Introduction
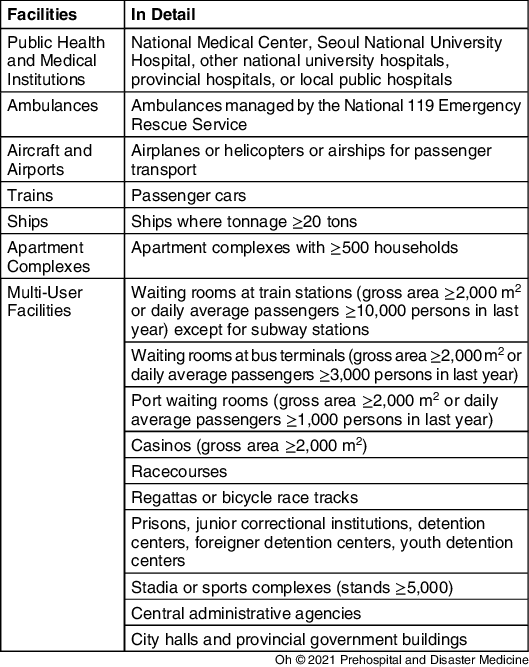
When defibrillation was performed by the public access defibrillation (PAD) program, the survival rate of out-of-hospital cardiac arrest (OHCA) increased significantly. Reference Perkins, Handley and Koster1–Reference Brady, Mattu and Slovis3 Therefore, resuscitation guidelines recommend placement of automated external defibrillators (AEDs) in public areas such as airports, railway stations, bus terminals, sport facilities, shopping malls, offices, and casinos. In South Korea, a law on AEDs (the Emergency Medical Service Act, Article 47, Paragraph 2 [hereafter referred to as “the Act”]) was established in 2007 and stated that AEDs should be installed and managed in specific places (Table 1). 4 In addition, since 2018, a penalty of 500,000 to 1,000,000 Korean Won (420 to 840 USD) was imposed when AEDs were not installed in places required by the Act. Furthermore, by establishing a Good Samaritan Law in 2008 (the Emergency Medical Service Act, Article 5, Paragraph 2), the legal basis for a PAD program was established. 4
Table 1. Places for which Automated External Defibrillator Installation is Required by the Emergency Medical Service Act, Article 47, Paragraph 2

To support the law on AEDs, since 2010, the Ministry of Health and Welfare in South Korea (Sejong, South Korea) has provided guidelines for PAD placement and management. 5 According to the guidelines, installation and usage of AEDs are reported to a public health center by the chief manager of each installed AED, and data are managed by the National Emergency Medical Center (NEMC; Seoul, South Korea). However, the current status of AED placement, usage, and rate of use in South Korea has not been reported. This study was conducted to investigate the current status and effectiveness of installation and usage of AEDs in South Korea. In particular, this study compared the distribution of AEDs and rate of AED use among provinces and places of installation.
Methods
Study Design
This was a retrospective analysis of the prospectively collected NEMC public database. Data were collected from the manager of installed AEDs by officers in the public health centers and transferred to the database. The data regarding installation of AEDs were subsequently open to the public via a website or smartphone application (E-GEN) designed by the Ministry of Health and Welfare. The data on AED usage are also freely available upon request. All data including installation and usage of AEDs were provided as Excel files (Microsoft Corporation; Redmond, Washington USA) from NEMC. This study analyzed data on AED installation collected from 1998 through 2018 and data on AED usage collected from 2012 through 2018.
Compositions of the Dataset
The dataset concerning AED installations included the year of installation, province, name and address of the place of installation, and category of place (whether the place was required or not by the Act). The dataset concerning AED use included usage date (year, month, day, and time); information regarding the place of usage (province, place, and category); and qualifications of the user (non-medical first responders, medical personnel, and unknown). Data on place of installation were divided by 17 major and 110 minor classifications for the purpose of analysis (Supplementary Material, Table S1; available online only). Characteristics regarding places of installation were divided into three areas (public, residential, and other). Among 17 major classifications, public institutions, educational institutions, multi-user facilities, sports facilities, industrial facilities, commercial facilities, gaming facilities, roads and highway service stations, terminals and waiting rooms for public transportation, and correctional facilities were regarded as public areas. Apartment complexes, detached houses, and multi-housing facilities were regarded as residential areas. Medical institutions, transport vehicles, and assisted living/nursing homes were regarded as other areas.
Variables
The number of installed AEDs and rate of use were compared according to province, place of installation, category of place, and characteristics of installed places. As periods of AED use differ, usage of AEDs was compared by using the annual rate of use ([total cases of AED use/total duration of AED use in year] × 100).
Statistical Analysis
Descriptive statistics are reported as mean (95% confidence interval) and categorical variables are reported as frequency (percentage). Differences of frequencies according to time, province, and place were analyzed using one-sample chi-squared tests. Differences in the annual rate of use according to province and place of installation were analyzed using an independent-sample t test, analysis of variance, Mann–Whitney U test, or Kruskal–Wallis test according to the normality of distribution. Data normality was analyzed using the Shapiro–Wilk test or Kolmogorov–Smirnov test. A P value <.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS version 25.0 (IBM Corp.; Armonk, New York USA).
Ethics Statement
This study was exempted from Institutional Review Board approval because it did not include human subjects or personal information (exemption No. 2003-006-19306). All data are open to the public and freely available upon request.
Results
The accumulated number of installed AEDs from 1998 through 2018 was 38,501. Of those, AEDs installed in ambulances or fire engines (n = 2,003) were excluded from the analysis. The accumulated number of incidents of AED usage from 2012 through 2018 was 3,753. After excluding the usage of AEDs installed in ambulances or fire engines (n = 3,315), 438 incidents of AED usage were analyzed.
Descriptive Data
The accumulated number of installed AEDs and annual incidents of AED usage increased every year from 1998 to 2012 (Figure 1). In total, 36,498 AEDs were in place in 2018, and the annual incidents of AED usage reached 184 cases in 2018. Considering the province of installation, AEDs were unequally distributed throughout the nation (Supplementary Material, Figure S1; available online only). Among 36,498 AEDs, 15,385 (42.2%) were installed in Seoul and Gyeonggi-do Province (7,760 [21.3%] and 7,625 [20.9%], respectively). Among the different provinces, in 2018, the number of installed AEDs per 100,000 population was the highest in Jeju (196 AEDs/100,000 population), followed by Jeollanam-do (138 AEDs/100,000 population; Supplementary Material, Figure S2; available online only). Considering the 17 major places of installation, the number of installed AEDs was the highest in apartment complexes, followed by transport vehicles (11,318 [31.0%] and 5,308 [14.5%], respectively; Supplementary Material, Figure S3; available online only). Considering the 110 minor places of installation, 16,007 (43.9%) AEDs were installed in apartment houses and ships (11,318 [31.0%] and 4,689 [12.8%], respectively; Supplementary Material, Figure S4; available online only).

Figure 1. Changes in the Installation and Usage of Automated External Defibrillators in South Korea.
Abbreviation: AED, automated external defibrillator.
Usage of AEDs
The overall annual rate of AED use was 0.38% (95% CI, 0.33-0.44). When evaluated by province, the annual rate of AED use was the highest in Jeju (1.12% [95% CI, 0.52-1.73]), followed by Daegu (0.64% [95% CI, 0.21-1.08]; Supplementary Material, Figure S5; available online only). Although a plurality of AEDs was located in Seoul and Gyeonggi-do, the annual rate of AED use in Seoul and Gyeonggi-do was only 0.56% (95% CI, 0.44-0.69) and 0.19% (95% CI, 0.12-0.26), respectively. Based on the 17 major places of installation, the annual rate of AED use was highest in assisted living/nursing homes (8.64% [95% CI, 3.64-13.65]), followed by terminals and waiting rooms for public transportation (2.26% [95% CI, 1.58-2.94]; Supplementary Material, Figure S6; available online only). The annual rate of AED use in apartment complexes and transport vehicles was only 0.13% (95% CI, 0.08-0.17) and 0.14% (95% CI, 0.04-0.25), respectively. Based on the 110 minor places of installation, the annual rate of AED use was highest in sanatoria (9.15% (95% CI, 3.80-14.51; Supplementary Material, Figure S7; available online only).
Comparison of Required and Non-Required Places
A higher number of AEDs were installed in places required by the Act compared with those not required by the Act (20,678 [56.7%] versus 15,820 [43.3%]; P <.001). However, the annual rate of AED use was significantly higher in non-required places than in required places (0.62% [95% CI, 0.52-0.72] versus 0.21% [95% CI, 0.16-0.25]; P <.001; Figure 2).

Figure 2. Comparison of the Places Required by Law and Places Not Required by Law.
Abbreviations: AED, automated external defibrillator; the Act, Emergency Medical Service Act, Article 47, Paragraph 2.
Comparison of Public and Residential Areas
A higher number of AEDs were installed in public areas compared with that in residential areas (15,395 [42.2%] versus 11,432 [31.3%]; P <.001; in addition, 1,671 [26.5%] AEDs were installed in other areas). The annual rate of AED use was also significantly higher in public areas than in residential areas (0.49% [95% CI, 0.41-0.57] versus 0.13% [95% CI, 0.08-0.17]; P <.001; Figure 3).

Figure 3. Comparison of Automated External Defibrillator Use in Public Areas and Residential Areas.
Abbreviation: AED, automated external defibrillator.
Variations in AED Usage According to Time of Day
Most incidents of AED usage occurred during daytime (06:00-21:00; 90.4%; Supplementary Material, Figure S8; available online only).
Discussion
Although the effectiveness of the PAD program has been confirmed several times, Reference Nakashima, Noguchi and Tahara6–Reference Hallstrom, Ornato and Weisfeldt11 to the best of the authors’ knowledge, the present study is the first to investigate the current status and effectiveness of placement and usage of AEDs in South Korea. In a systematic review, the median survival to hospital discharge ratio when PAD was performed by lay persons after OHCA was 53%. Reference Baekgaard, Viereck, Moller, Ersboll, Lippert and Folke12 Therefore, proper placement of AEDs throughout the nation is essential for the success of the PAD program.
The current study confirmed that the number of installed AEDs in South Korea increased rapidly after two important laws (the law on AEDs and the Good Samaritan Law) came into effect. The strategy of using laws to establish a PAD program has been effective in increasing the absolute number of installed AEDs in South Korea. However, the current study discovered several problems.
First, there were mismatches between the number of installed AEDs and the annual rate of AED use among provinces and places. For example, there was an extremely low rate of AED use in Gyeonggi-do, where a large number of AEDs were installed in apartment complexes (4,472 [58.6%]). The annual rate of AED use in apartment complexes was extremely low. Consequently, the overall annual rate of AED use in Gyeonggi-do decreased. Although the Act dictated installation of AEDs in apartment complexes with ≥500 households, the Act did not propose a minimum number of AEDs. Therefore, some apartment complexes installed an AED in every building, and others installed AEDs in only one or two buildings, especially in the control office. This inconsistent strategy contributed to a different distribution of AEDs in provinces. In contrast, in Jeju Province, only 15 (1.2%) AEDs were installed in apartment complexes.
Second, there was an excess number of AEDs installed in residential areas (31.3% of all AEDs). In Japan 13 and Copenhagen, Reference Folke, Lippert and Nielsen14 the percent of AEDs installed in public areas was 82.4% and 94.2%, respectively. Although 60%-80% of cardiac arrest occurs at home, the effectiveness of AEDs was low in residential areas because of fewer witnessed arrests, lower bystander cardiopulmonary resuscitation rate, and fewer shockable rhythms than that in public areas. Reference Perkins, Handley and Koster1,Reference Weisfeldt, Everson-Stewart and Sitlani15 In addition, several studies reported that there were no advantages when AEDs were applied in residential area, even in the home of high-risk patients. Reference Kiguchi, Kiyohara and Kitamura16,Reference Bardy, Lee and Mark17 On the contrary, many studies showed a survival benefit of AED in public areas. Reference Hallstrom, Ornato and Weisfeldt11,Reference Weisfeldt, Everson-Stewart and Sitlani15,Reference Kiguchi, Kiyohara and Kitamura16 Therefore, a redistribution of AEDs in South Korea is needed to maximize their effectiveness.
Third, because the Act requires installation of AEDs on ships when the tonnage is ≥20 tons, an excess number of AEDs were installed on ships. However, the annual rate of AED use on ships was only 0.15%. As a result, in South Korea, 16,007 (43.9%) AEDs were placed in areas with low usage, such as apartment complexes and ships.
Fourth, there was a mismatch in the number of installed AEDs and the annual rate of AED use between places for which installation was required by the Act and places for which installation was not required. Although the number of AEDs in required places was larger than that of non-required places, the annual rate of AED use was significantly higher in non-required places. This result suggests that places designated by the Act are not as effective.
Placement of AEDs without guidance or evidence regarding effectiveness can result in ineffective installation. Reference Folke, Lippert and Nielsen14,Reference Nichol, Huszti and Birnbaum18 Muraoka, et al recommended six locations for installation, including workplaces, railway stations, hospitals, homes for the aged, other playgrounds, and golf courses, considering the incidence of cardiac arrest, the ratio of ventricular fibrillation, and good neurological outcomes. Reference Muraoka, Ohishi and Hazui19 Several places in the current study showed a higher annual rate of AED use, such as sanatoria, banks, subway stations, civilian medical facilities, senior centers, other playgrounds, resorts, other multi-housing facilities, and swimming pools. Among these, only other multi-housing facilities (comprising housing facilities, including those for individuals who are homeless or disabled) were classified as residential areas. Accordingly, the annual rate of AED use was higher than that of apartment complexes. With the exception of sanatoria and civilian medical facilities, all places were classified as public areas. Patterns regarding the time of AED use also showed that most PAD is delivered in the daytime. Overall, previous evidence and present data show that AEDs should be placed in public places where there is a higher probability of a witnessed cardiac arrest during the day. Reference Brady, Mattu and Slovis3
Limitations
The present study has several limitations. First, only data regarding AED usage were analyzed and not outcome data from patients. In addition, a reported incident of AED use does not certify completion of PAD, as there was an inability to discriminate between simply attaching the pads and actually delivering the shock. Therefore, evidence level of the results was limited. Second, the guidelines state that the manager of installed AEDs should report when AEDs are used. However, there is no fine or penalty if the manager fails to report AED use. Therefore, there is a possibility of missing incidents of AED usage. In addition, there was no penalty for the reporting of AED installation or use in places where AED installation was not mandatory by law (non-required places). Therefore, data on AEDs in such places could be missing. Third, although qualification of the AED user was included in the dataset, 208 (47.5%) cases reported use by unknown rescuers. Therefore, differences in qualifications could not be analyzed according to provinces and places.
Conclusions
There were significant mismatches between the number of installed AEDs and the annual rate of AED use among places. To optimize the benefit of AEDs in South Korea, changes in the policy for selecting AED placement are needed.
Acknowledgement
The authors specially thank Ms. Kyungyi Lim, Korean Association of Cardiopulmonary Resuscitation, for her technical assistance for this study.
Conflicts of interest/funding
The Korean Association of Cardiopulmonary Resuscitation (KACPR) provided the funding needed to prepare and publish this manuscript in 2020. Prof. Gyu Chong Cho is chair of the basic life support committee in the KACPR. The task force team (TFT) for investigating the current status of automated external defibrillator (AED) in South Korea was organized in the KACPR in 2019. All authors are the member of the TFT for AED in the KACPR. All authors declare that they have no competing interests.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1049023X20001508