



Introduction
Nouvelle-Aquitaine is the largest administrative region in France and is located in the southwest of the country. Created in the 2014 reform of French Regions, with the merging of the regions Aquitaine, Limousin, and Poitou-Charentes,1 it covers 84,061 km2 with a population of approximately 5,800,000 inhabitants. It comprises 12 départments (sub-regional level administrative districts): Charente, Charente-Maritime, Corrèze, Creuse, Dordogne, Gironde, Landes, Lot-et-Garonne, Pyrénées-Atlantiques, Deux-Sèvres, Vienne, and Haute-Vienne.
Nouvelle-Aquitaine it is the largest agricultural region in Europe and the number one French region for tourism. The annual summer increase in its population (in particular along the Atlantic Ocean shores) impacts epidemiological surveillance. Furthermore, the Atlantic shore climate favors health risks from heatwaves and the ocean (eg, drowning, Physalia physalis, and trauma).
The syndromic surveillance system SurSaUD, developed by Santé publique France (SpF; the French National Public Health Agency; Saint-Maurice, Paris, France), has been active since July 2004. It is based on daily data sourced from: hospital emergency departments (OSCOUR ED network); emergency general practitioners (GPs; SOS Médecins network); the national statistics bureau (Insee) for crude mortality data; and electronic death certification (CepiDC), which includes data on causes of death.Reference Caserio-Schönemann, Bousquet, Fouillet and Henry2 SurSaUD aims at ensuring early detection and situational awareness of public health issues from known or unexpected threats.
In Nouvelle-Aquitaine, the SpF regional office is in charge of coordinating public health surveillance in the region. The objectives of this article are to describe the SOS Médecins network in Nouvelle-Aquitaine, as well as its contribution to surveillance in terms of assessing the health impact of events.
Method
Collected Data and Processing
With regard to SOS Médecins, data from all emergency GP medical consultations and home visits, logged during the previous 24-hour period, are recorded on a secure national database server that can be monitored by SpF regional offices. The Nouvelle-Aquitaine regional SpF office, in collaboration with all five local SOS Médecins associations, is in charge of coordinating public health surveillance in the region.
Data collected include: the date of consultation or home visit, residential postal code, age, sex, patient’s health complaints, and medical diagnosis. Medical information, such as provisional medical diagnosis, which is coded according to the specific thesaurus for SOS Médecins, is routinely monitored through different syndromic indicators.
Data Analysis
The huge amount of collected data is first organized by aggregating the individual data by age group, day or week, geographical area, and syndromes defined by one or several medical diagnoses or chief complaints.
Quantitative analysis of health indicators is performed by studying global activity with a description of the total number of visits (%) along with specific analyses based on syndrome groups, particular age group, and specific medical diagnoses.
The SpF regional office uses statistical methods (average/fluctuating median, control maps, Serfling methods) for certain syndromic groups of data to make a homogeneous territorial analysis. The analysis of control panels (on daily or weekly datasets) is performed twice a week. When an (un)expected event or unusual variation is signaled, the regional office contacts the sources of these alarm data and examines their analysis of the situation so as to validate or invalidate the signal. In the former case, the regional office will then launch an investigation.
Feedback
Surveillance results are published in the regional office’s epidemiological updates. The frequency depends on the current health context. During epidemic periods, results are published weekly. Annual reports are created at the behest of the local SOS Médecins networks. When health events occur, an investigation note is transmitted to the SpF at the national level and to relevant partners.
Results
Description of the Network
In Nouvelle-Aquitaine, the SOS Médecins network consists of five local organizations spread across the region (Figure 1). The network was implemented in 2006 through a collaboration between SOS Bordeaux and SOS Limoges. SOS Pau (2007), SOS Cote Basque Bayonne (BAB 2008), and SOS La Rochelle (2010) subsequently joined. The network comprises 146 GPs operating in 160 townships, for a total of 1,000 interventions a day in a population of 1,509,513 inhabitants (data from 2018).
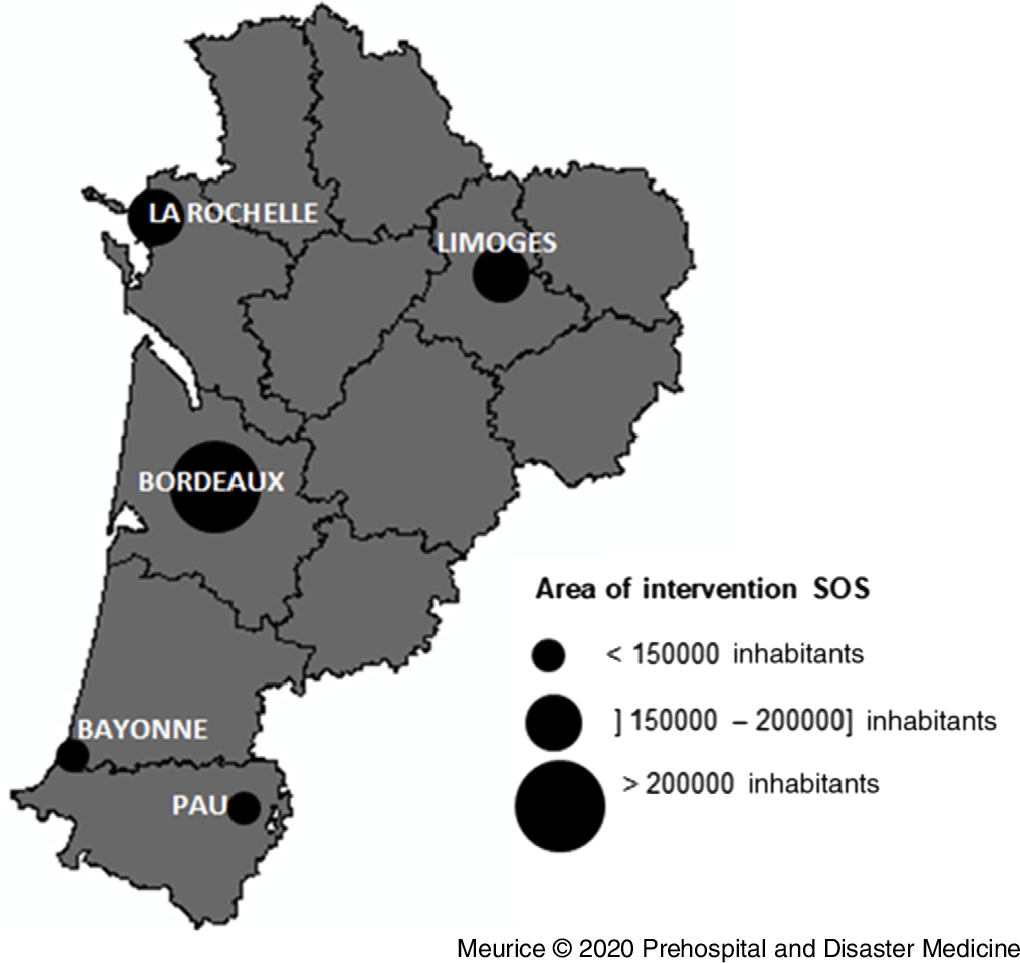
Figure 1. Number of Inhabitants by Area, SOS Médecins Network 2017, Nouvelle-Aquitaine.
The SOS Médecins network activity has greatly increased in recent years, from approximately 200,000 annual visits/consultations in 2007 to 480,000 in 2017 (Figure 2). During that period, global activity varied according to the day of the week and the season, as the number of visits/consultations increased during weekends and in the winter.

Figure 2. Monthly Number of Visits/Consultations, SOS Médecins Network 2006 – 2017, Nouvelle-Aquitaine.
Of the 480,000 consultations in 2017, approximately 30% and 16% concerned children under 15 years old and persons over 65 years old, respectively. The 10 most frequent pathologies are displayed in Figure 3: approximately 25% of the network’s activity involved respiratory pathologies.

Figure 3. Most Frequent Diagnosis, All Age Groups, SOS Médecins Network 2017, Nouvelle-Aquitaine.
Surveillance of Seasonal Outbreaks of Influenza-Like Illnesses
The monitoring of syndrome groups enables the surveillance of seasonal outbreaks such as influenza-like illnesses. Epidemic periods are clearly identified on curves and reach high peaks during the winter seasons.
Figure 4 shows the weekly activity for influenza-like illnesses in Nouvelle-Aquitaine for three different seasons. During the 2017-2018 epidemic, almost 21,000 visits/consultations for an influenza-like illness were reported during the epidemiological surveillance period (S40-2017 to S15-2018), which corresponds to seven percent of the total activity of all five local SOS Médecins units.

Figure 4. Weekly Number and Weekly Percentage of Visits/Consultations for Influenza-Like Illnesses, SOS Médecins Network 2016 – 2018, Nouvelle-Aquitaine.
Surveillance of Unusual Events such as the Early Heatwave in June 2017
In June 2017, a significant heatwave occurred in France, and the warning level of the Heat Watch Warning systemReference Laaidi, Ung, Wagner, Beaudeau and Pascal3 was activated from June 17-25. In the Nouvelle-Aquitaine region, the warning level was activated from June 17-23. All-cause and heat-related cause GP visits/consultations are individually monitored during heatwaves. Heat-related causes include heat stroke and dehydration. However, these pathologies only represent a small portion of the potential health impact during heatwaves.
During the June 2017 episode, daily monitoring showed a sharp increase in the number of GP visits/consultations for heat syndromes. More specifically, 235 GP visits/consultations were observed for diagnoses related to heat, representing approximately three percent of total regional activity. Adults under 75 years of age (47%) and children (32%) were mostly represented (Figure 5). During the heatwave outbreak, two episodes of physical discomfort (fainting) were reported.

Figure 5. Daily Number of Visits/Consultations for Heat-Related Syndromes, SOS Médecins Network May 15, 2017 – July 02, 2017, Nouvelle-Aquitaine Region.
Impact Assessment
One of the aims of SurSaUD, and therefore of SOS Médecins data, is to evaluate the impact of known and (un)expected phenomena on emergency care uptake and on mortality. This has been broadly achieved during recent years; for example, in the case of the pandemics of A(H1N1) influenza virus in 2009, extreme climate events (heatwaves),Reference Caserio Schönemann, Fouillet and Ung4 industrial and natural disasters,Reference Vilain, Pagès and Combes5 unexpected events such as the terrorist attacks in Paris on November 13, 2015,Reference Vandentorren, Paty, Baffert, Chansard and Caserio-Schönemann6 and popular mass gatherings such as the EURO soccer championship in 2016.Reference Fougère, Caserio-Schönemann and Daoudi7 In the Nouvelle-Aquitaine region, SOS Médecins data were used during all these events to measure the health impact (Table 1).
Table 1. List of Events for which SOS Data were Used in Nouvelle-Aquitaine

Discussion
Continuous care provided by the SOS Médecins network ensures that epidemiological information is available at night, on weekends, on public holidays, and during school holidays. In Nouvelle Aquitaine, the extent of the network and its wide-spread use confirm its importance as a source of essential data (nearly 480,000 consultations per year), particularly for the monitoring of pathologies in children and young adults in the urban and suburban areas.
The main features of this system are that: (1) It is responsive, with automatic near real-time data transmission. Consequently, health authorities can use it to mobilize rapid response (eg, the control of medical stocks and the coordination of the different local health authorities when wide-spread epidemics occur). And (2) It complements other surveillance sources: hospital emergency unit and mortality data reflect only the most serious forms of disease, while SOS Médecins data guarantees access to care for a large number of diseases not requiring hospitalization.
For a large number of situations (eg, festivals and heatwaves), health authorities request data from SOS Médecins on the number of visits/consultations in order to inform decision making on situation management. Through SurSaUD, SpF must communicate these data as soon as possible, even to indicate that nothing serious is happening and thereby reassure the population.
Limitations
Regarding limitations, differences in coding practices between GPs are possible, and it would be interesting to evaluate the coding practices of pathologies in all of the French SOS networks. In addition, the representativeness of SOS Médecins network may be questioned because only urban territories are covered.
In spite of these limitations, the network’s contribution to epidemiology has been demonstrated several times, especially regarding the permanent surveillance of influenza-like illnesses and bronchitis in order to quickly inform health professionals of a current epidemic. In this article, it can be seen that while heatwaves usually affect older people, the increasing frequency of these episodes is also affecting younger populations, and this underlines the importance of prevention in this population. During the 2017 heatwave, the SpF regional office in Nouvelle-Aquitaine was able to quickly inform the national education authority, which in turn implemented preventive measures in schools (eg, cancelling sports competitions at the end of the school year).
Since the integration of SOS Médecins data into the SurSaUD system, several national and regional studies have benefited from these data. Over the entire Nouvelle Aquitaine region, these data have been used in epidemiological investigations (gastroenteritis, foodborne infections, and clustered cases of measles) and during the monitoring of air pollution epidemics, as well as major climatic events (ie, storms and extreme cold).
The SurSaUD system aims to ensure early detection and situational awareness of known and unexpected threats to public health. For example, syndromic surveillance with SOS Médecins network data can be used for the early detection of abnormal health-related events or to quantify the health effects of major events such as terrorist attacks. One such case is the increase in psychological effects reported by the network during the week following the terrorist attack in Paris in November 2015, even before the confirmation of diagnoses.Reference Vandentorren, Paty, Baffert, Chansard and Caserio-Schönemann6 Today, the deployment of circumstantial coding (pathology X for consultations related to an event) in the case of unusual or unexpected events is one of the working areas in which the five local SOS Médecins network associations in the Nouvelle-Aquitaine region are involved.
To date, few studies have examined the SOS Médecins network. An evaluation of the SurSaUD system was performed in 2008 in Bordeaux and showed the efficiency, the simplicity, and the acceptability of the system.Reference Flamand, Larrieu, Couvy, Jouves, Josseran and Filleul8 In addition, a study on influenzaReference Pelat, Bonmarin and Ruello9 showed that the number of influenza-like illness cases reported by GPs in the network was twice that reported by hospital emergency departments and 10-times that reported by GPs from another French GP network called Sentinelles.
Other SOS Médecins networks have been created in Belgium, Greece, and Senegal. Physicians from London, New York, and Rome have used the same modus operandi. However, France is the only country where the network provides near real-time information for syndromic surveillance.
Conclusion
The SOS Médecins network is one of the major tools used for health surveillance in the Nouvelle-Aquitaine region in France and complements data from other surveillance sources.
Acknowledgements
The authors thank all the physicians of the SOS Médecins network in Nouvelle-Aquitaine for their collaboration in providing data. Thanks also to SOS Médecins France and to the “DATA SurSaUD” department, which manages all SurSaUD data.
Conflicts of interest
none






