


Introduction
Road traffic accidents (RTA) are a common cause of pediatric trauma death and disability, constituting a worldwide loss of financial resources as well as a loss of potential manpower.Reference Danseco, Miller and Spicer1-Reference Nordberg3 The majority of RTA are due to preventable causes, and the outcomes for victims have been reported to be due mainly to availability of timely and appropriate rescue teams and medical management.Reference Zargar, Sayyar, Shadman, Kaviani and Tarighi4, Reference Roudsari, Shadman and Ghodsi5 The prevention of RTA has been noted to be more cost-effective compared to material and resources required for adequate treatment of victims.Reference Diamond, Parkin and Wales6 In many developed countries, efforts to reduce RTA incidence and organize emergency prehospital services have significantly improved outcomes of victims.Reference Pearson and Stone2, Reference Durkin, Laraque, Lubman and Barlow7
There is an urgent need to educate children, drivers, the general public, and government policy makers on the consequences of RTA to encourage the adoption of measures aimed at RTA prevention. This is particularly important in developing countries, where RTA involving pediatric victims are reported to be common and increasing in frequency, and where there is a shortage of facilities and skilled personnel required for adequate treatment of RTA victims.Reference Asogwa8-Reference El-Sadiq, Norman, Lloyd, Romilly and Bener10 In most developing countries, policy makers are faced with a lack of data on pediatric RTA.Reference Al-Shammari, Bendak and Al-Gadhi11 Information on pedestrian accidents is scarce, and this has served as an obstacle for efforts to reduce these types of trauma.Reference Al-Shammari, Bendak and Al-Gadhi11 Unlike the case with adult patients,Reference Siram, Oyetunji and Khoury12, Reference Roudsari, Sharzei and Zargar13 the factors influencing the occurrence of pediatric RTA, including the mode of referral and presentation, and the spectrum of injuries sustained, have not been adequately reported in the sub-Saharan African subregion.
The objective of this study was to report on the causes of pediatric RTA, the prehospital care, the pattern of presentation, and the spectrum of injuries resulting in pediatric deaths, and to make suggestions based on the study data that may help in reducing RTA incidence and enhance the overall survival of RTA victims.
Methods
This was a five-year retrospective analysis of pediatric RTA in a Nigerian referral trauma and pediatric surgical center. The records of all children involved in RTA over five years (January 2006-December 2010) at the University of Benin Teaching Hospital were analyzed. The 700-bed hospital, which houses a Level 1 Trauma Center and a standard pediatric surgical center, is located in densely populated Benin City in the southern part of Nigeria. It receives RTA cases from the city and from other health care institutions in Edo and neighboring states, from a distance of up to 350 km. Following Local Ethics Committee approval, the case files of all pediatric RTA, deaths, and dead on arrival (DOA) patients were extracted from the Medical Records Department, and corroborated with records obtained from the pathological day book of the Pathology Department. Two cases were excluded from the study, one because the mechanism of injury was not documented, and one because the case file was not available.
Data collected included age, gender, cause of RTA, mechanism and type of injury, rescue team, injury to hospital arrival time, mode of referral, clinical condition on arrival, resuscitation and definitive treatment, duration of hospitalization, challenges and postmortem findings. Data were entered into Microsoft Office Excel 2007 (Microsoft Corp, Redmond, Washington USA) and analyzed as counts, frequency, and percentages. Continuous data were expressed as mean with standard deviations, and categorical data were analyzed using the Chi-square test with a P value < .05 regarded as statistically significant. The results were then tabulated in tables and figures.
Results
A total of 26 children (constituting 18% of 143 pediatric RTA cases treated during the study) died. Ages ranged from less than one to 18 years (mean 9.3 ± 5.2) and included 18 males and 8 females, with a male to female ratio of 2.3:1. Figure 1 and Table 1 depict the age group involvement in, and deaths following, RTA. Children in the age group 11-15 years accounted for 46 (32.2%) of those involved in RTA, while children in the age group 6-10 years accounted for the highest percentage, 10 (38%), of the 26 deaths. As shown in Table 2, 52 (36.4%) of the total pediatric victims of RTA were pedestrians; 22 (42.3%) were crossing roads and 30 (57.7%) were selling wares on the side of the road. In total, 15 (58%) of those who died were involved in automobile accidents and 11 (42%) were motorcycle accident victims. No statistical difference was observed when the 15 deaths recorded among the total 67 (46.9%) children involved in automobile accidents were compared with the 11 deaths following 76 (53.1%) motorcycle accidents (P = .31). Seven of those who died from automobile accidents were pedestrians, while eight were passengers. Similarly, of the 11 who died from motorcycle accidents, seven were pedestrians and four were passengers. Of the total 14 pedestrian children who died, eight were children selling wares by the side of the road, while the others were crossing roads that had no road traffic signs or traffic control.
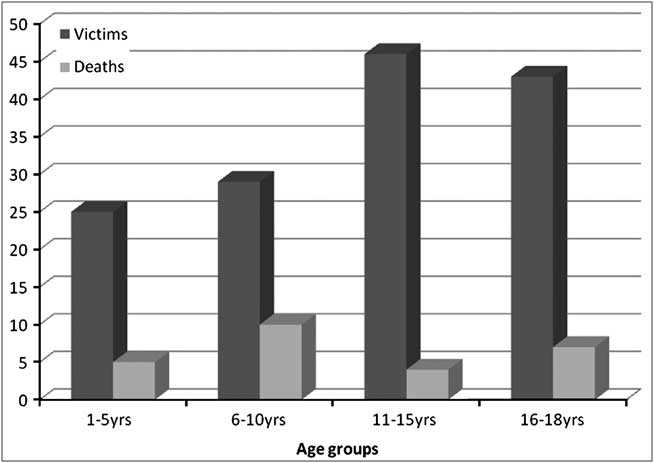
Figure 1 Age distribution of deaths
Table 1 Patient profile of Benin pediatric road traffic accidents in the Center (n = 143)
Table 2 Analysis of the pediatric road traffic accident victims and deaths at Benin City centre in 2006-2010 (n = 143)
Among those passengers who died, head-on collision with another vehicle or stationary object accounted for six deaths, while rollover of a vehicle due to a burst tire or a pothole was recorded in seven. Of the total RTAs, 21 children wore seat belts or were strapped into car seats, while 25 were not restrained. Of the eight passengers who died, two wore seat belts or were strapped into car seats, with no statistical significance compared to those who did not have restraints (P = .37). Four children died among the 14 front seat passengers, and four among 32 rear seat passengers (P = .222). Of the motorcycle passengers, none of those who wore protective crash helmets at the time of accident died, while four died among those who did not wear helmets. First responders, transport vehicles and the reasons or payers for transfer to the study center are depicted in Table 1. There were no organized emergency prehospital services provided for study subjects. Sympathizers or passers-by served as rescuers, providing first aid and taking victims to the study hospital, mainly via public transport. A significant statistical difference was observed when deaths among those arriving via public transport were compared with those arriving via ambulance, police, or road safety vans (P = .0035). Sympathizers or passers-by reported some drivers of the vehicles to be under the influence of alcohol, as the drivers smelled strongly of alcohol at the scene of accident. Accidents associated with alcohol intoxication resulted in more severe injuries and accounted for the majority of deaths (P < .0001).
An average time lag of 18 hours (range one hour to four days) elapsed between the accidents and presentation. Figure 2 shows the mode of referral of those who died after they were involved in the accident. Fourteen (54%) of the dead victims presented directly from the scene of the accident to the study center between one and 12 hours after the accident; those who were referred from other health care institutions presented much later. Deaths were more frequently recorded among those referred late, because they arrived in severe clinical compromise compared to those who came directly from the accident scene (P < .0001). Four children were pronounced dead upon arrival, while the others were hospitalized for between one hour and two weeks before death. Of the 22 children hospitalized before death, particularly among those who were referred from other health care centers, severe clinical compromise due to shock, sepsis, and multiple organ dysfunction posed challenges.

Figure 2 Mode of referral for victims who died
As depicted in Table 2, analysis of the site and type of injuries revealed that head injury sustained by 17 children resulted in 14 (54%) of the 26 deaths, and was statistically significant when compared to other causes of deaths (P < .0001). This was followed by multiple injuries and skeletal trauma recorded as the cause of death in eight (31%) cases. Blunt chest and abdominal trauma was associated with three deaths (12%), and neck injury with transection of spinal cord at C4 resulted in one (4%) death. Correlation of clinical with postmortem examinations findings showed that 13 (including the five motorcycle riders who did not wear protective crash helmets) with head injury had skull fracture, cerebral contusion/laceration, and intracranial hemorrhage, with one also herniating the brainstem. Lung and cardiac contusion, and hemopnuemothorax were findings in three children following blunt chest trauma, while splenic and liver laceration resulting in hemoperitoneum and shocked kidney with acute tubular necrosis were recorded in four children with multiple and blunt abdominal trauma. Femoral fracture, which occurred in multiple injured patients, was the commonest skeletal injury, and resulted in four deaths.
Discussion
The number of pediatric RTA in this study, the majority of which were preventable, were consistent with earlier reports from developing countries.Reference Asogwa8-Reference Roudsari, Sharzei and Zargar13 This study showed that 18% of mortalities occurred among children referred and managed at other institutions following the accidents. Although this finding agreed with results from similar settings in sub-Saharan Africa, it was high compared to reports from more organized settings where the reported mortalities among affected children over a similar duration were lower.Reference Naci, Chisholm and Baker14-Reference Miller, Baig, Hayes and Elton17 The male to female mortality ratio of 2.3:1, with mean age of 9.3 ± 5.2 years, along with children in age group 6-10 years having the highest mortality rate, corresponded with other reports in the subregion.Reference Asogwa8-Reference Roudsari, Sharzei and Zargar13 Head injury, which resulted in 54% of the deaths, is reported as the leading cause of all adult and pediatric trauma deaths globally.Reference Roudsari, Shadman and Ghodsi5, Reference Naci, Chisholm and Baker14 Skull fracture, cerebral contusion and laceration, intracranial hemorrhage, lung and cardiac contusion, hemopnuemothorax, splenic and hepatic rupture, femoral fracture, hemorrhagic shock, and shocked kidney with acute tubular necrosis were clinical and postmortem findings resulting in mortality, and corresponded with findings in previous reports in the African subregion.Reference Asogwa8, Reference Bombom and Edino9, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18
Unlike developed countries, many roads in the sub-Saharan region have no traffic signs, traffic control system, or pedestrian walkways. As shown in this study, the risk for pediatric road traffic injury was compounded by underage children who, owing to financial constraints in their families, sold their wares on the roadside in order to raise money to pay school fees.Reference Asogwa8, Reference Bombom and Edino9, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18 Consequently, preventable pedestrian accidents were high, and accounted for 54% of all pediatric RTA deaths in this study. Moreover, in Nigeria, there is no legislation against alcohol use in public places, while operating machinery or while driving vehicles.Reference Bernard and Gupta19 Therefore, many accidents that could have been prevented appeared to be directly influenced by alcohol intoxication, as many drivers smelled strongly of alcohol at the scene of accidents. Other significant and contributory factors to RTA, as also reported in other studiesReference Zargar, Sayyar, Shadman, Kaviani and Tarighi4, Reference Asogwa8-Reference El-Sadiq, Norman, Lloyd, Romilly and Bener10, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18 were poorly maintained roads with unexpected potholes, and vehicles in poor driving condition with worn-out tires that easily burst. An effective Vehicle Inspection Officer (VIO) and Federal Road Safety Commission (FRCS) that ensured road worthiness of vehicles and enforced safe driving could have helped to prevent some of the accidents in this and earlier studies.Reference Zargar, Sayyar, Shadman, Kaviani and Tarighi4, Reference Asogwa8-Reference El-Sadiq, Norman, Lloyd, Romilly and Bener10, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18
The United Nations Decade of Action for Road Safety 2011-2020, co-sponsored by more than 90 countries, aims to save lives by halting the increasing worldwide trend in road traffic deaths and injuries.20 The implementation of this resolution in sub-Saharan Africa could result in reduction of the rate of road traffic deaths. In Nigeria, the Save Accident Victims Association of Nigeria (SAVAN) was established as a non-governmental organization (NGO) to rescue accident victims, provide first aid, and refer patients to the study trauma center or any other nearby trauma center. In addition, the organization helps to educate the general public on accident prevention, and helps train paramedic staff who serves as rescue teams and provides prehospital treatment to RTA victims.
The frequency of deaths following motorcycle accidents and that of automobile accidents (58% versus 42%) was similar to those reported in earlier studies.Reference Miller, Baig, Hayes and Elton17, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18 A high rate of motorcycle accidents may be a direct consequence of the use of motorcycles as a means of public transport in this setting, with the incidence reported to be lower in regions where motorcycles are not used for public transportation.Reference Zargar, Sayyar, Shadman, Kaviani and Tarighi4, Reference Miller, Baig, Hayes and Elton17, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18, Reference Markogiannakis, Sanidas and Messaris21 In many countries, the use of seat belts and pediatric car seats are required, and children usually are secured in a car seat in the rear seat while traveling. This has been reported to reduce the number of deaths by preventing severe, multiple, and head injuries following RTA.Reference Zargar, Sayyar, Shadman, Kaviani and Tarighi4, Reference Naci, Chisholm and Baker14, Reference Bener, Abu-Zidan, Bensiali, Al-Mulla and Jadaan22 It was observed in this study that only two older children traveling in vehicle wore seat belts, and no younger children were strapped into car seats, with many sitting in the front seat at the time of accident. This may help explain the many cases of severe multiple injuries and the high number of head injuries recorded in this and similar studies in this African subregion.Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18, Reference Odebode and Abubakar23 The use of helmets by motorcycle riders is well established in many countries, and has been reported to reduce the severity of head injuries following crashes.Reference Lin, Hwang and Kuo24, Reference Liu, Iyers, Norton, Boufous, Blow and Lo25 This, as observed in similar studiesReference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18, Reference Adogu and Ilika26 could partly explain the severity of head injuries reported in this study, as none of the motorcycle riders or passengers who died wore helmets.
Before inauguration of the SAVAN program, many deaths after RTAs were related to the lack of organized trauma rescue teams and emergency prehospital services that are readily available in other settings.Reference Pearson and Stone2, Reference Durkin, Laraque, Lubman and Barlow7 Children who sustain a wide spectrum of injuries, including cardiac, cervical spine, and brain injuries, have been reported to survive in more organized settings with prompt, adequate, and effective accident rescue teams and available intensive care units.Reference Pearson and Stone2, Reference Calleja, Delgado, Elias, Sainz, Gonzalez and Esteban27 The rescue, prehospital treatment, and transportation provided by sympathizers and passers-by in this study may not have been adequate, as these people were lay public with no facilities or formal training in handling accident victims. Moreover, poor awareness as to where to transport victims was a problem, because medical attention was sought for a majority of the injured children in privately owned clinics, chemist shops or pharmacies, and even in traditional African clinics. This resulted in unnecessary delay in presentation, which led to deaths as also reported by other authors.Reference Asogwa8, Reference Bombom and Edino9, Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18 This delay in adequate trauma care allowed time for deterioration in clinical parameters, and children were referred when they failed to respond to treatment, arriving at the study center with irreversible complications.Reference Solagberu, Ofoegbu, Nasir, Ogundipe, Adekanye and Abdur-Rahman18 This study was undertaken at a referral center located in a city, and may not reflect the true incidence, causes and injury severity for pediatric RTA deaths in all of this African subregion. This is because many RTAs and deaths occur in remote areas without advanced referral centers, and to develop a full understanding of the problem of RTA injuries and deaths requires a prospective nationwide study.
Conclusion
Pediatric RTA deaths in the setting described were due mainly to preventable causes such as driving on bad roads with no traffic signs, use of vehicles in poor driving condition, alcoholic intoxication while driving, placing children in the front seat with no seat belt or pediatric car seat, and failure by motorcycle riders to use helmets. Severe multiple, head, cardiac, and solid visceral injuries led to majority of the deaths. These were compounded by the absence of organized rescue teams, inadequate emergency prehospital services, hazardous transportation to the referral center, and late referral of many victims when irreversible complications set in.
To decrease pediatric RTA deaths and injuries in Nigeria, government organizations such as the VIO and FRCS should be reactivated, to remove vehicles in poor driving condition from the road and ensure road users comply with driving rules. The use of protective helmets should be made compulsory for all motorcycle drivers and passengers to reduce severe head injury. The full implementation, especially in sub-Saharan Africa, of the United Nations Decade of Action for Road Safety 2011-2020 (A/64/255) and the establishment of SAVAN in African subregions are advocated. Volunteers should be encouraged to train as accident rescue team members and paramedics, to provide first aid to accident victims and refer them appropriately for definitive treatment. The government should prohibit the use of alcohol while driving, and offenders should be reported to appropriate authorities. Efforts should be made by road maintenance agencies to improve the condition of roads, including placement of road traffic signs and construction of pedestrian walkways. Children should be taught how to cross roads, and be prevented from the roadside sale of wares. Older children should be taught to use seat belts, and young children should be placed in pediatric car seats in the rear seat.
Abbreviations
- FRCS:
Federal Road Safety Commission
- RTA:
road traffic accident
- SAVAN:
Save Accident Victims Association of Nigeria
- VIO:
Vehicle Inspection Officer




