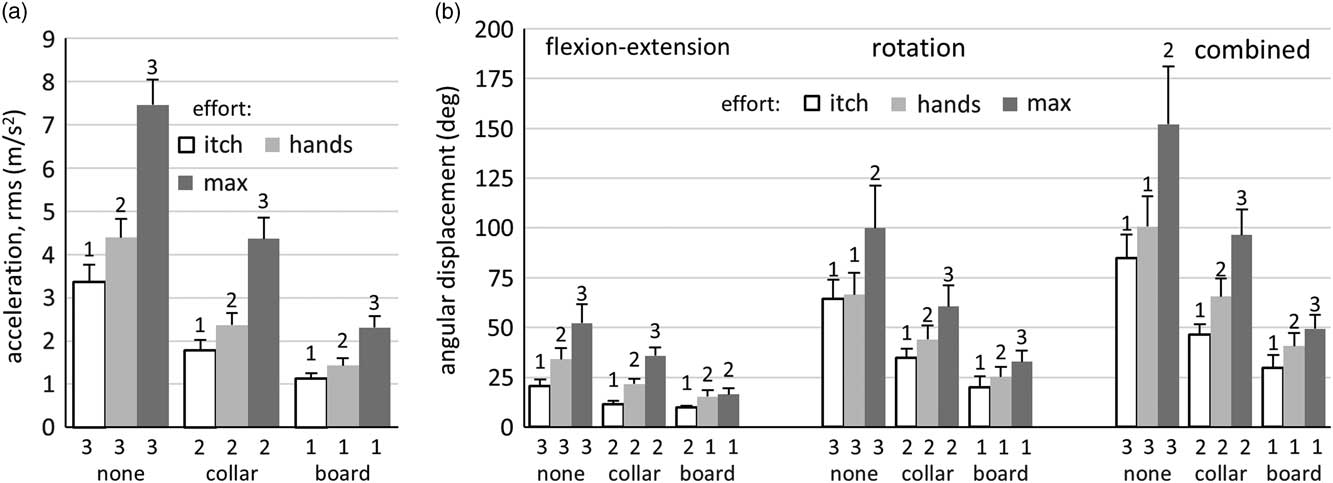
Figure 3 a) Accelerations (RMS, M+SD) and b) Angular Displacement (M+SD) of the Head during Abstract Motions across Unrestrained (none), Collar, and Full Immobilization (board). Motions included an imagined itch around head/neck area (“itch”); using the hands to pull collar away from mandible and moving the head (“hands”); and maximal struggle (“max”). Post hoc comparisons are indicated by homogenous subsets (1-3), with the effect of effort (within-set) shown above the bars and the effect of immobilization (between-set) shown below. Abbreviation: RMS, root mean square.
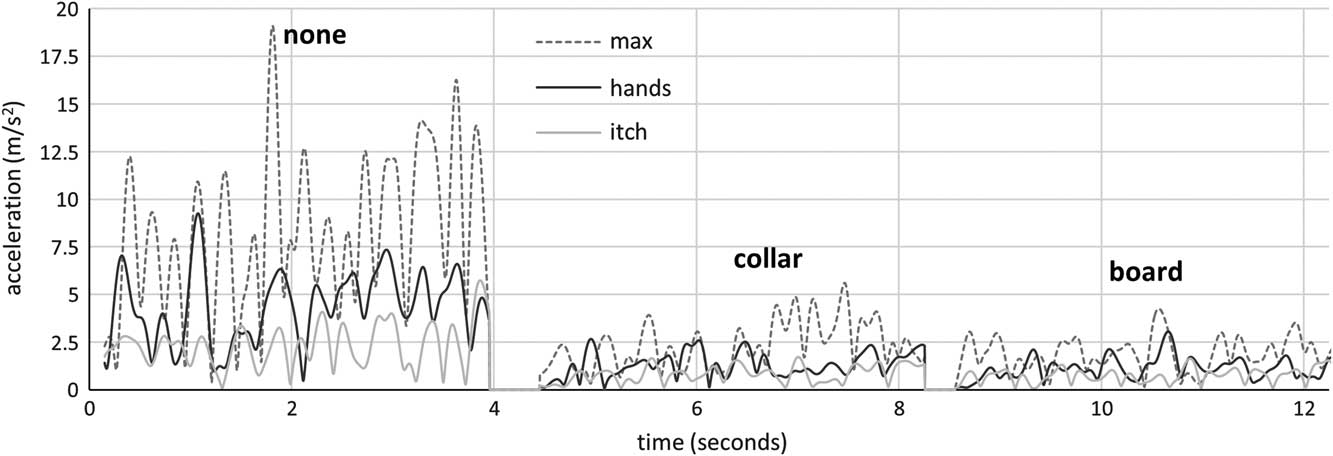
Figure 4 Representative Sample of Head Acceleration (resultant, relative to trunk) during Abstract Movements across Three Immobilization Conditions. Movements consisted of low effort motions to relieve an imagined itch around the head/neck area (“itch”); a moderate effort motion using the hands to pull collar away from mandible and moving the head (“hands”); and a maximal struggle (“max”). Four seconds of each condition are shown.
Discussion
This study provides preliminary estimates for head acceleration during a variety of SI conditions and adds to the small number of studies examining SI kinematics during circumstances similar to those encountered in practice.Reference Sarig-Bahat, Weiss and Laufer 14 - Reference Perry, McLellan, McIlroy, Maki, Schwartz and Fernie 20 With respect to motion in single planes, application of SI appliances resulted in a consistent stepwise reduction in acceleration magnitude (23% and 44% for collar and full SI, respectively). This finding is consistent with effects of SI on displacement found here (36% and 40%, respectively) and published previously (40% to >75%),Reference Webber and Kriellaars 28 - Reference Holla 31 but of a slightly lower magnitude. In spite of the reductions, participants were still able to produce substantial voluntary accelerations of the head (1.5 to 6.8 m/s2), indicating SI appliances likely attenuate displacement to a greater extent than acceleration. Further, the voluntary accelerations reported here are substantially larger than involuntary accelerations (described as “sudden jarring”) reported elsewhere (0.5 to 1.7 m/s2), which were of sufficient magnitude to displace unrestrained participants.Reference Treme, Diduch, Hart, Romness, Kwon and Hart 19 Given the potential role of force in contributing to secondary traumatic spine injury,Reference Boissy, Shrier and Briere 21 the data gathered here constitute a methodological starting point in accurately characterizing patient movements that potentially contribute to further harm.
Although the effect of effort on SI motion is hypothesized as a source of unaccounted variation across studies, 10 , Reference Voss, Page and Benger 11 it has not been investigated thoroughly. In the current study, increasing participant effort was associated with relatively consistent stepwise increases in acceleration (69%) and orientation (32%). The results demonstrate that the restraint imposed by SI appliances varies with effort and had no apparent plateau in restriction. While it is difficult to compare these results to previous studies that did not account for effort, these findings provide an estimate for the unaccounted variance if effort is not controlled: participants were able to elicit a further 30%-60% more motion when prompted for maximum, rather than high, efforts. This is similar to previous findings of increased motion when participants were provided visual stimuli rather than instructions to move as far as possible.Reference Manix 13
Across conditions, increasing effort had a greater effect on acceleration than on displacement in single-plane motions (increases of 69% and 32%, respectively). This effect was most evident during flexion in full SI, where increasing efforts were associated with a gradation of increasing accelerations, but not displacement. Similar effects also were apparent during multi-dimensional motions, where no change was detected in flexion-extension displacements at moderate and maximal efforts, in spite of increased acceleration. This provides further evidence supporting acceleration as a complementary outcome to orientation changes and indicates that acceleration magnitude may be more sensitive than displacement to changes in underlying head or neck motion. Further, although the correlation between acceleration and displacement was relatively high (r=.67), a substantial amount of variation remained unaccounted (55%; or r2 ~.45). One explanation for discordant acceleration and displacement changes may include translation-type motions (as when a participant’s head pokes forward) where the relative inclination of the head and torso does not change. This motion would manifest as detectable linear accelerations with no detectable change in angular orientation of body segments. Additionally, acceleration and displacement can vary somewhat independently, as high accelerations can occur in spite of small displacements, and vice versa. These results show that investigating participant effort during active motion complements measures of acceleration and displacement to characterize motion that might otherwise go undetected.
Whereas many studies have measured individual movements in a single plane, the generalizability of these findings to actual trauma patients is unclear. The three continuous, multi-dimensional motions studied here provide an indication of kinematics of realistic, voluntary patient motions (identified as “itch,” “hands,” and “maximal,” and described in Figure 4), which yielded distinct gradations of effort drawn from field observation. In spite of the use of full SI, participants were able to elicit substantive motions (up to 1.4 m/s2 and 40°) during low and moderate effort conditions, and even more so during the maximal effort, multi-dimensional motions (up to 2.3 m/s2 and 50°). These displacements exceed the displacements of 7° observed by Perry et al, caused by passive jarring and thought likely to compromise the quality of immobilization.Reference Treme, Diduch, Hart, Romness, Kwon and Hart 19 They are also equivalent to the peak displacements observed by Boissy et al in simulated agitated patients receiving manual stabilization, where the suitability of certain stabilization approaches was questioned.Reference Perry, McLellan, McIlroy, Maki, Schwartz and Fernie 20 Additionally, the peak values – as opposed to the RMS average – encountered during multi-dimensional motions were two to three times greater than those observed during single-plane motions.
The results of this component of the study indicate that participants moving continuously in multiple planes are able to move farther and generate greater accelerations than those moving only in a single plane in a given immobilization condition and at comparable effort. In this light, estimates of efficacy of SI appliances in single-plane motions may represent ideal performance that may not be generalizable to field conditions. Further, during maximal struggles against SI devices, restrained, non-compliant patients are capable of producing potentially harmful forces (accelerations) despite relatively little observed motion. This possibility warrants further investigation.
The displacements derived from accelerometers were related strongly to video-based measures (r=.83) and with relatively low error (2.7°), consistent with good concurrent validity. The relative reductions in displacement due to SI appliances (36% and 40% for collar and full SI, respectively) are consistent with previously reported values (40% to ~75%),Reference Webber and Kriellaars 28 - Reference Holla 31 albeit at the lower end of the range. Previous investigations have noted that IMUs can provide near perfect resolution of orientation; however, this generally has been established under ideal conditions (that is, with negligible external acceleration) and/or using IMUs that house additional sensors (for example, magnetometers and gyroscopes).Reference Perry, McLellan, McIlroy, Maki, Schwartz and Fernie 20 , Reference Sandler, Dvorak, Humke, Grob and Daniels 32 , Reference Shrier, Boissy and Briere 33 The variations (error) reported here are slightly larger than those reported previously,Reference Sandler, Dvorak, Humke, Grob and Daniels 32 but they may be more indicative of the variation encountered during actual human movements, and they also provide a potential alternate method of quantifying orientation in SI.
The results of the current study suggest a number of findings to be investigated in future research. First, acceleration offers a complement to displacement in characterizing patient motion. Second, participant effort has an effect on outcomes when studying active motion. Third, realistic and clinically relevant scenarios yield results that differ from ideal or laboratory-based experiments. Once refined, techniques such as those used in this study may be suitable for deployment on actual patients in trauma settings.
Limitations
The current study shares a number of limitations with other studies examining SI conditions. The amount of motion that causes additional traumatic injury remains unknown. Previous studies have assumed that any motion is potentially harmful.Reference Treme, Diduch, Hart, Romness, Kwon and Hart 19 , Reference Sandler, Dvorak, Humke, Grob and Daniels 32 , Reference Lebel, Boissy, Hamel and Duval 34 It remains an open question as to whether perfect immobilization is achievable under field conditions or uniformly beneficial to all patients. 4 - Reference Connor, Greaves, Porter and Bloch 6 Additionally, measurements of body-segment motion will only approximate intervertebral motion. The exact relation between observed motion and movement of the spinal column, much less disruption of the spinal canal in cases of unstable injury, is unknown.
Conclusion
The results of this study support the use of accelerometer-based IMUs for quantification of head motion during SI. Both displacement and acceleration were shown to vary as expected across a range of efforts and immobilization conditions, and acceleration was shown to complement orientation in characterizing patient movement. The effects of effort and multi-dimensional motions add to the small number of studies describing the kinematics of patient motion in realistic situations.Reference Sarig-Bahat, Weiss and Laufer 14 - Reference Perry, McLellan, McIlroy, Maki, Schwartz and Fernie 20 Inertial measurement sensors are well suited to investigating patient motion and immobilization techniques in realistic, clinically relevant ways and are not restricted by limitations of traditional laboratory-based methods. Future research should consider study designs that mimic or use actual trauma settings.






