Introduction
Modern society is dependent upon consistent and reliable energy supplies. In particular, the provision of medical care, in both disaster and nondisaster settings, is reliant highly on large volumes of consistent, high-quality power. Natural, manmade, and technological disasters often have dramatic affects on the energy infrastructure of affected communities. During the acute post disaster phase, this results in a loss of local sustainment and response capabilities. As the response proceeds, significant resources must be dedicated solely to restoring power, importing fuel, and managing energy utilization.
Mobile medical and disaster medical response traditionally relied on diesel generators to supply power. While dependable and widely available, diesel generators have the obvious limitations of needing a steady supply of fuel and of producing local air pollution. In the resource-poor setting of disaster, this can present an obstacle to disaster operations. The 2012 “superstorm” Sandy that decimated parts of New York and New Jersey (USA) demonstrated the fragility of both utilities and fuel supplies as millions were left without heat and power, and fuel shortages were rampant.Reference Neuman 1 , Reference Domm 2
Carolinas HealthCare Systems operates the mobile emergency medical unit (MED-1) hospital fleet. The components of the fleet are outlined in Table 1. Carolinas MED-1 is uniquely capable of providing comprehensive medical care to offer support in disaster relief situations and mass-gathering public events. The MED-1 fleet is comprised of one treatment vehicle and six support vehicles that can provide advanced resources up to and including operative interventions, cardiac monitoring, portable radiology, and intensive care. Carolinas MED-1 has a long history of providing medical care in post disaster settings, including response to Hurricane Katrina (2005; USA) and the devastating 2008 floods in Indiana (USA).Reference Blackwell and Bosse 3
Table 1 MED-1 Fleet

Abbreviations: ICU, intensive care unit; Med-1, Carolinas Medical Center's mobile emergency medical unit.
The MED-1 Green Project (M1G) was initiated to identify improvements that could be made to the MED-1 fleet that would increase energy efficiency, decrease demands on the diesel generators, and expand emergency medical care capabilities. The primary goal was to increase operational independence, allowing for longer deployments in potentially more austere environments. Additional environmental and financial benefits include decreased emissions and decreased expenses from fuel costs.
The first phase of this project was the execution of an energy audit (EA) that quantified the energy usage of MED-1 and identified specific targets for improvement (heating, ventilating, and air conditioning (HVAC); lighting; and medical and clerical equipment). This EA was the first of its kind to quantify energy utilization in large-scale prehospital medical response. The EA also revealed that MED-1's two 100 kVA, 208 V 3-phase generators were operating at a low load capacity, below minimum efficiency, resulting in significant energy waste. As MED-1's power plant was already functioning below its optimum load, implementing energy conservation measures (ECMs) would reduce further the required generator output, but have no effect on fuel utilization. The EA demonstrated that if MED-1 generators could operate at an optimal load, they would increase power generation without any significant change in fuel consumption. The implementation of a microgrid was the proposed solution to address increased generator efficiency while leveraging ECMs.
This report describes the second phase of the M1G investigation of the feasibility and potential benefit of implementing a microgrid to achieve this maximization in efficiency of the existing diesel generators. A microgrid is a localized grouping of electricity generation, energy storage, and loads. Microgrids have seen increasing popularity as they allow a degree of independence from the centralized grid.
While there has been little, if any, utilization of microgrids in mobile applications outside of the military, incorporating them into MED-1's generation system would offer several benefits. First, it would allow for the possibility of distributive energy generation. Distributive generation (DG) allows for multiple energy sources to be harnessed and integrated into a single energy system. With a DG system, alternate sources, such as solar and wind, could be added to the fleet, further decreasing the demands on the diesel generators. Secondly, it would allow integration of an energy storage system (eg, batteries). A comprehensive battery array would enable the generators to operate at their maximum efficient load by diverting “surplus” power into the storage system. Carolinas MED-1 then could operate alternately off the batteries and the generators, meaning the generators could be shut down intermittently creating a substantial fuel savings. Finally, a microgrid offers conditioned power. The electricity produced by the diesel generators is highly variable. A power conditioner provides increased power quality, meaning less variation in voltage magnitude, less transient changes in voltages and currents, and improved harmonic content in the alternating current (AC) waveform. Improved energy quality extends the lifetimes of the sensitive electronic equipment, such as mechanical ventilators, cardiac monitors, and computer systems, employed during patient care in MED-1.
A detailed load analysis of the mobile hospital was performed at two events so that the data could be used for microgrid modeling. These events included a training exercise for supporting the Democratic National Convention (DNC) and the DNC in Charlotte, North Carolina (USA) from September 1-5, 2012. The data were used to model different power-system configurations for the optimal microgrid design.
Methods
Load Analysis
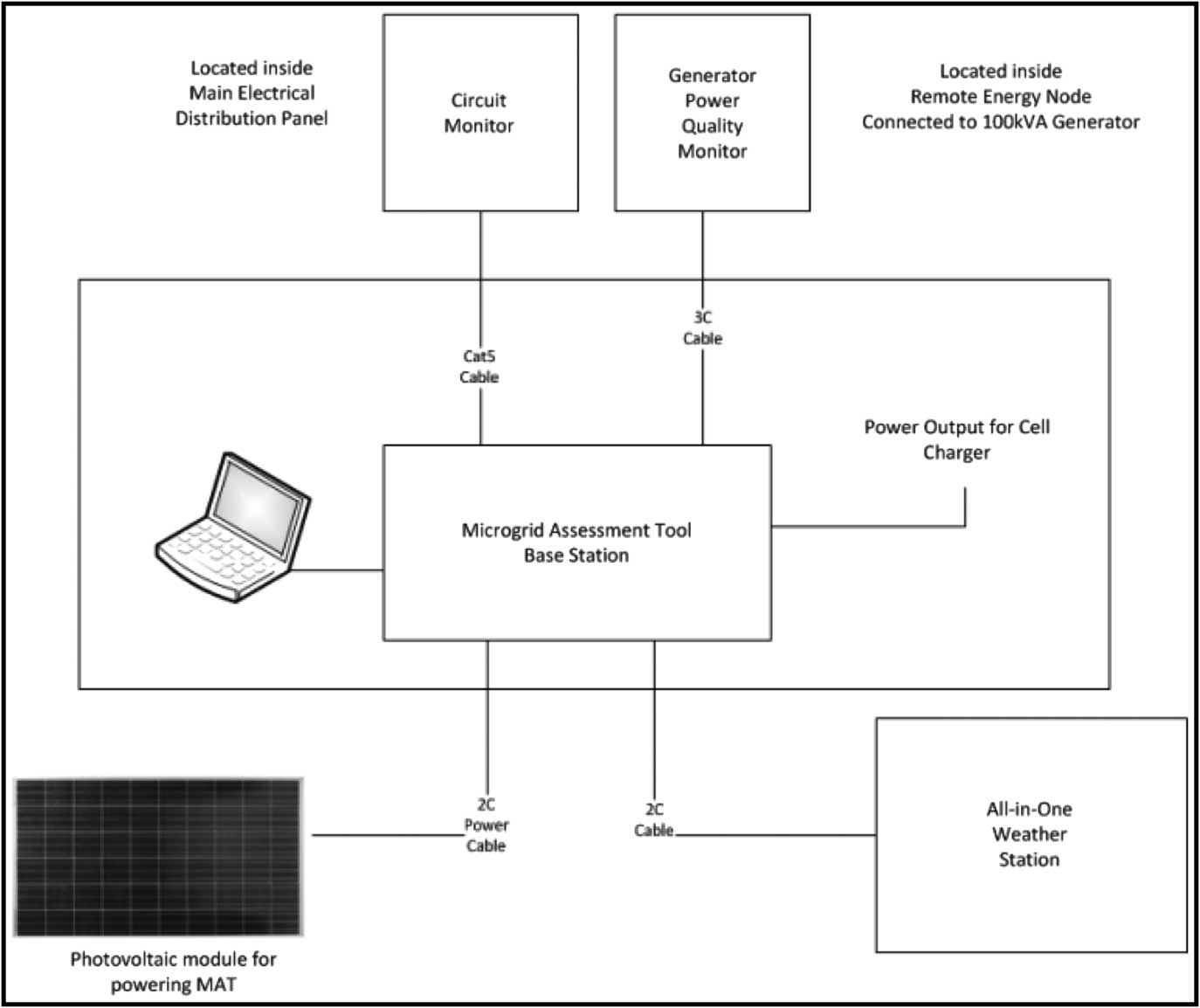
The electrical consumption and power quality of the MED-1 facility was completely unknown at the start of this project. A microgrid assessment tool (MAT; Microgrid Assessment Tool, MAT 0.1, Smart Resource Labs, Burlington, Vermont USA) was used to capture both granular load profiles and the power quality for use in the preliminary microgrid feasibility report. A one-line diagram of the MAT is shown below in Figure 1. The MAT comprised a base station (with an embedded datalogger, absorbed glass mat battery, and photovoltaic (PV) module for charging the battery); a circuit level monitor (with 12 current transformers and voltage sense for each of the three phases installed in the main load panel); a power quality meter (with three split-core current transformers for measuring generator output before any loads); and a weather station (that included a second-class pyranometer for measuring solar resource and an all-in-one weather transmitter that included wind speed, wind direction, precipitation, ambient temperature, relative humidity, and barometric pressure).
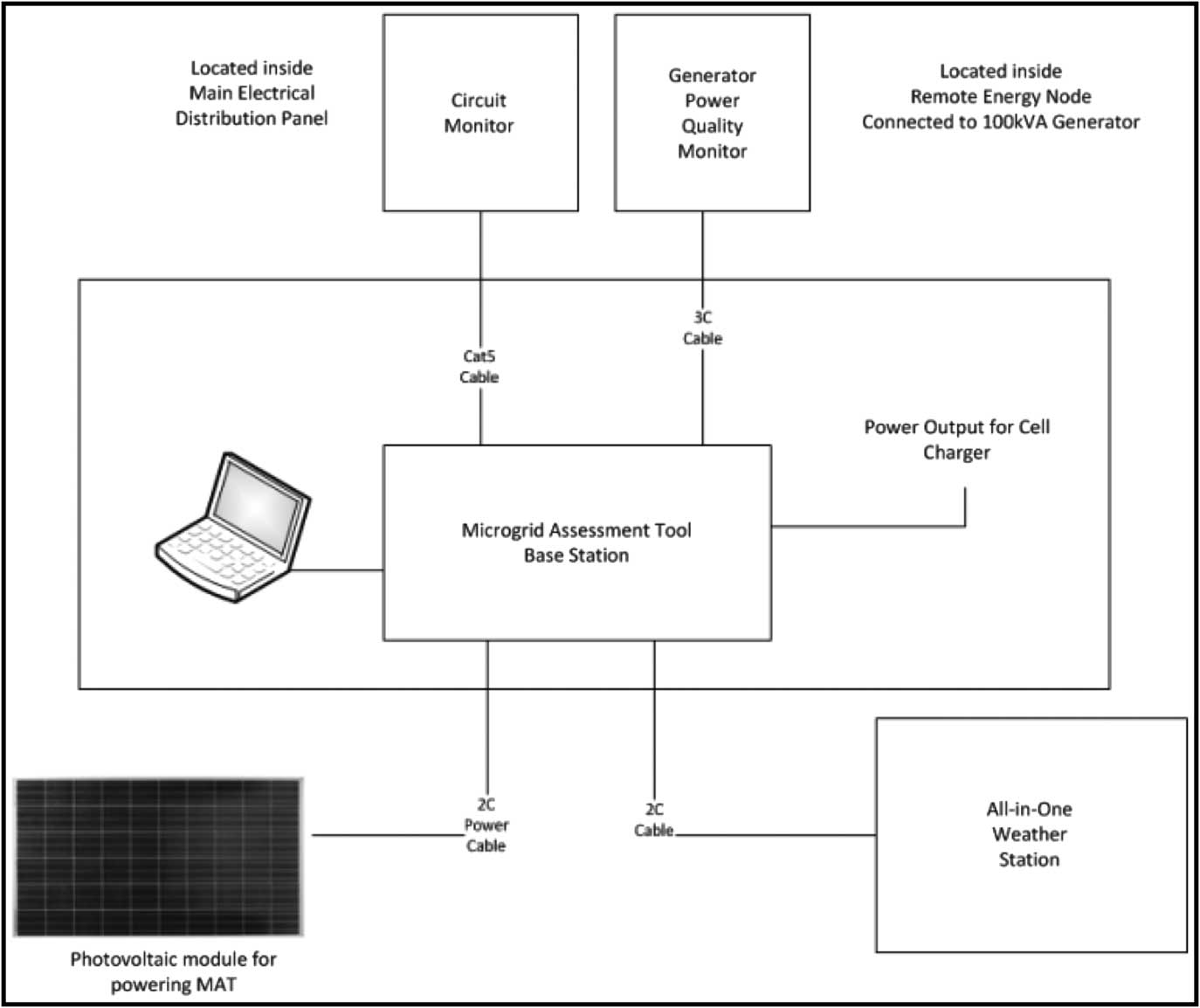
Figure 1 One-line Monitoring Diagram for Microgrid Assessment Tool Abbreviation: MAT, microgrid assessment tool.
Load profiles were measured twice with the MAT, first using the circuit monitor only at a preconvention training deployment at Lake Wylie, South Carolina (USA) in mid-August 2012, and then again later using the full MAT at a deployment at the DNC in Charlotte in early September of 2012. The circuit level monitor was used to measure the three input phases of the main load panel, six circuits that powered two 3-phase HVAC units, and three additional circuits for lights and plug loads.
Power System Modeling
Several scenarios were modeled using the HOMER hybrid power system optimization (HOMER 2 Software, HOMER Energy, Boulder, Colorado USA).Reference Bernal-Agustín and Dufo-López 4 The parameters considered were PV array size, power converter capacity, battery bank size, different load profile scenarios, generator minimum load ratio (MLR), efficiency, and solar resources available.
Photovoltaic arrays of 0 kW, 4.5 kW, 9 kW, and 13.5 kW were modeled for this preliminary study. It is estimated that 4.5 kW could be added to the top of each tractor trailer. Any additional PV generation would have to be added to another structure, via portable ground mount arrays assembled on site, or thin film modules integrated into tents or other structures.
Power converters are required when interfacing AC generation and loads, and direct current (DC) generation sources and battery storage. The diesel generators are AC generation, and PV arrays are DC generation. The power converter charges the batteries from the generator and inverts the DC power from the batteries for use in AC loads. Most medical and consumer electronic equipment deployed in MED-1 is designed to operate off an AC source.
The rate at which a diesel generator consumes fuel depends on the loading ratio. This loading ratio is defined as the load divided by the rated generator capacity. A fuel consumption chart published by Diesel Service & Supply Inc of Brighton, Colorado (USA) was used to estimate the generator fuel consumption of the MED-1 microgrid based on generator loading. The chart showed consumption rates for 25%, 50%, 75%, and full load as 2.6 gal/hr, 4.1 gal/hr, 5.8 gal/hr, and 7.4 gal/hour, respectively.
There are generator controls that set the minimum loading at which the fuel consumption remains constant to ensure full fuel combustion and reliable generator operation under low load conditions. This translates to a point on the fuel consumption curve which is referred to as the generator's MLR. Below the MLR, any decreases in the load no longer correspond to decreases in fuel consumption. Typically, this parameter is set to 30% in the HOMER model. This translates to 30 kVA for the generator attached to MED-1. So, in this case, loads of 10 kW, 20 kW, and 28 kW all consume the same amount of fuel as a 30 kW load.
The model is most sensitive to the generator MLR parameter because of the low loading of the generator relative to its rated capacity. The MLR for the generator was modeled at 30% and 15% to perform a sensitivity analysis.
Batteries were modeled to estimate fuel savings due to energy storage. The commonly used Surrette KSP25P battery (Rolls Battery Company, Springhill, Nova Scotia, Canada) was configured in 48 V strings. Since each battery is 4 V, there are 12 batteries in each serial string. Higher battery bank voltages could be used to save on conductor costs, but the modeling results would not change significantly. The 4KS25Ps are 1,900 Ah lead-acid batteries that weigh 315 pounds each.
A range of battery bank sizes were modeled for energy storage. Three battery bank sizes are reported for comparison—no battery bank, small bank, and large bank. The small bank consisted of a single battery string of 12 batteries with a total capacity of 90 kWh and was the smallest battery bank string at 48 V using the selected batteries. The large bank consisted of five strings with 60 batteries and a 450 kWh capacity and was the largest battery bank that could be supported using the weight capacity rating of a standard 20 foot trailer using an advanced battery technology. Advanced battery technologies, such as Lithium Ion batteries, decrease the weight of the battery bank by three times and the volume by nearly six times.
The effect of energy efficiency was modeled using the Efficiency Inputs parameter in the load profiles. Energy efficiency measures were assumed to be able to decrease total usage by 25%. This assumption was based on data collected from the EA. Described areas of potential improvement include a more efficient HVAC system, envelope sealing, light-emitting diode light bulbs, and some type of real-time display for showcasing electrical loads to inspire behavioral modifications.
The MED-1 unit typically operates in one of two modes: event support and disaster relief. The hospital is fully staffed for only a fraction of the day in the event support mode, typically during daytime hours. The load profile reflects this usage pattern with higher consumption during the day and lower consumption at night when the heating load is decreased by the sun not heating the exterior of the unit and a decreased internal heat loading by limited staff occupancy.
Results
Load Profiles
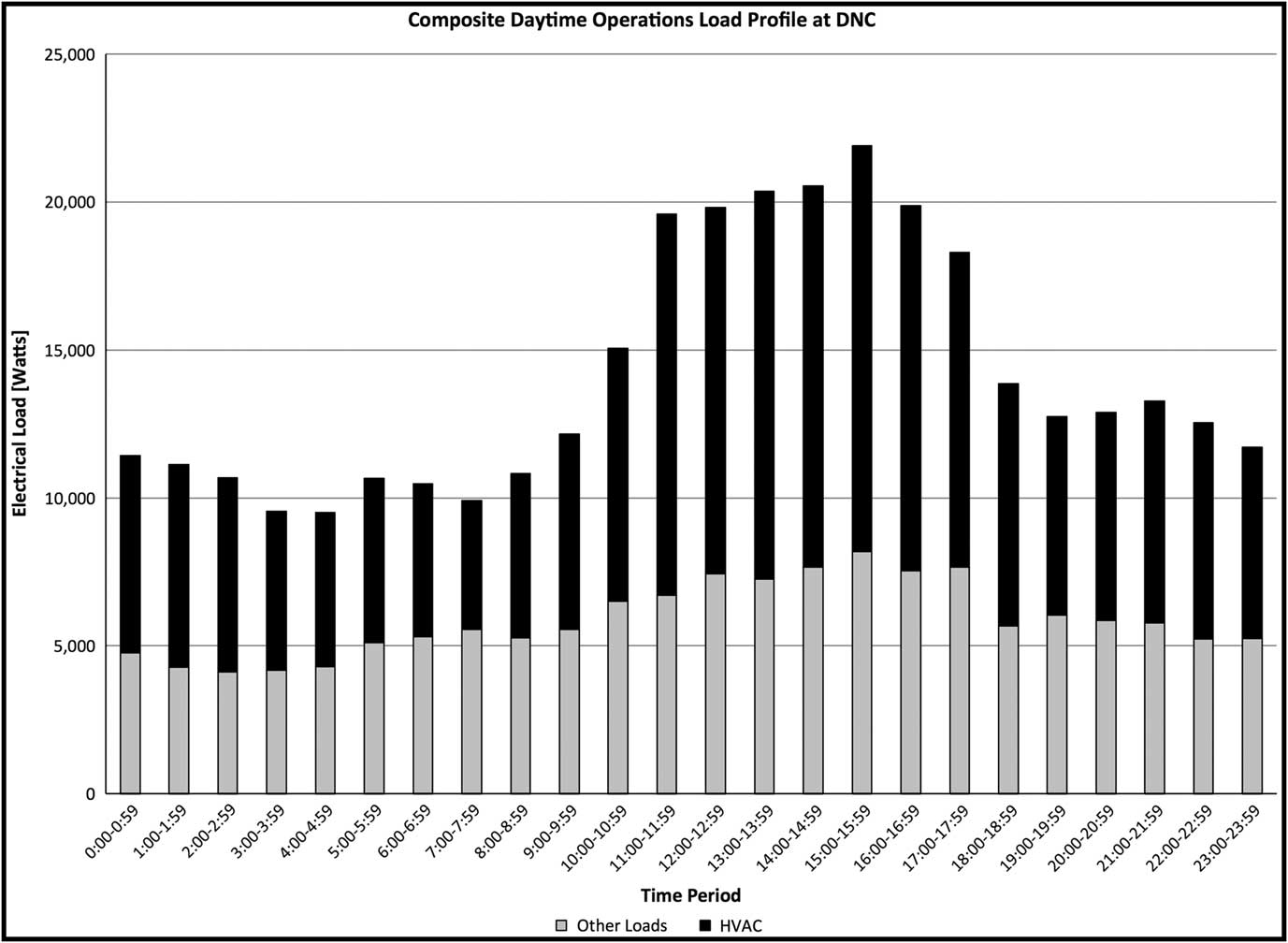
The load profiles from the training and DNC deployment were similar. The deployments had large electrical-usage patterns due to the heavy reliance on the HVAC system for air conditioning in hot and humid conditions. The measured composite convention load profile was the average of the measured load profiles over five days for actual daytime operations covering the DNC (Figure 2).
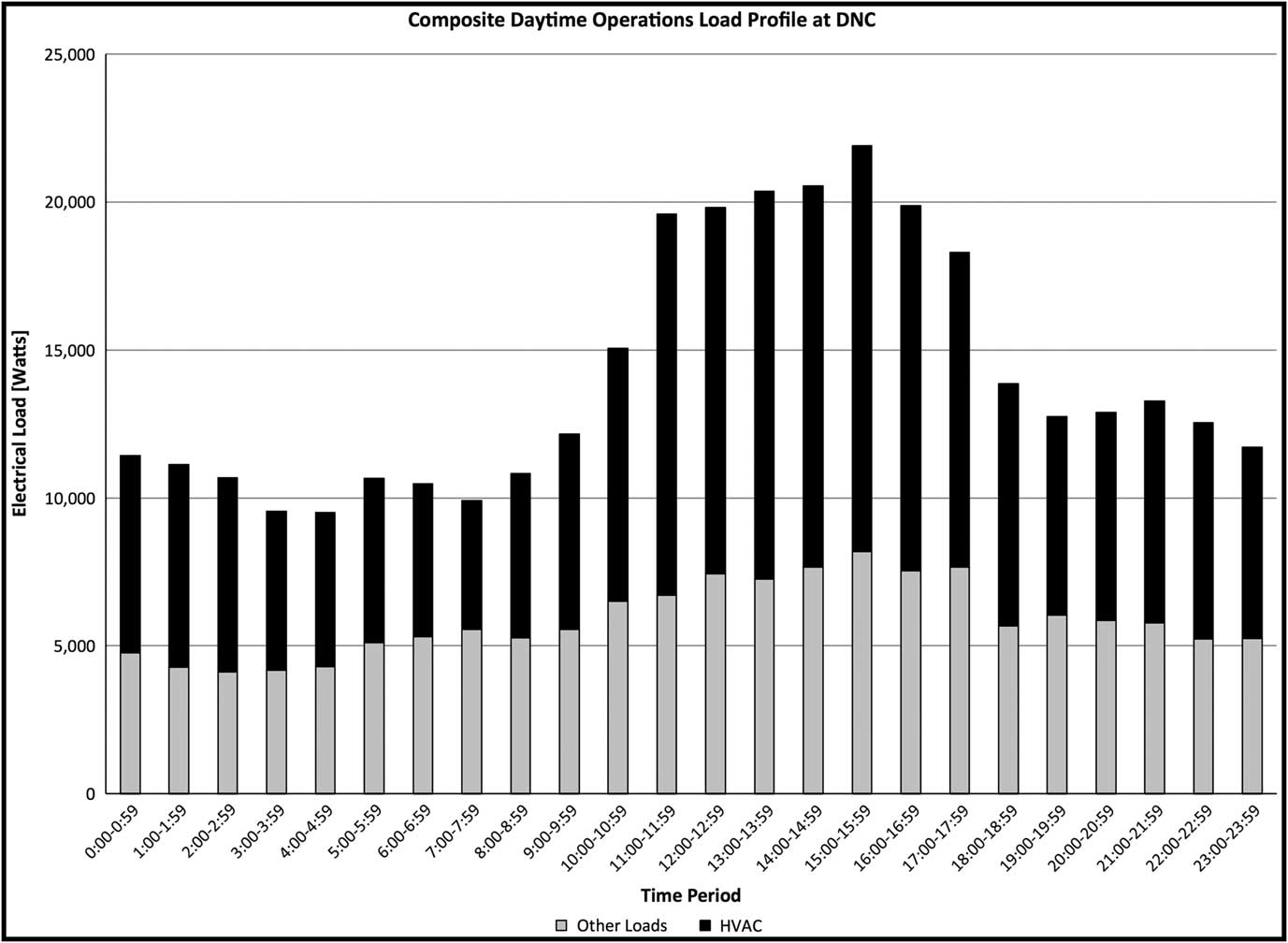
Figure 2 Composite Daytime Operations Load Profile at DNC Abbreviations: DNC, Democratic Nation Convention; HVAC, heating, ventilating, and air conditioning.
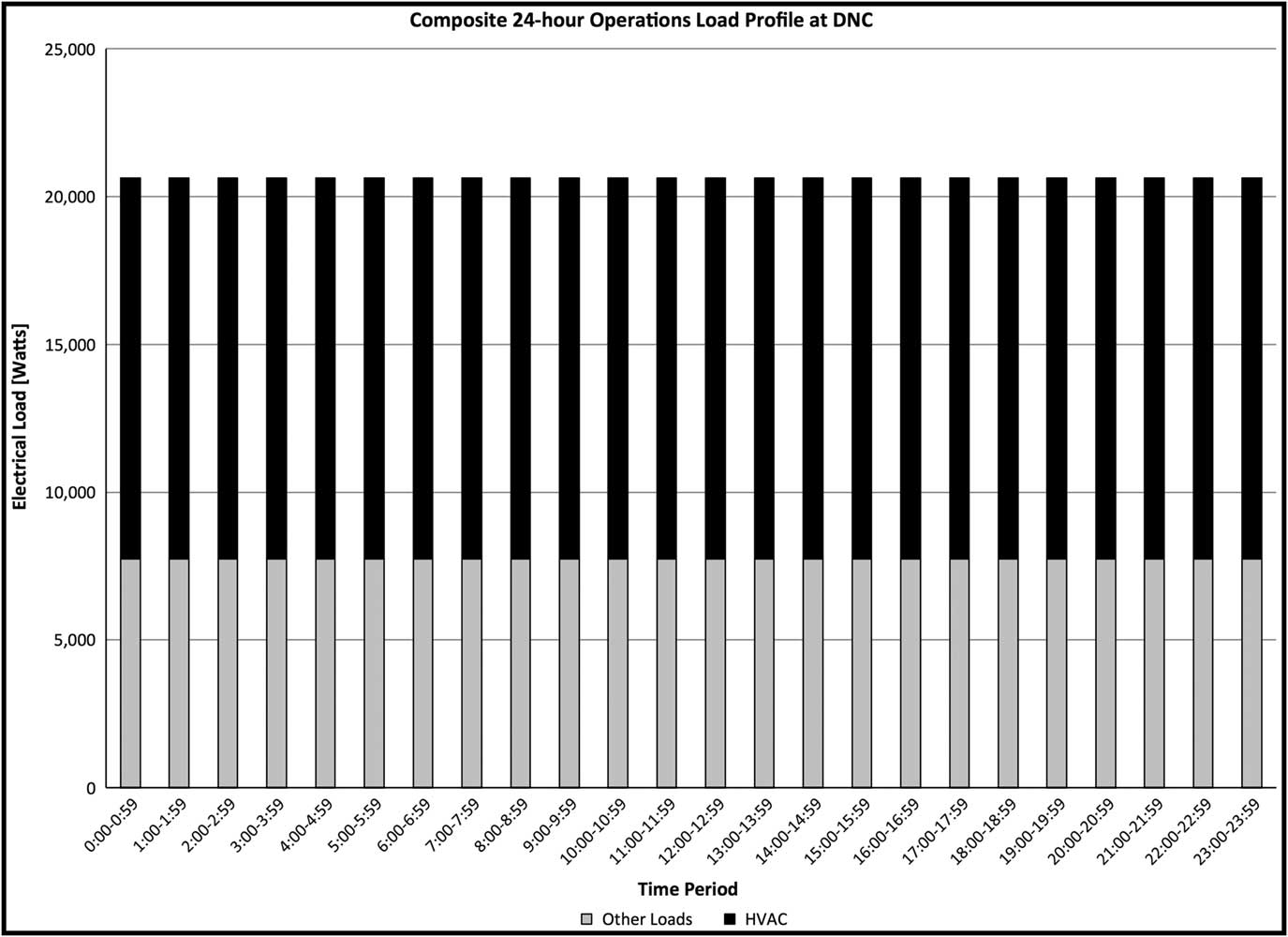
The HVAC loads were found to account for 57% of the load, on average, and varied between 44% and 66% with higher percentages between 11:00 am and 5:00 pm when outdoor temperatures were the highest. Most medical care was performed between 4:00 pm and 11:00 pm, emphasizing the fact that HVAC pulls far more power than the energy requirements of patient care. A second load model was generated, which was an extrapolated load profile where the highest hour load was used for each hour (Figure 3). This represented a worst-case scenario where consistent internal heat loading was generated by staff and patients due to 24-hour operations, and the exterior temperature was assumed to stay relatively constant due to humid conditions. Both were modeled to see how much of a difference the load profile would make with the 24-hour operations load profile representative of a worst case.

Figure 3 Composite 24-Hour Operations Load Profile at DNC Abbreviations: DNC, Democratic Nation Convention; HVAC, heating, ventilating, and air conditioning.
Model Scenarios
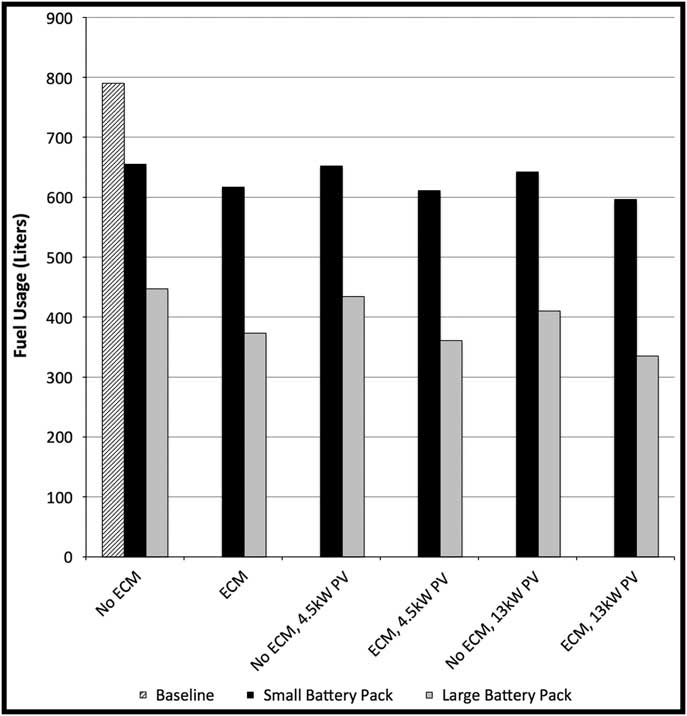
Based on modeling data, projections of generator run time and diesel fuel consumption were calculated. The effect of building improvements into the system, such as ECM, variably sized PV arrays, and battery packs, was also modeled to demonstrate the individual and cumulative benefits of these modifications as demonstrated in Figure 4.

Figure 4 Fuel Usage (liters) for a 3-day, Daytime-only Deployment Abbreviation: ECM, energy conservation measures.
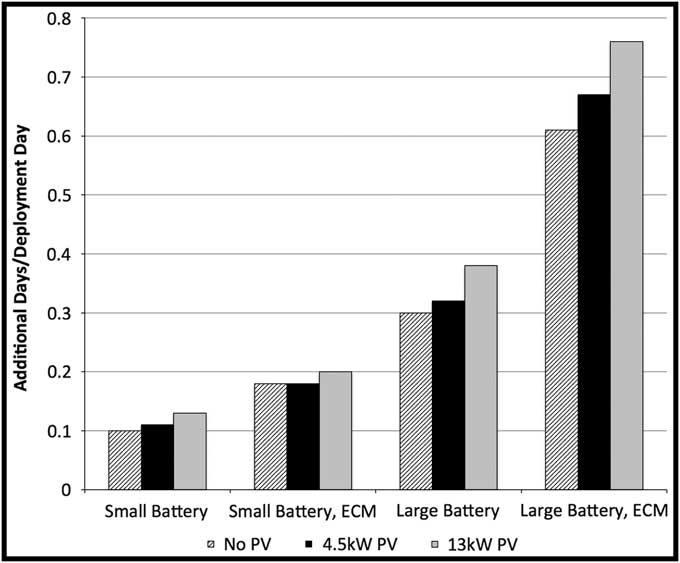
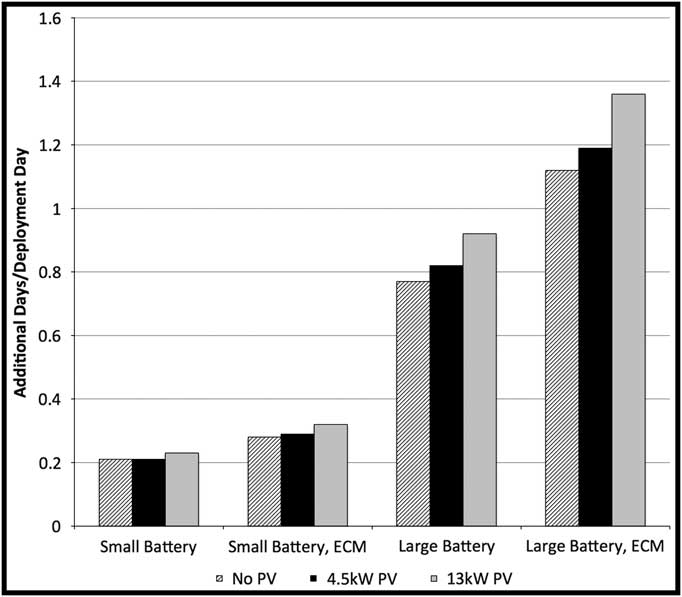
The results of these analyses were then used to calculate additional days of deployment that would be possible, assuming a fixed volume of fuel. Separate modeling was performed for both 24-hour operations and daytime-only use of MED-1. Different configurations, with and without ECM, and with various sized battery packs and PV arrays, were modeled. Using a 13 kW PV array in conjunction with a large battery pack and ECM, modeling showed that for 24-hour operations, energy savings would add an additional 0.76 days/day of deployment (Figure 5). A similar configuration would add an additional 1.36 days/day of deployment for a daytime-only operations deployment (Figure 6).
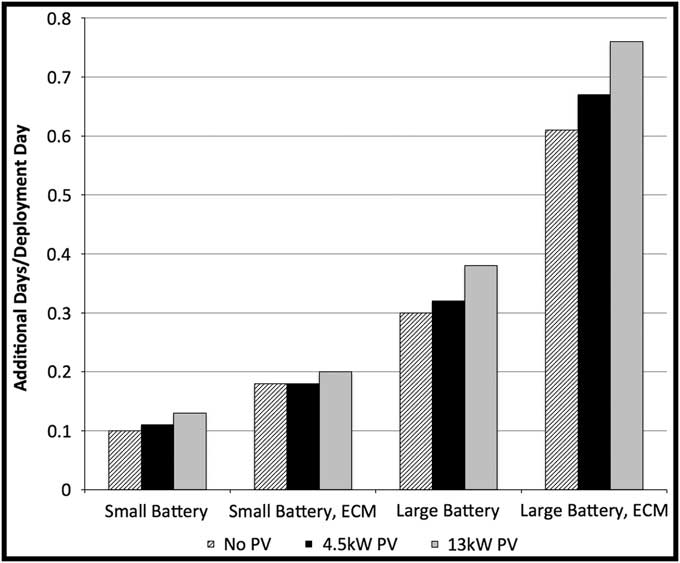
Figure 5 Modeling for Additional Days/Deployment Day – 24 hour Operations Abbreviations: ECM, energy conservation measures; PV, photovoltaic.

Figure 6 Modeling for Additional Days/Deployment Day – Daytime-only Operations Abbreviations: ECM, energy conservation measures; PV, photovoltaic.
Discussion
Large-scale disasters create immediate and ongoing challenges. The disaster cycle (planning, preparedness, response, and recovery) is a common framework for approaching emergency response to large-scale disruptive events. During the response and recovery phases, operations focus on discrete, but often overlapping, phases: actions during the ongoing event (eg, shelter, emergency care, and modified search and rescue), immediate response during hours 1-48 (eg, rapid needs assessment, gap analysis, and provision of emergency care), and acute response and recovery during days 2-14 (eg, provision of emergency care, reestablishment of local health care infrastructure, and transition to local resources).
Reliable energy is core to all phases of disaster response. Disruption of the power grid, loss of water and sewage systems, disabled communication infrastructure, and interruption of routine logistics impede disaster response and emergency medical care. Research has shown that all-cause mortality increases during severe power outages.Reference Anderson and Bell 5 , Reference Lin, Fletcher, Luo, Chinery and Hwang 6 Several recent natural disasters demonstrate the fragility of the infrastructure and the reliance on fossil fuels. On October 29th, 2012, during “Superstorm” Sandy, New York University's Langone Medical Center (New York USA) lost primary power and had inoperable back-up, roof-mounted, reserve generators. The Medical Center was forced to evacuate the entire hospital and transfer multiple critically ill patients on advanced life support. Two weeks after the storm, power remained unreliable or absent.Reference Powell, Hanfling and Gostin 7 , Reference Redlener and Reilly 8 The Federal Emergency Management Agency (FEMA) was able to provide reliable diesel fuel for federal response assets, distributing 313,000 gallons of gasoline and 157,000 gallons of diesel fuel in the first two weeks. However, civilian entities were less fortunate and individuals were often forced to wait in line for up to 16 hours for gasoline.Reference Wood 9
The tornado in Joplin, Missouri (USA) on May 22, 2011 is another recent example of the fragility of medical and community infrastructure. The tornado flattened a 1-mile by 6-mile path through downtown that affected the local hospital, nursing homes, schools, and houses. Nearly 35% of the population was without power. During the storm, an emergent surgical case had to be performed by flashlight.Reference Mathias 10 A deployable, integrated, microgrid system could circumvent the need for this austerity, allow critical operations to continue normally, and could dramatically improve community health.
In their recent article in the New England Journal of Medicine, Redlener and Reilly noted four critical concerns for response operations in the aftermath of a storm such as Sandy: (1) identification and treatment of casualties requiring urgent intervention; (2) attempt to minimize public health risks causes from flooding; (3) restoration of essential supply chains; and (4) access to care.Reference Redlener and Reilly 8 Provision of reliable power is critical to achieving all of the critical concerns, ranging from powering triage and staging tents to running water purification systems to shifting the logistics burden from providing fuel to providing medications or shelter.
In the aftermath of Katrina, the MED-1 team cared for over 7,500 patients and demonstrated its capabilities at providing access to care when existing health care institutions were suddenly offline. However, MED-1's technologically-advanced care capabilities were still reliant on diesel fuel resupply.Reference Blackwell and Bosse 3 The capacity of distributed generation through the implementation of a microgrid will allow MED-1 to provide immediate and sustained tertiary care during the ongoing and immediate post-disaster phase. Integrated into a larger response, MED-1 will require less fuel and less water, reducing the strain on external logistics and resupply efforts. This study demonstrates that the MED-1 microgrid energy-optimization capabilities would be invaluable in directly addressing a majority of the critical concerns detailed in the post Hurricane Katrina and post Hurricane Sandy after action reports.
Small-scale efforts have been made in the past to utilize solar power in disaster and emergency response. During the response to Hurricane Hugo (Southeastern USA) in 1989, small portable PV and battery systems were deployed in St. Croix (USA) to power 12 V DC fluorescent lights, radios, and shelter fans. In South Carolina, first responder agencies utilized trailer-mounted solar systems to power emergency public announcement systems. In 1992, the Florida Solar Energy Center (Cocoa, Florida USA) and SANDIA National Labs (New Mexico and California USA) deployed five PV systems that contained a 1 KWp PV array, battery bank, controller, and DC/AC converter to medical clinics in South Dade County, Florida.Reference Young 11 , 12 Despite significant improvements in the weight, durability and efficiency of various “renewable energy” sources, and advances in energy management technology, there exists no documented use of an integrated microgrid for powering advanced medical care post disaster.
The M1G study indicates a comprehensive energy strategy that incorporates ECM, power storage, and smart energy utilization through microgrid technology is required to provide advanced medical care in austere environments. The data indicate that MED-1's energy usage is very sensitive to the generator MLR. This sensitivity is most pronounced in the scenarios using the daytime-operations load profile. This makes sense as measured loads varied from under 10 kW to just over 20 kW each day. This means that only one-third of the fuel being consumed by the generator is used to power directly the loads during the low usage time periods, assuming a 30% MLR. A 30% MLR means that all loads below 30 kW consume the same amount of fuel when using a 100 kVA generator. This fraction of fuel used to directly power loads is increased around 66% when the MLR is assumed to be 15%. When battery storage is added to build out a microgrid, the excess electricity from the generator, (what is not used directly by power loads – HVAC, lighting, and equipment) is captured and stored in the batteries for later use. This storage allows the generator to turn off periodically and transition to the batteries to satisfy loads. In summary, the microgrid allows the generator to be used most efficiently.
The results also show that integrating a modern battery array into the microgrid has a larger impact for fuel savings than either energy conservation measures or adding a PV array. This observation makes sense since neither efficiency measures, nor PV generation, will cut fuel consumption if the generator loads are already below the MLR. The efficiency measures and PV array make a difference in fuel consumption when batteries are added. By lowering the net load, ECMs would increase the time the generator could be off due to decreased battery discharge rates. Photovoltaic would also increase generator downtime by providing an alternate source of energy to the batteries. A microgrid would be necessary to handle these alternate power routes, but would yield the distinct advantage of increasing operational time.
The M1G modeling shows that disaster-response operation times could be more than doubled before refueling is required through the incorporation of a 450 kWh battery bank and a 13.5 kW PV array. This capability will allow MED-1 to extend time on station while decreasing reliance on local (and perhaps scarce) resources. This independence will, in turn, lead to greater resilience and the possibility of operating in more austere environments. The ability to utilize distributive generation would introduce greater flexibility into the system as it would permit the incorporation of solar (as modeled here), wind, biodiesel, or yet undiscovered fuel sources. Having such a robust and efficient generation system could even allow MED-1 to act as a short-term power utility (ie, power plant) for other operations in the immediate vicinity. Finally, the realization of this system would demonstrate MED-1 to be both a model for “green energy” practices and an ongoing prototype of innovation in disaster operations.
Limitations
The primary limitation of the study is that the data provided are based on modeling, not real-world testing. Despite this, the data produced by this study suggest that a microgrid could have significant benefit in increasing autonomy and resiliency during disaster operations. A system would have to be built to allow actual testing to occur, and fuel usage could be compared to the baseline data collected for this study to demonstrate an actual savings. Furthermore, to date, there has been limited use of microgrids in mobile applications. The installation of a microgrid would add to the weight of MED-1, and the battery packs could necessitate an additional vehicle to transport this load. The additional equipment could add to the logistical challenges of deployment; however, the microgrid itself is automated, and so once installed monitoring could easily be managed by personnel already responsible for the operation of the generator.
Conclusion
The improved energy efficiency of MED-1 that couples EMC and microgrid technology has clear operational, financial, and environmental benefits. A fully-integrated energy management system will make MED-1 the most flexible, mobile, advanced disaster medical facility in the nation. It will be more independent and resilient while being cheaper and cleaner to operate. The MED-1 microgrid can also serve as proof of concept for deployment of mobile microgrids in other austere disaster and medical operations.