Introduction
Trauma is the leading cause of death in the United States for people under the age of 44. 1 Thoracic injuries may be a contributing factor in up to 60% of deaths in the setting of multi-system trauma. 2 Tension pneumothorax can lead to death within minutes, can be temporized by the use of needle thoracostomy (NT), and is one of the few life-threatening thoracic injuries that can be treated in the prehospital setting. 2 Needle thoracostomy is also one of the few interventions that has been shown to make a difference in outcomes for prehospital traumatic cardiac arrest.Reference Lockey, Crewdson and Davies 3 - Reference Weichenthal, Crane and Rond 5
The American College of Surgeons (Chicago, Illinois USA) Advanced Trauma Life Support (ATLS) and Prehospital Trauma Life Support (PHTLS) courses currently recommend NT as a treatment for presumed tension pneumothorax until a tube thoracostomy can be performed, and a majority of urban Emergency Medical Service (EMS) systems allow the use of NT in patients with traumatic cardiac arrest or severe chest trauma. 2 , Reference Butler, Giebner and McSwain 6 - Reference Warner, Copass and Bulger 9 Currently, ATLS recommends NT with a 18-guage 5.0-cm intravenous (IV) catheter inserted in the second intercostal space (ICS) at the midclavicular line (MCL), and studies have supported this recommendation to be safe and effective. 2 , Reference Weichenthal, Crane and Rond 5
Other research suggests that NT failure may be associated with chest wall thickness and IV catheter lengths inadequate for complete chest wall penetration.Reference Schroeder, Valdez and Krauthamer 10 - Reference Zengerink, Brink, Laupland, Raber, Zygun and Kortbeek 12 Chest wall penetration may be achieved when NT is performed in alternative anatomical locations such as the fourth or fifth ICS at the anterior or midaxillary line (MAL), and/or with IV catheter lengths greater than previously recommended.Reference Inaba, Branco and Eckstein 13 - Reference Sanchez, Straszewski and Saghir 18 In one metanalysis, researchers found that the estimated IV catheter length for successful chest decompression was 6.4-cm.Reference Clemency, Tanski, Rosenberg, May, Consiglio and Lindstrom 19
Needle thoracostomy with a 14-guage 8.0-cm IV catheter at the second ICS, MCL or at the fourth or fifth ICS anterior axillary line is supported by the most recent PHTLS course and by the Defense Health Board’s (Falls Church, Virginia USA) Committee for Tactical Combat Casualty Care. 20 To date, two studies with human subjects examined NT with an 8.0-cm IV catheter. Using radiographic measurements of NT with 8.0-cm and 5.0-cm IV catheters, one study found greater rates of chest decompression with an 8.0-cm IV catheter, but also theorized higher rates of injury.Reference Chang, Ross and Kiefer 21 Another study found significantly greater rates of chest decompression when an 8.0-cm IV catheter was used for NT compared to a 5.0-cm IV catheter, but did not analyze differences in mortality or clinical improvement between patients with NT inserted at the second ICS versus the fourth ICS.Reference Aho, Thiels and El Khatib 22
The purpose of this study is to compare overall mortality, efficacy, and complications of patients receiving two different types of NT procedures in an EMS system that includes urban, rural, and wilderness environments.
Methods
This was a before and after observational study of all patients who underwent prehospital NT in the jurisdiction of the Central California EMS Agency (CCEMSA; California USA) during the time period of May 7, 2007 through January 30, 2016.
The CCEMSA serves four counties (Fresno, Kings, Madera, and Tulare) with a wilderness, rural, suburban, and urban catchment of greater than 1.6 million people. 23 It is a two-tiered EMS system, with the first response staffed by emergency medical technician-firefighters who are trained to provide Basic Life Support, and the second tier staffed by paramedics who are trained to provide Advanced Life Support. There is one primary prehospital provider for the CCEMSA, but there are also six smaller provider agencies, a mixture of fire-service-based and private companies that provide care in the more remote areas of the jurisdiction. There is one aeromedical provider that responds to field calls that is staffed by a nurse, a paramedic, and a pilot. The helicopter is simultaneously dispatched to some scenes based on mechanism and distance from a receiving hospital, or an aeromedical response can be requested by field crew. Community Regional Medical Center (CRMC; Fresno, California USA) is the only level-one trauma center for the region and, with rare exceptions, receives all patients suffering from serious trauma.
Care by both first responders and paramedics is protocol-driven with the option to contact a base hospital for further orders or assistance. There are 37 paramedic treatment protocols that are based on chief complaint. The trauma treatment protocol allows for the use of NT in the setting of trauma arrest (TA), and when tension pneumothorax is suspected and the patient is hypotensive with a systolic blood pressure of less than 90. Before March 1, 2013, NT procedure protocol included using a 14-gauge IV catheter at least 5.0-cm long for adult patients and placement of the NT at second ICS, MCL on the side with decreased breath sounds or bilaterally for TA. This procedure is performed after initial stabilization on scene and only once the patient has been placed in the ambulance (ground or air). After March 1, 2013, modifications to the NT procedure protocol included using a 10-gauge IV catheter at least 9.5-cm long for adult patients with placement at fifth ICS, MAL on the side with decreased breath sounds or bilaterally for TA. This procedure occurs on scene during the initial stabilization (Appendix A; available online only).
Beginning in 2007, the CCEMSA required its providers to maintain an electronic prehospital care report (PCR). A PCR is electronically entered by paramedics for all encounters in the CCEMSA’s jurisdiction into a program named SIMON (American Ambulance; Fresno, California USA). This information is then stored in an electronic data base called NOMIS (American Ambulance; Fresno, California USA). SIMON and NOMIS are software programs that were developed in-house by American Ambulance and continue to be managed and monitored by this agency. SIMON is designed so that all key information must be entered by the paramedics before they can finish and print the PCR. SIMON first became compliant with the National EMS Information System (NEMSIS; Salt Lake City, Utah USA) in 2010.
NOMIS was queried for all patients who accessed EMS during the study period with a chief complaint of trauma and who also underwent NT. Prehospital data collected from NOMIS records included: age; gender; personal identifiers; mechanism of injury; call status (stat trauma [ST] or TA); type of NT (unilateral or bilateral); positive response to NT (defined as increased oxygen saturation by 10%, increased systolic blood pressure >20 mm Hg, objective findings of improved mental status or improvement in dyspnea, or return of spontaneous circulation); need for repeat NT; transport times; and mode of transportation. The CCEMSA defines a ST as a patient with a potentially life- or limb-threatening condition, who is unstable or has a rapidly changing status as identified by the assessment and vital signs. A TA is a patient found in the setting of trauma who is pulseless and not breathing.
Prehospital records were then linked to hospital and trauma registry records using personal identifiers including name, age, date of service, and medical record number. Hospital data collected included: need for repeat NT in the emergency department (ED), tube thoracostomy placement, reported complications due to NT, and final outcome. The trauma registry was utilized to obtain Injury Severity Scores (ISS). Patients were categorized into two cohorts based on NT procedure, corresponding to date of service and changes in CCEMSA procedure protocol. The MCL cohort of patients were treated with prehospital NT with a 14-guage IV catheter at least 5.0-cm long at second ICS, MCL from May 7, 2007 through February 28, 2013, and the MAL cohort of patients were treated with prehospital NT placement with a 10-guage IV catheter at least 9.5-cm long at fifth ICS, MAL from March 1, 2013 through January 30, 2016.
All data were manually abstracted by principal investigators and entered into an Excel 2010 Spreadsheet (Microsoft; Redmond, Washington USA) where means and standard deviations were calculated, when appropriate.
Data were then imported into SPSS software, version 24.0.0 (IBM; Chicago, Illinois USA) where first, a univariate analysis was conducted using chi-squared and independent two-tailed t-tests to compare the categorical data and means, respectively, between the before and after groups. Univariate analysis was then conducted with all of the study data to look for any variables significantly related to the major outcome of death. A multivariate model was then constructed, using binary logistics regression, to further assess the relation between final outcome (mortality) and the variables initially found to be significant in the univariate analysis.
Primary outcomes included overall mortality, efficacy, and complications. A positive outcome was defined as survival to hospital discharge. Efficacy was defined as a positive response to NT in the field, including: increased oxygen saturation, increased blood pressure, improvement in mental status, subjective improvement in reported dyspnea in alert patients, or return of spontaneous circulation in patients with TA. Complications included any reported iatrogenic injury, including vascular or pulmonary injuries.
Secondary outcomes included whether differing mechanisms of injury (blunt versus penetrating), call status (ST versus TA), EMS transport mode (ground versus helicopter), or transport time impacted mortality.
This study was approved and written informed consent was waived by the Institutional Review Board at CRMC and by the CCEMSA.
Results
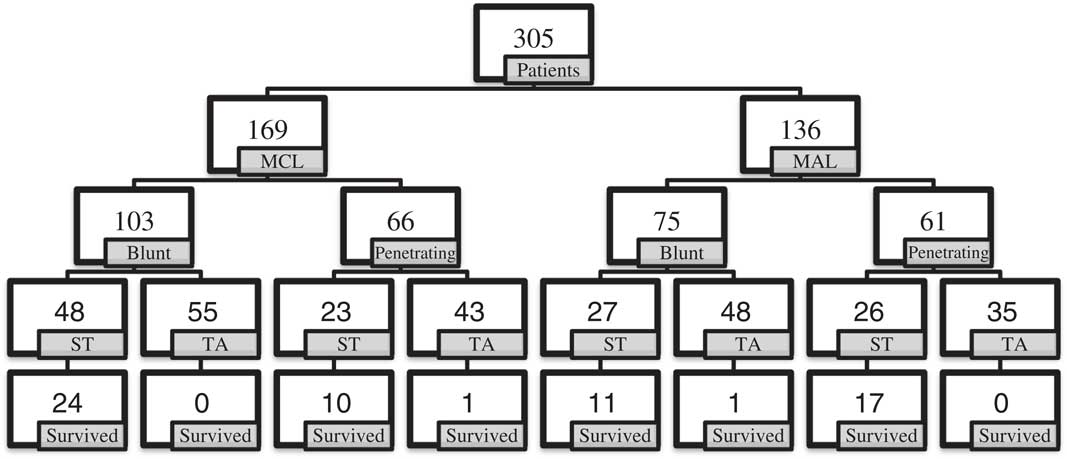
One-hundred and sixty-nine people made up the MCL group, who underwent NT at the second ICS, MCL before the change in policy on March 1, 2013; and 136 people were included in the MAL group who had NT performed at the fifth ICS, MAL after the change of policy (Figure 1). There was no major difference regarding demographics between the two groups; however, there was a significant difference with regard to the mean ISS, with the MAL group being less injured (69.2 versus 64.5; P=.007; Table 1).

Figure 1 Flow Diagram of Before and After Patients Showing Breakdowns with Regard to Mechanism (Blunt verses Penetrating), Call Status, and Survival to Hospital Discharge. Note: MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line; MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line. Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line; NT, needle thoracostomy; ST, stat trauma; TA, trauma arrest.
Table 1 Demographics Comparing MCL and MAL Patients

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
c Age=mean average age in years.
d Weight=mean average weight in kilograms.
The overall mortality for both groups was the same (79%). There were no significant differences in situational factors or clinical efficacy after NT between the two groups (Table 2). Blunt trauma was the most common mechanism of injury in both groups, with motor vehicle collisions accounting for the majority of blunt traumas. Gunshot wounds were the main cause of penetrating trauma in both groups (Table 3).
Table 2 Situational and Outcomes Variables Comparing MCL and MAL Patients

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line; NT, needle thoracostomy.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
Table 3 Mechanism of Injury for all Patients in Relation to NT Procedure, Call Status, and Mortality

Abbreviations: ATV, all-terrain vehicle; GSW, gunshot wound; MAL, mid-axillary line; MCC, motorcycle collision; MVC, motor vehicle collision; MVE, motor vehicle ejection; NT, needle thoracostomy; ST, stat trauma; SW, stab wound.
a %=percentage of mechanism subcategories for both groups.
b MAL %=percentage of mechanism subcategories among patients with NT in the anterior axillary line.
There was a higher number of female patients (18% versus 6%; P=.021) and lower mean ISS (48.08 versus 61.23; P<.001) in the MAL group when looking only at ST patients. Clinical change after NT was more likely for patients presenting as ST in both the MCL (63% versus 24%; P<.001) and MAL group (72% versus 31%; P<.001). There were no significant differences between the two groups with regard to demographics and outcomes in patients presenting in TA.
When data for the entire study period were analyzed, six factors were found to be statistically significant with regard to the final outcome of death: ST call status (P<.001; 95% CI, 0.023-1.241); fluid bolus in the field (P=.02; 95% CI, 0.117-4.752); helicopter transport (P<.001; 95% CI, 0.205-3.395); prolonged transport time (P=.003; 95% CI, 0.159-2.339); ISS (P<.001; 95% CI, 1.115-1.255); and clinical change after NT (P=.002; 95% CI, 0.013-0.386; Table 4). However, the multivariate model that was constructed only supported that ISS and documented clinical change after NT were statistically significant.
Table 4 Reported Positive Responses to NT in the Field

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line; NT, needle thoracostomy.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
A subset analysis was completed based on mechanism of injury. Of the patients with blunt trauma, there were 103 in the MCL group and 75 in the MAL group with no significant differences in age, ISS, call status, transportation method, clinical change, or mortality (Tables 5 and 6). Four factors were found to be statistically significant with regard to the final outcome of death: ST call status (P<.001; 95% CI, 0.013-6.690); helicopter transport (P=.004; 95% CI, 0.016-19.568); ISS (P<.001; 95% CI, 1.152-1.501); and clinical change after NT (P<.001; 95% CI, 0.003-0.653). From these factors, a multivariate model was constructed that found only ISS and clinical change after NT to be statistically significant.
Table 5 Situational and Outcome Variables of Patients with Blunt Trauma Who Underwent MCL versus MAL

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line; NT, needle thoracostomy.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
Table 6 Demographics among Patients with Blunt Trauma in MCL versus MAL

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
c Age=mean average age in years.
d Weight=mean average weight in kilograms.
Of the patients with penetrating trauma, there were 66 in the MCL group and 61 in the axillary group. Patients with penetrating trauma in the MAL group were less sick than patients in the anterior group (59.67 versus 69.50; P=.002), but there were no differences in mortality (Tables 7 and 8). Four factors were found to be statistically significant with regard to the final outcome of death: ST call status (P<.001; 95% CI, 0.018-14.937); helicopter transport (P<.001; 95% CI, 0.013-1.489); ISS (P<.001; 95% CI, 1.190-1.322); and clinical change after NT (P<.001; 95% CI, 0.008-1.290). From these factors, a multivariate model was constructed that found only ISS to be statistically significant.
Table 7 Situational and Outcomes Variables of Patients with Penetrating Trauma in MCL versus MAL

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line; NT, needle thoracostomy.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
Table 8 Demographics of Patients with Penetrating Trauma in MCL versus MAL

Abbreviations: MAL, mid-axillary line; MCL, mid-clavicular line.
a MCL=patients who underwent NT at the 2nd intercostal space, mid-clavicular line.
b MAL=patients who underwent NT at the 5th intercostal space, mid-axillary line.
c Age=mean average age in years.
d Weight=mean average weight in kilograms.
Of the patients who received NT in the field, only three required repeat NT due to catheter dislodgement. For patients who initially received NT at the MCL, nine (5%) underwent repeat NT in the ED and 80 (47%) had tube thoracostomy in the ED. Among patients who initially received NT at MAL, 14 (10%) underwent repeat NT in the ED and 70 (51%) had tube thoracostomy in the ED. All NT or tube thoracotomies in the ED involved the affected side(s) where NT was performed in the prehospital setting. The majority of patients who did not undergo tube thoracostomy in the ED were either declared dead on arrival or shortly after arrival in the ED (less than 10 minutes of attempted resuscitation), or they went to the operating room for emergent sternotomy or laparotomy in addition to tube thoracostomy. One patient was stable without tube thoracostomy but suffered severe traumatic intracranial hemorrhages.
No complications to prehospital NT or misplacement of the catheter were reported in hospital records, including patients who underwent an operative thoracotomy (11 in the MCL anterior group and 25 in the MAL group). The two patients who survived TA were admitted to the trauma intensive care unit and later discharged to subacute facilities with significant neurologic disabilities.
Discussion
Tension pneumothorax is a rapidly progressive and life-threatening process that, if not quickly recognized and treated, leads to cardiovascular collapse.Reference Leis, Hernandez, Blanoc, Paterna, Hernandez and Torres 4 , Reference Bulger, Nathens, Rivara, MacKenzie, Sabath and Jurkovich 7 , Reference Eckstein and Suyehara 8 Needle thoracostomy can decrease intrathoracic pressure temporarily to allow adequate venous return to the heart until tube thoracostomy can be performed, and it is the only tension pneumothorax treatment technique available to most ground paramedics and aeromedical teams in the United States. 2 , Reference Mistry, Bleetman and Roberts 24 Currently, ATLS recommends NT be performed with a 5.0-cm IV catheter at the second ICS, MAL, but new research suggests IV catheter lengths of 8.0-cm or greater and NT at the fourth or fifth ICS, anterior or MAL may be more effective.Reference Chang, Ross and Kiefer 21 , Reference Aho, Thiels and El Khatib 22
This study showed no difference in mortality or complication rates between patients who underwent NT with a 5.0-cm IV catheter at second ICS versus patients who underwent the procedure with an 8.0-cm IV catheter in the fifth ICS. The findings of this study support that NT is a safe procedure regardless of the site where it is performed or the catheter size. Being less injured and having a reported positive response to the procedure were the only two factors found to predict survival. In subset analyses of trauma mechanisms, there were no significant differences in mortality, and being less injured was found to predict survival.
The overall mortality of patients in this study (79%) is higher than those reported in other studies, one of which had a mortality rate as low as 28%.Reference Eckstein and Suyehara 8 This may, in part, be due to the fact that 59% of patients in this study presented in TA, whereas in the above referenced study, the number of patients presenting to EMS without vital signs was only 18%.Reference Eckstein and Suyehara 8
This study is also unique in that the patients undergoing NT suffered from both blunt and penetrating trauma. Previous studies looking at NT consisted of an overwhelming majority of patients who sustained blunt trauma. The mixture of blunt and penetrating mechanism in this study is more reflective of trends for trauma that have been reported in the literature.Reference Champion, Copes and Sacco 25 - Reference Minei, Schmicker and Kerby 27
Previous studies have suggested that NT is a relatively infrequently used procedure despite its general safety. The MCL group of this study supports this with only 169 NT preformed in a five-year period for an average of 2.8 per month. With the change in policy, however, the number of NT increased to an average of 5.7 per month. The patients with penetrating trauma treated with NT in the MAL group were also less ill, based on their ISS, than the MCL group. Interpreting this trend of increased usage of NT in the MAL group is challenging. Is it just the result of the introduction of a new policy, increasing the likelihood of prehospital personnel using NT, or does it represent an increased comfort in performing the procedure? Increased comfort in performing the procedure could both be due to increased opportunities to utilize it early in the care of patients and also increased ease in anatomical identification of where to perform the procedure, a concept supported by a cadaver study where NT at the fifth ICS was successful 100% of attempts versus 58% at the second ICS.Reference Inaba, Branco and Eckstein 28 While the relative increase in NT use could be considered a limitation to the study’s purpose of comparing NT procedural techniques, practically this may represent a larger, system-based improvement in trauma care, as significantly more unstable patients were eligible for operative management.
Limitations
There are several other limitations to this study, the primary one being its observational nature. Investigators only had access to the data entered by the prehospital and hospital personnel, which although well documented due to required electronic PCR templates, may not adequately document some data, such as complications due to NT. They also did not have access to medical examiner records, thus could not report complications due to NT potentially found on autopsy. Further, investigators relied on changes in clinical condition to assess adequate chest decompression with NT, as opposed to studies which utilize advanced imaging techniques to assess catheter penetration of the chest wall. As mentioned, patients who received NT in the MAL group were less sick than those in the MCL group, creating a confounding variable (mean ISS), limiting the value of predicting mortality and survivability between before and MAL groups in the multivariate analysis. Finally, it is difficult to determine how many patients truly had a pneumothorax prior to NT placement, and thus to determine how many iatrogenic pneumothoraxes are caused by NT.
Conclusion
There was no difference in mortality or reported complications between patients who received NT with a 14-guage IV catheter at least 5.0-cm long at the second ICS and those who received NT with a 10-guage IV catheter at least 9.5-cm long at the fifth ICS. The procedure, in both groups, is most beneficial for patients who are unstable but still have vital signs on EMS arrival. The change in policy did increase the frequency in which this procedure was utilized.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1049023X18000316