Introduction
The increase in institutional delivery and the decline in maternal mortality are the key indicators to monitor the central goal of safe motherhood and child survival movements, as per the fifth Millennium Development Goal. Reference Kesterton, Cleland and Sloggett1 It is estimated that at least 15% of all pregnancies will encounter complications and seven percent will be serious enough to require referral to a higher level of care. 2 Most maternal deaths are preventable if pregnant women receive timely and quality emergency obstetrics services by skilled attendants. 2 The delay in deciding to seek care, delay in reaching an adequate health care facility, and delay in getting appropriate care at the institutions are three identified major delays that are responsible for home deliveries as well as maternal death. Reference Holmes and Kennedy3 To prevent home deliveries, as well as maternal death, it is important to address all three delays equally. However, strategies to address the second delay have been relatively neglected; the lack of transport, poor communication, high cost, and geographical barriers are also important causes of fatal delays in reaching life-saving care. Reference Holmes and Kennedy3 One-third of reported maternal deaths occurred at home or on the way to care, which can be reduced by providing pregnant women with timely and free transportation. Reference Ganatra, Coyaji and Rao4–Reference Thaddeus and Maine8 In the last decade, the Government of India has taken several initiatives to improve the availability of basic transport and ambulances for pregnant women, including a decentralized “108” Emergency Medical Response Services (EMRS) maintained through public-private partnerships. 9–11 Although they provide free-of-cost services to all patients who are critically ill, as well as victims of trauma and accidents. There is no doubt that the indicators of maternal health and child health can improve by providing quality EMRS. Reference Singh, Murthy and Thippaiah6,Reference Prinja, Bahuguna and Lakshmi12–Reference Raj, Manthri and Sahoo14 But evaluation of the existing EMRS in a timely manner and incorporating innovations go hand-in-hand, two continuous processes required to enhance the performance of the services. Therefore, the aim of this research is to contribute to the knowledge about the use of the EMRS for pregnant women in the tribal district of Western India.
Material and Methods
Study Location
The District of Dadra and Nagar Haveli (D and NH) is situated on the western coast of India between the states of Gujarat and Maharashtra. It lies between north latitudes 20° 02’ and 20° 22’ and east longitudes 72° 54’ and 73° 14’. The headquarters of the district is located at Silvassa. The EMRS was launched on April 10, 2012 under a public-private partnership with public financing and private delivery. The call center of the private provider was established in Shri Vinoba Bhave Civil Hospital, Silvassa. The EMRS works through a 24×7×365 centralized Emergency Medical Response Center (EMRC). The EMRS is dedicated to providing out-of-hospital acute medical care and/or transport to definitive care to patients with illnesses and injuries. The services could be accessed to the place of emergency by dialing a toll-free number “108” throughout the Union Territory (UT). The nearest ambulance available to the site is dispatched by the EMRC by using a well-functioning Geographic Information System.
Study Design
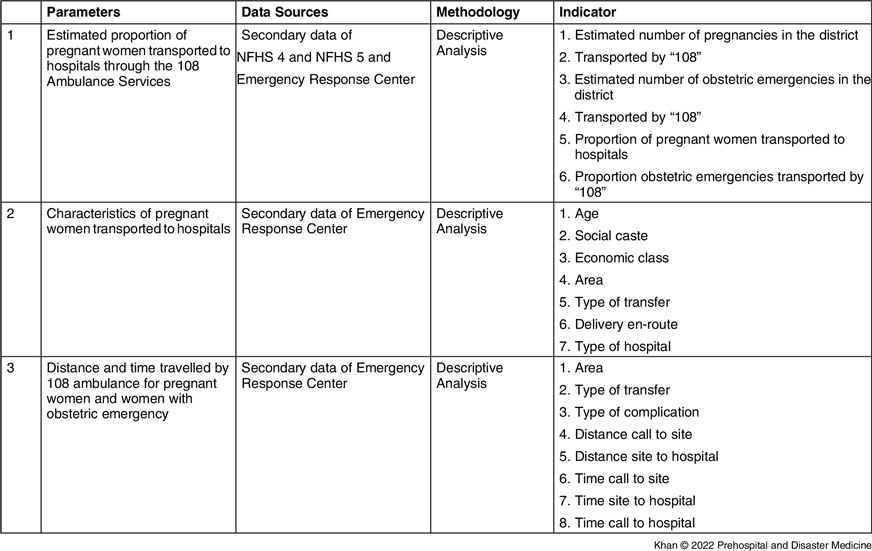
This study is a descriptive analysis of the EMRS from January 1, 2013 through December 31, 2020. The secondary data of emergencies related to pregnancy, social-demographic variables, and matrixes of services were drawn from the EMRS tracking software which is generated from the calls received at the centralized call center for availing EMRS. The obstetric emergency, for this study, is defined as any life-threatening medical complication related to pregnancy or medical complication during pregnancy, labor, or child-birth, or within 42 days of termination of pregnancy. A pregnancy-related call is defined as any call from, or for, a pregnant woman in labor or in the post-partum period for post-natal care, abortion-related care, labor pains, child-birth, or any complication during these periods. The demographic data of the population were collected from the data of Census 2011. The information related to institutional delivery and estimated numbers of obstetric emergencies were obtained from the State Data Center, as well as the National Family Health Survey (NFHS)-4 and NFHS-5. The number of pregnant women transported by “108” as recorded in the call center were compared with these estimated numbers. The details of the methodology are given in Table 1.
Table 1. Overview of the Methodology

Abbreviation: NFHS, National Family Health Survey.
Ethics Approval and Consent to Participate
The authors of this manuscript declare that this scientific work complies with reporting quality, formatting, and reproducibility guidelines set forth by the EQUATOR Network. The authors also attest that this clinical investigation was determined to require the Institutional Review Board/Ethics Committee review, and the corresponding protocol/approval number is DMHS/IEC/2016/214/2018.
Results
Frequency of Calls Related to Pregnancy Landed at EMRC
A total of 54,939 pregnancy-related calls were attended by the EMRC from January 1, 2013 through December 31, 2020. A higher proportion of calls were landed from rural/tribal area than urban areas. However, in the year 2015, 49.16% of the total population of the District of D and NH lived in rural areas. The proportion of the rural population increased year after year. In the year 2020, the contribution of the rural population to the total population was 68.01%, whereas 85.51% to 90.59% of total calls related to pregnancy were received by the “108” call center from rural areas. Overall, ambulances were provided for more than 99% of pregnant women in pregnancy-related calls.
Proportions of Pregnant Women and Obstetric Emergencies Handled by EMRC
Total 44,809 pregnant women were transferred to hospitals using “108” ambulances from the period of January 1, 2013 through December 31, 2020, which was 93.59% of the estimated pregnancies. The estimated proportion of pregnant women transported by “108” ranged from 68.53% in the year 2017 to 117.06% in the year 2019. A total of 6,106 obstetric emergencies were transported to the hospital from the period of January 1, 2013 through December 31, 2020, which was 85.02% of estimated obstetric emergencies. The highest proportion of obstetric emergencies transported was in the year 2019 (158.69% estimated obstetric emergencies) and the lowest proportion was transported in the year 2017 (30.68% of estimated obstetric emergencies), as shown in Table 2. Out of those pregnant women who took advantage of “108” emergency response services during the obstetric emergency, 88.7% were tribal living in rural places.
Table 2. Estimated Proportion of Pregnant Women Transported to Hospitals by 108 in the District of Dadra and Nagar Haveli

Abbreviation: EMRC, Emergency Medical Response Center.
Characteristics of Pregnant Women Handled by EMRC
Out of the pregnant women transported by the “108” service, 82.32% women were aged 20-35 years old, 16.51% women were aged <20 years, and 1.17% were aged >35 years old. A higher proportion of users belonged to scheduled tribes, followed by other backward caste, general caste, and scheduled caste. Out of the pregnant women using “108” facilities, 88.95% were women residing in tribal/rural areas. An average percentage of deliveries that happened at the pick-up site or in the ambulance en-route were noted 2.99% during the study period; it was highest (3.78%) in the year 2014 and lowest (2.15%) in the year 2018. More than 98% of pregnant women transported by the “108” service shifted to public hospitals (Table 3).
Table 3. Characteristics of Pregnant Women Transported to Hospitals by EMRS in the District Dadra and Nagar Haveli

Abbreviation: EMRS, Emergency Medical Response Services; DK, don’t know; BPL, below poverty line.
Distance and Time Travelled by 108 Ambulances for Pregnant Women
The ambulances travelled less than 10km to reach 89.0% of pregnant women, followed by 11-20km to reach 9.86% pregnant women, 21-30km to reach 1.05% pregnant women, and more than 30km to reach 0.08% pregnant women. To avail the definitive care, 69.56% of pregnant women covered a distance of up to 10km from the pick-up site to reach the hospital, while 23.81% covered a distance of 11-20km, 5.65% covered a distance of 21-30km, and less than one percent of covered a distance of more than 30km. The median distance from pick-up site to the health center was 8km. The average time taken in travel to reach the pregnant women was 11:10 minutes and the time taken in travel from site to hospital was 13:39 minutes (Table 4).
Table 4. Distance and Time Traveled by 108 Ambulances for Pregnant Woman

Discussion
It is well-documented that the lack of transport, poor communication, high cost, and geographical barriers are important causes of fatal delays in reaching life-saving care. Reference Holmes and Kennedy3 The availability of timely and free transport to pregnant women is a key intervention to reduce such delays. 7,Reference Thaddeus and Maine8 The data of the present investigation confirmed the statement of previous workers that the timely and hassle-free emergency response services to pregnant mothers can increase institutional delivery and reduce the risk of morbidity and mortality of the mothers and newborns. This is encouraging; as desired, more pregnant women were accepting “108” ambulance services. However, the results of a previous study conducted in Punjab indicate that EMRS did not have a significant impact on the increase in institutional deliveries. Reference Prinja, Bahuguna and Lakshmi12 The number of pregnant women transported by “108” in the District of D and NH increased from 6,161 (73.4% of estimated pregnant women) in 2015 to 8,782 (112.5% estimated pregnant women) in 2020; simultaneously, significant improvement was noted in the institutional deliveries, which were 88.0% in 2015 and 96.0% in 2020. The reason for providing the service availed to be more than 100% of the estimated pregnant women may be due to some pregnant women having used the services more than once during the period of pregnancy.
It is undeniable that tribal and rural pregnant women are more prone to home delivery and obstetric complications. Reference Hussein, Kanguru, Astin and Munjanja15–Reference Narzary, Kumar and Jadhav17 In the present investigation, most of this service was used by tribal pregnant women and pregnant women living in villages. By providing easy EMRS to these high-risk groups living in remote areas, institutional delivery has certainly increased and the risk of obstetric complications has been reduced. According to the World Health Organization (WHO; Geneva, Switzerland) and United Nations Population Fund (UNFPA; New York USA), laboring women have access to the institutional-based emergency obstetric and newborn care facilities within two hours. Longer times have been associated with worse outcomes, including higher maternal mortality. Various studies show that institutional-based emergency obstetric and newborn care facilities have been accessible to pregnant women in less time than the norms set by the WHO and UNFPA in various states of India. Reference Strehlow, Newberry and Bills18 To the best of the authors’ knowledge, and as per the available literature, the accessibility of the institutional-based emergency obstetric and newborn care facilities is being provided to the pregnant women of the District of D and NH in the shortest time in India. Previous work has pointed out that the 22% of the women have their first pregnancy before age 18 in India. Reference Moore, Singh and Ram19 But in this study, it has been found that only 16.51% of women get pregnant at the age of younger than 20 years; this is lower than the previous study. During the study period, emergency medical technician-assisted deliveries were noted (1,643; 2.99%), which was less in percentage than reported in previous studies. Reference Strehlow, Newberry and Bills18,Reference Mavalankar, Singh, Patel, Desai and Singh20 In the present investigation, the response time of ambulance was noted (11:10 minutes), which was the lowest in India. Reference Prinja, Bahuguna and Lakshmi12
Limitations
The secondary data were drawn from the software which was generated from the telephonic calls received at the centralized call-center for availing EMRS. The complications in pregnancy mentioned in the software were broadly described and not specific. Hence, it was difficult to analyze the complications. Furthermore, the epidemiological data suggested the pattern of emergencies handled by EMRS only, and not the actual emergency data, as non-EMRS user data were not available.
Conclusion
The current study involved a unique analysis. There is no exception in the fact that home delivery is a cause of the adverse impact on maternal and infant health, and lack of transport facilities is one of the main reasons for home delivery in developing countries. The results of the present study suggest that institutional delivery can be positively increased if pregnant women are provided with timely and hassle-free transportation facilities in developing countries as well. To provide timely and hassle-free transport facilities to the community, it is necessary that the services should be evaluated in a time frame, and the need-based initiatives should be taken to improve the quality of services.
Conflicts of interest/funding
No conflict of interest. No funding.
Acknowledgements
The authors are grateful to the Administration of the UT of Dadra & Nagar Haveli for support in data collection.