Introduction
Airway management (AM) is an important part of prehospital care provided by ambulance staff.Reference Ismail, Zia, Samad, Naeem, Ahmad, Raza, Baqir and Khan 1 Airway management is generally more challenging in prehospital settings compared to hospital settings, but unfortunately in low- and middle-income countries (LMICs), training required for ambulance paramedics in airway skills does not match that required for hospital-based practitioners such as anaesthetists and emergency physicians.Reference Jacobs and Grabinsky 2 - Reference Sanson, Di Bartolomeo and Nardi 5 As a result, those making decisions at the critical moment on the site of emergency are seldom aware of the factors which one should keep in mind when taking affected persons to a hospital. As a result, many victims die a preventable death at the scene or during the first few hours following emergency conditions (including injury and trauma).Reference Winchell and Hoyt 6 , Reference Baqir and Ejaz 7
The importance of AM training of ambulance staff and availability of equipment in the ambulances has been recognized in developed countries.Reference Razzak, Baqir and Khan 8 Unfortunately, the capacity to provide the basic level of prehospital care does not exist in many LMICs, including Pakistan.Reference Winchell and Hoyt 6 Poorly trained ambulance staff with ill-equipped ambulances are frequently observed problems in LMICs.Reference Deakin, King and Thompson 9 There are a number of ambulance services in the city of Karachi, Pakistan, which either belong to individual hospitals or private non-profit organizations. A survey done in 2009 in Karachi showed that ambulance drivers from two privately run charity-based ambulance services had no paramedic training, and ambulances were equipped only with a stretcher and an oxygen cylinder with no resuscitation measures available.Reference Bhatti, Waseem and Razzak 10
The World Health Assembly (Geneva, Switzerland) has reiterated its call for reforming the available prehospital care services worldwide.Reference Siddiqui, Jawad and Minhas 11 Unfortunately, there is almost no recent literature from LMICs, including Pakistan, detailing availability of AM equipment in ambulances and the amount of AM training undertaken by ambulance technicians and paramedics for a quality prehospital care system.
The objectives of this study were to: (1) assess the awareness of ambulance staff regarding the concept of AM; (2) assess the knowledge of those ambulance staff who are aware of this concept; (3) assess the level of training of ambulance staff pertaining to AM; and to (4) assess the availability of AM equipment in ambulances of Karachi.
Methods
This cross-sectional study was conducted in Karachi, Pakistan from June through September 2014 after approval from Ethical Review Committee of the Aga Khan University (Karachi, Pakistan). For this study, six major ambulance services operating in Karachi were approached, out of which, five consented to be a part of the study. For the purpose of confidentiality, the ambulance services have been named as Ambulance Services A, B, C, D, E, and F. The operation of these ambulance services is not centralized as each ambulance service is contacted by a separate phone number. The data were collected at two levels: (1) the management of the ambulance services, and (2) the ambulance staff, which included ambulance drivers, paramedical staff, and ambulance doctors. Data collection was done by data collectors specifically hired and trained for this study. Two separate consent forms and tools were developed: one for the organizational level data and the other for ambulance staff-related data. Both the tools and consent forms were available in English and Urdu.
Ambulance Services
For the data collection from ambulance services, management of each service was approached by one of the investigators and the purpose of the study was explained to them. After taking informed consent, interviews were conducted with the identified management individuals. Data related to number of vehicles operating under the ambulance service, total number of ambulance staff working, the number of staff in each ambulance sent to attend emergency calls, whether AM training is provided to the ambulance staff, the level of training of ambulance staff, and availability of AM equipment in ambulances were collected.
Ambulance Staff
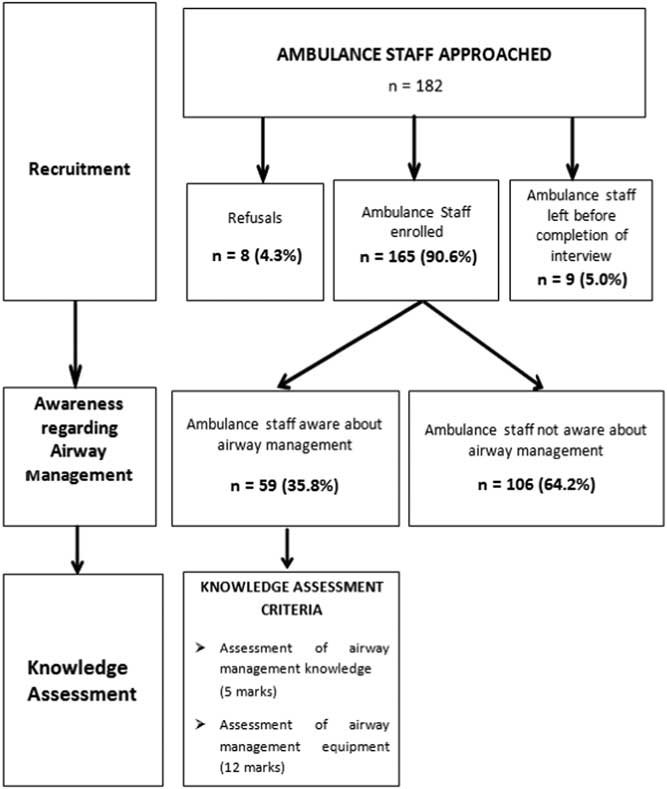
The ambulance staff was recruited into the study either from their specific ambulance service centers in the city or from the emergency departments of three major tertiary-care hospitals of Karachi. After taking informed consent, face-to-face interviews were done using a predesigned questionnaire. Figure 1 gives a flow diagram of participant recruitment and knowledge assessment.
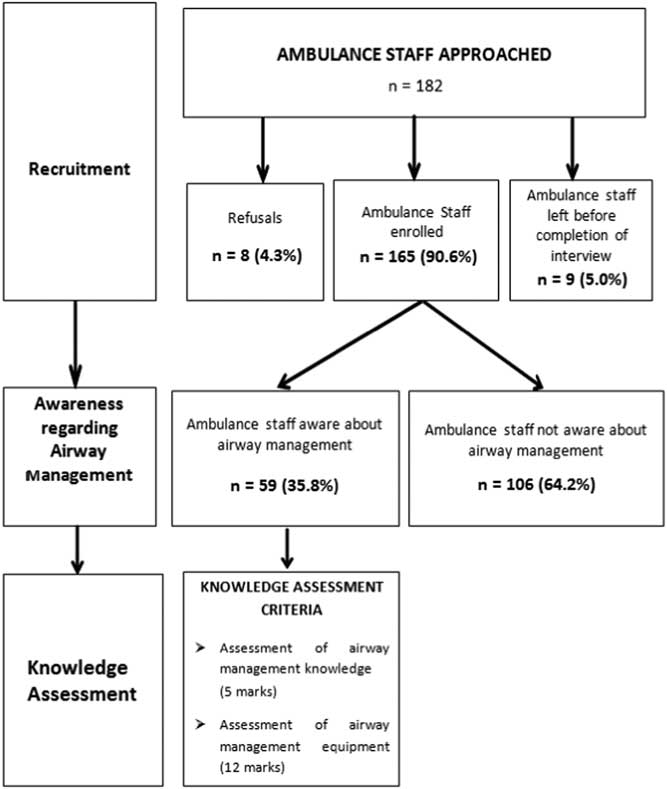
Figure 1 Ambulance Staff Awareness Regarding Airway Management and Knowledge Assessment.
The first component of the questionnaire was related to demographics, including age, gender, level of education, designation in the ambulance service, years of experience working in ambulances, and AM training. The next section of the questionnaire assessed the awareness of the ambulance staff about the concept of “airway management.” All the ambulance staff were asked if they had heard, seen, or practiced AM on patients. If the answer was “No,” they were asked about their usual practice of transferring the patients (either with or without oxygen). If the answer was “Yes,” they were assessed for their knowledge in managing patients’ airways.
The knowledge was assessed in two parts: the first part was related to knowledge of assessing the need for AM, neck stabilization, and steps required for AM, and the second part dealt with knowledge related to equipment required for AM. This was a self-reporting assessment. A scoring system was developed for quantifying the knowledge of ambulance staff; a total score of 17 points could be obtained (five for the first part and 12 for the second part). When enumerating the steps required for AM, each correct step mentioned by the respondent was given one point. Regarding knowledge pertaining to AM equipment, one point was given for each correct mention of equipment required for AM. Table 1 shows the questions asked to gauge knowledge regarding steps for AM in emergency patients and names of equipment required for AM.
Table 1 Questions Related to Assessment of Knowledge of Steps and Equipment Required in Airway Management

Sample Size
Based on available estimates, there are approximately 500 ambulances in the city of Karachi with one to two staff members per ambulance. Previous data on the ambulance services in Karachi had indicated ambulances as being merely transport vehicles with untrained staff. No quantitative data regarding AM knowledge were available. Therefore, the minimum sample size for this survey was calculated with only an anticipated prevalence of knowledge of AM amongst ambulance staff.Reference Winchell and Hoyt 6 , Reference Anderson, Suter and Mulligan 12 , Reference Chandran, Ejaz and Karani 13 It was expected that over 90% of ambulance staff would not have knowledge related to AM, so the prevalence of knowledge was estimated with 95% confidence interval, giving a minimum sample size of 137 ambulances staff for this study. This sample size of 137 was distributed proportionately according to the number of ambulances that each of the six major service providers have in Karachi. A total of 165 ambulance staff were interviewed using the tool developed for ambulance staff.
Data Analysis
The data were entered and analyzed using Statistical Packages for Social Sciences version 19 (SPSS Inc.; Chicago, Illinois USA). Percentages and frequencies were reported for categorical variables and mean with standard deviation for continuous variables. For this analysis, the Ambulance Service A was taken as standard and was compared with other services based on organizational data, demographic characteristics, and knowledge assessment. Type of training and awareness of AM equipment were reported as multiple responses. Chi-square and Fisher’s exact tests were applied to compare qualitative variables between Service A and other ambulances services, while t-test and Mann Whitney U test were used to compare quantitative variables between Service A and other ambulance services. A P value of <.05 was considered as significant.
Results
Ambulance Services
Out of six ambulance service providers approached, five agreed to participate in the study. Overall, a total of 615 ambulances and 1,336 ambulance staff had been reported by the five ambulance service providers. The number of vehicles owned by each organization was variable, ranging from a maximum of 300 to a minimum of 10 vehicles per organization.
Regarding the training of ambulance staff, only two ambulance services (A and B) claimed to provide life support and AM training to their staff. According to the organization heads of Ambulance Service B, 70% (n=350/500) of their staff had received Basic Life Support (BLS) and AM training. According to the organization heads of Ambulance Service A, 91% (n=500/550) of their staff had received BLS and AM training. In addition, 13.6% (n=75/550) of ambulance staff of Ambulance Service A had training in Advanced Cardiac Life Support.
Regarding the number of ambulance staff sent to attend an emergency call, all the providers sent an ambulance with a solo driver, while Service A also reported to have paramedical staff and technicians in their ambulances. When sent for an emergency call, the reported ratio of ambulance vehicle to ambulance staff was 1:1 for all ambulance services except for Service A, where the ratio was either 1:2 or 1:3. On average, each ambulance service provider attended more than five calls a day.
When inquired about the availability of AM equipment in the ambulances, all the ambulance service providers had basic equipment for AM, which included oxygen cylinder/face mask, Ambu bag, and oral and nasal airway. Only Service A had advanced AM equipment and medications which included endotracheal tube, laryngoscope, suction machine, and medication for intubation, in addition to basic equipment like oxygen cylinder with Ambu bag/face mask and oropharyngeal and nasopharyngeal airway.
Ambulance Staff Demographics
Most of the ambulance services provided basic transportation vehicles except for one, Ambulance Service A, which had ambulances that were better equipped with AM equipment and trained staff to provide prehospital care to the patients. Therefore, Ambulance Service A was taken as a standard ambulance service provider in terms of ambulance staff and equipment for the purpose of comparison of ambulance services. Table 2 gives the total and comparison of demographic characteristics of staff belonging to Ambulance Service A with other ambulance services. The comparison showed that most of the other ambulance services only had drivers (n=115/117; 98.3%) while ambulances of Service A had paramedical staff (n=22/48; 45.8%) and doctors (n=2/48; 4.2%) in addition to drivers (n=21/48; 43.8%). The mean age of ambulance staff of Service A was significantly lower than that of other ambulance services (31.3 years (SD=5.4 years) compared to 38.3 years (SD=10.0 years); P value <.01); however, the years of experience of the ambulance staff from other ambulance service was significantly higher than from Ambulance Service A staff (63.2% vs 20.8% with more than five years of experience; P value <.01). Approximately 13% of the ambulance staff from Service A reported attending ≥ five calls per day compared to 35% staff from other ambulance services (P value <.008; Table 2).
Table 2 Comparison of Demographics and Number of Emergency Calls Attended by Staff of Various Ambulance Services (n=number of ambulance staff)

Awareness of the Ambulance Staff Regarding Concept of Airway Management
Of the 165 ambulance staff, the majority (n=106; 64.2%) had never heard the term “airway management” and had no concept of assessing the need to manage the airway of a critical patient in an emergency situation. Out of these 106 staff, 88.7% (n=94) transported patients in ambulances with oxygen in case patients had shortness of breath or had difficulty in breathing.
Training and Experience of Ambulance Staff who had Awareness of Airway Management
Out of one-third (n=59; 35.8%) of ambulance staff who had heard, seen, or practiced “airway management,” 86.4% (n=51) were trained in BLS and 30.5% (n=18) received training in Advanced Life Support. Approximately 81.4% (n=48/59) received formal training in AM. Approximately 88.1% (n=52) had experience performing bag mask ventilation, 84.7% (n=50) had experience using oropharyngeal or nasopharyngeal airway, 37.3% had experience with laryngeal mask airway, and 45.8% had experience performing endotracheal intubations (Table 3).
Table 3 Comparison of Training and Experience of “Airway Management” of Staff of Ambulance Service A and Other Ambulance Services Staff (n=59)

Abbreviations: ALS, Advance Life Support; BLS, Basic Life Support; LMA, laryngeal mask airway.
a Multiple response variables, therefore the percentage does not add up to 100%.
b Others: first aid training; Advance Trauma Life Support; Pediatric Advance Life Support; Prehospital Trauma Life Support; Emergency First Response; Cardiac First Responder.
Airway Management Assessment
Fifty-nine ambulance staff who reported awareness regarding AM were assessed for their actual knowledge regarding management of airway. The mean score was 4.73 (SD=0.71) out of a total of five with a minimum score of two and a maximum score of five. The mean score for knowledge regarding AM equipment was 8.39 (SD=2.31) out of 12 with a minimum score of two and a maximum score of 12 (Table 4).
Table 4 Comparison of Assessment of Scores of Ambulance Staff A with Staff of Other Ambulance Services Regarding Management of Airway and Equipment Knowledge (n=59)

Discussion
This study gives an insight into the awareness, level of training, and knowledge of ambulance staff pertaining to AM of critical patients in Karachi, which is the largest and most populous metropolitan city of Pakistan. Karachi is considered the center of research in biomedicine with at least 30 public hospitals and more than 80 private hospitals.Reference Waseem, Carenzo, Razzak and Naseer 14 Therefore, being the economic engine of growth and facing tremendous growth in traffic at 7.2% annually, this city is representing the major share of ambulance services of Pakistan.Reference Waseem, Carenzo, Razzak and Naseer 14 This study has shown that the situation with regard to AM in ambulances of Karachi, and hence, Pakistan, remains grim as the majority (64.2%) of ambulance staff interviewed had never heard about AM and had no concept of how to assess and manage patients’ airways in critical situations at the site of injury or during transportation to hospitals. Of the one-third of ambulance staff (35.8%) who had heard about this concept, the majority (46/59; 77.9%) belonged to only one ambulance service which has been taken as the standard ambulance service in this study. Thus, the number of aware staff has very little representation from the remaining five ambulance services in the study sample. The ambulance staff who had heard about AM showed a thorough knowledge about this concept. The study therefore reveals extremes of both awareness and unawareness regarding AM.
The results of this study show insufficient knowledge of ambulance staff from Pakistan in providing even basic prehospital care to patients; this is consistent with previous studies.Reference Deakin, King and Thompson 9 , Reference Bhatti, Waseem and Razzak 10 , 15 However, in terms of the availability of AM equipment in ambulances, the findings of this study are different from what was stated in previous literature.Reference Winchell and Hoyt 6 , Reference Bhatti, Waseem and Razzak 10 The results of a survey done in 2009 showed that ambulance services in Karachi were only equipped with a stretcher and an oxygen cylinder with no other resuscitation equipment.Reference Bhatti, Waseem and Razzak 10 In addition, another study from Pakistan published in 2006 mentioned a lack of life-saving equipment, including oxygen cylinders in ambulances. 15 Contrary to expectations based on such earlier surveys, this study suggests that many of the ambulance services in Karachi do have basic equipment required for AM of patients during transfer to hospitals. It is possible to state that the availability of AM equipment has improved since earlier studies were conducted.
Despite this, the situation with regard to AM in ambulances remains grim in Karachi, as it seems that the problem does not lie in lack of availability of AM equipment but in the human resource. Among the ambulance staff interviewed, paramedics, technicians, and doctors belonged to only Ambulance Service A. The majority (82.5%) of the ambulance staff were drivers with 98.3% belonging to organizations other than Ambulance Service A. In addition, the ratio of ambulance to staff in all ambulance services was 1:1, except for Ambulance Service A where the ratio was 1:2 or 1:3. Therefore, according to the findings of this study, even in ambulances which do have basic AM equipment, there is only an ambulance driver on board. There is no paramedical staff available to carry out AM procedures on patients during transfer to hospital. These factors render the availability of AM tools ineffective in ambulances for the purposes of prehospital care and the ambulances can be justly termed as mere transport vehicles.
Another important point highlighted in this study was the lack of training of ambulance staff, as the majority of ambulance staff interviewed did not receive any training regarding AM. Although the management of one ambulance service claimed to provide training to 70% of its staff, interviews with ambulance staff revealed that only 7.8% of ambulance staff from ambulance services other than Ambulance Service A received AM training.
Among the ambulance staff who did not belong to Ambulance Service A and who were aware about AM, some (38.5%) had not received formal training about AM but had acquired the concepts through extensive experience in the field. As can be expected, this shows that staff can learn about AM through experience without formal training. However, such an approach is not efficient and relies heavily on the learning ability of ambulance staff from circumstances and the irregular opportunities in the field during the course of duty. This finding is somewhat consistent with a previous study which stated that ambulance staff had gained confidence through experience and had increasingly treated patients at the scene, which had therefore led to a decline in the actual number of transfers to hospitals. 15 However, this previous study also highlighted a need for formal emergency management trainings for ambulance staff to further boost their confidence and abilities to save lives. 15
The literature from the developed world has emphasized that one-time training of ambulance staff is not sufficient. It is crucial to have regular refresher courses, frequent practice, and regular feedback on performance regarding AM for ambulance staff to maintain their competence.Reference Ali, Miyoshi and Ushijima 16 It is proposed that simulation training for ambulance staff should be conducted, and procedures performed by ambulance staff should be registered systematically to help target supervision.Reference Ali, Miyoshi and Ushijima 16 In cases where awareness regarding AM equipment use is low, literature proposes check-outs, guidelines, standard operating procedures, and quality control measures to be in place.Reference Jacobs and Grabinsky 2 Health care professionals should take an initiative to arrange AM courses and liaison with the ambulance services to make it mandatory for their staff to attend these courses. After achieving a basic level of training, refresher courses can be done at regular intervals to maintain the skill and knowledge levels achieved. Regular audits can be performed to assess the quality of these courses.
Limitations
One of the limitations of this study was that the data obtained from the organization and ambulance staff were self-reported. The study therefore relied on the information provided to the investigators by the ambulance service management and staff. Another limitation of this study was that only the theoretical knowledge of ambulance staff was assessed, whereas how AM was being done in real-life situations was not looked into, which could have given deeper insights into the knowledge and performance of ambulance staff.
Conclusions
It was found that the majority of the ambulance services in Karachi are not lacking in AM equipment, but in manpower, as the ambulance staff hired by the organizations comprised mostly of drivers who were the only persons sent to attend emergency calls. As there was no provision of training of ambulance staff, the sole purpose served by these ambulances was merely the transportation of critical patients to hospitals. At the ambulance services level, there is a need to uplift the training status of ambulance staff and to increase the number of staff per ambulance to at least two to provide adequate care to patients during transportation to the hospital. A system of quality assurance in ambulatory care may be helpful in improving the AM situation in ambulances of Karachi. Since there is one ambulance service operating in the city of Karachi which is providing regular training pertaining to AM to their staff, it can be taken as a gold standard.
Acknowledgment
The authors acknowledge the data collection team and tertiary care centers which participated in the study.