Introduction
Extreme weather events (EWEs) are caused by oceanic and atmospheric hazards that are influenced by the global climate. Warming of the global climate is predicted to increase the number of EWEs (ie, disasters caused by climatological, hydrological, and meteorological hazards).1,2
Most disease related to EWE disasters occurs as a result of traumatic and/or psychological injury sustained through: (1) exposure to environmental hazards such as water, wind, fire, smoke, debris, or heat; or (2) an absence of a life-sustaining requirement (eg, air, food, and water). There are also indirect health effects that occur secondary to displacement and loss of health-sustaining services that (under certain circumstances) can result in outbreaks of infectious disease and/or exacerbations of chronic disease.Reference Keim3-Reference Keim and Frumkin5
These events are predicted to cause catastrophic health consequences for millions of people world-wide. The world’s poor are disproportionately affected by all disasters. Thus, the most vulnerable and marginalized in all societies are expected to bear the highest health burden.Reference Brouewer, Akter and Brander6 This manuscript summarizes the 50-year review of global disaster data to characterize the impact of seven extreme weather hazards on the health of disaster-affected populations.
Methods
A historical database including seven extreme weather hazards (ie, cyclones, droughts, floods, heatwaves, landslides, cold weather, and storms) occurring globally from 1969 through 2008 was created from the Emergency Events Database (EM-DAT), an internationally accepted source of aggregate disaster data.7 Being a global database on natural and technological disasters, EM-DAT contains essential core data on the occurrence and effects of more than 21,000 disasters in the world, from 1900 to present. It is maintained by the Center for Research on the Epidemiology of Disasters (CRED) at the Catholic University of Louvain, School of Public Health, in Brussels, Belgium. Established in 1973, CRED has collaborative status with the United Nations (UN) Department of Humanitarian Affairs (Geneva, Switzerland), the European Union Humanitarian Office (Brussels, Belgium), the International Federation of the Red Cross and Red Crescent (Geneva, Switzerland), the US Office of Foreign Disaster Assistance (Washington, DC USA), as well as with non-governmental agencies such as the International Committee of the Red Cross (Geneva, Switzerland).7
The EM-DAT database is comprised of information from various sources, including UN agencies, non-governmental organizations, insurance companies, research institutes, and press agencies. Priority is given to data from UN agencies, governments, and the International Federation of Red Cross and Red Crescent Societies. This prioritization is not only a reflection of the quality or value of the data, it also reflects the fact that most reporting sources do not cover all disasters or have political limitations that could affect the figures. The entries are constantly reviewed for inconsistencies, redundancy, and incompleteness, and CRED consolidates and updates data daily. A further check is made at monthly intervals, and revisions are made at the end of each calendar year.7
For a disaster to be entered into the EM-DAT database, at least one of the following criteria must be fulfilled: (1) ten (10) or more people reported killed; (2) one hundred (100) or more people reported affected; (3) declaration of a state of emergency; or (4) call for international assistance. Deaths are defined as the “number of people who lost their life because the event happened.” Total deaths are the “sum of deaths and missing.” The EM-DAT definition of “injury” is actually comprehensive of all categories of disease, not merely injury: “persons suffering from physical injuries, trauma, or an illness requiring immediate medical assistance as a direct result of a disaster.” Also, EM-DAT defines “affected” as those persons “requiring immediate assistance during a period of emergency… requiring basic survival needs such as food, water, shelter, sanitation, and immediate medical assistance.”7
The annual incidence of disasters related to EWEs was calculated over a 50-year period (1969-2018) for all seven hazards. A regression analysis was then performed to characterize any trends involving the annual global rates of EWE-related hazard incidence, exposure, morbidity incidence, and mortality incidence.
Linear regression and analysis of variance (ANOVA) calculations were performed to evaluate the association between the dependent variable of exposure rate (ie, global number of persons affected per 100,000 population) and the independent variable of hazard incidence rate (global number of EWEs per year).
Separate multiple regression and ANOVA calculations were also performed to evaluate the association between individual dependent variables of morbidity and mortality incidence rates and the independent variables of both exposure rate and EWE hazard incidence rate.
Results
According to this review, during the 50-year-long period (1969-2018), 10,009 EWE disasters caused over two million (2,037,415) deaths and nearly four million (3,998,466) cases of disease. Over seven billion (7,350,276,440) persons required immediate assistance during a period of emergency.
Global Incidence of EWE Disasters
Floods (47%) and storms (30%) were the most common EWE disasters to occur during the 50-year period studied, followed by landslides (7%), drought (6%), cold (4%), wildfire (4%), and heat wave (2%). Figure 1 depicts a review of the 50-year trend for the relative contribution from individual hazards to the total annual incidence of EWE disasters over time. This graph highlights the scale and consistency of flood and storm incidence over time as the most common EWE disasters world-wide.

Figure 1. Relative Contribution of Individual Hazards to the Total Annual Incidence of EWE-Related Disasters (1969-2018).
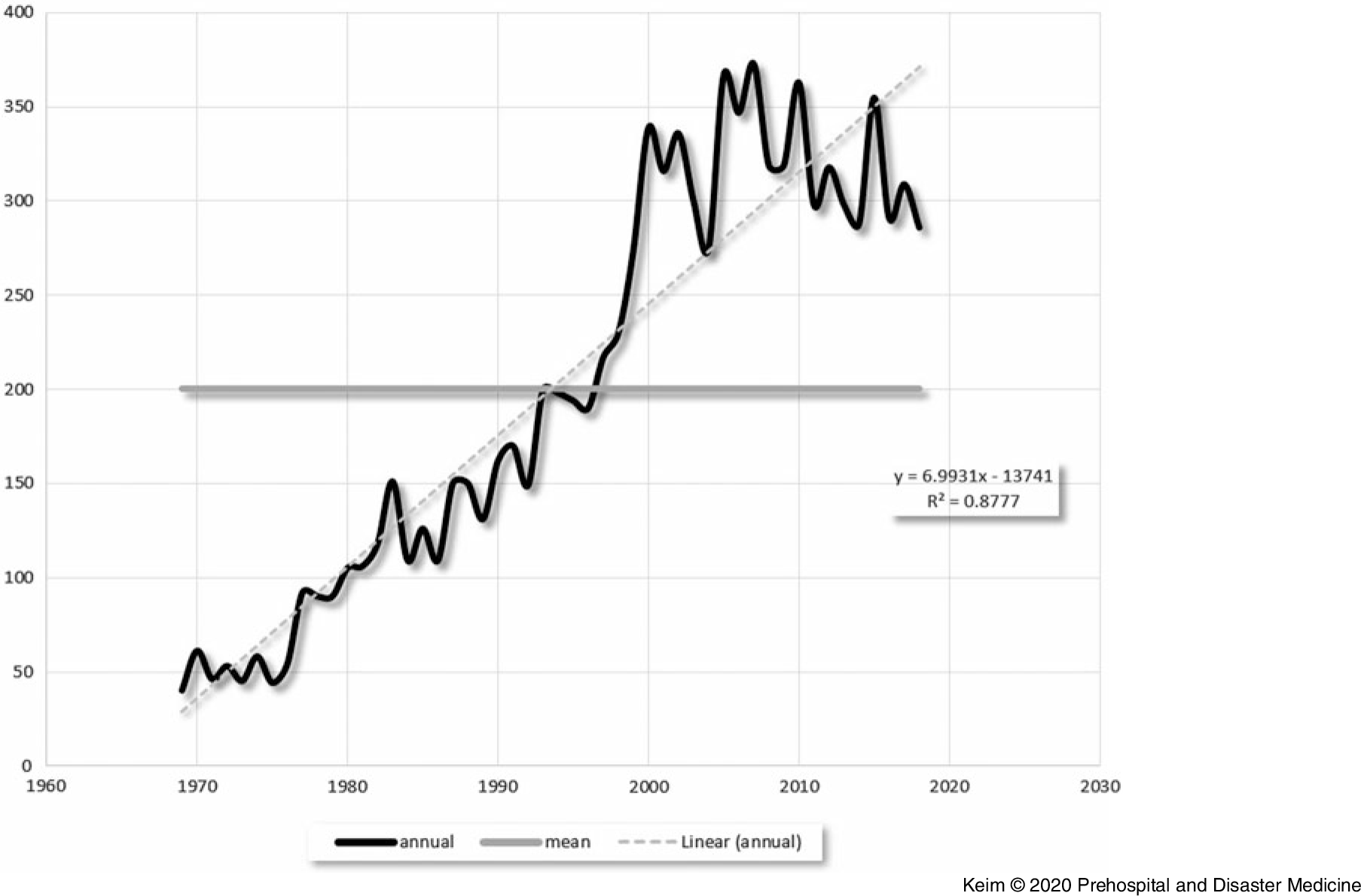
Calculation of linear regression for EWE disaster incidence revealed an upward trend over time (with a model equation of y = 6.9931x – 13741 and R2 = 0.88; Figure 2).

Figure 2. Global Incidence of EWE Disasters (1969-2018).
Regression analysis of the other factors studied revealed the following values: exposure rate (R2 = 0.07); incidence of mortality (R2 = 0.07); and incidence of morbidity (R2 = 0.02). In 1969, there were 40 EWE disasters on record. In 2018, there were 286. The mean annual incidence for EWE disasters during this 50-year period was 200.
Linear regression and ANOVA calculations performed to evaluate the association between the dependent variable of hazard incidence rate and the independent variable of exposure rate resulted in an R2 = 0.12; F-significance = 0.01; and P value = .01.
Global Mortality from EWE Disasters
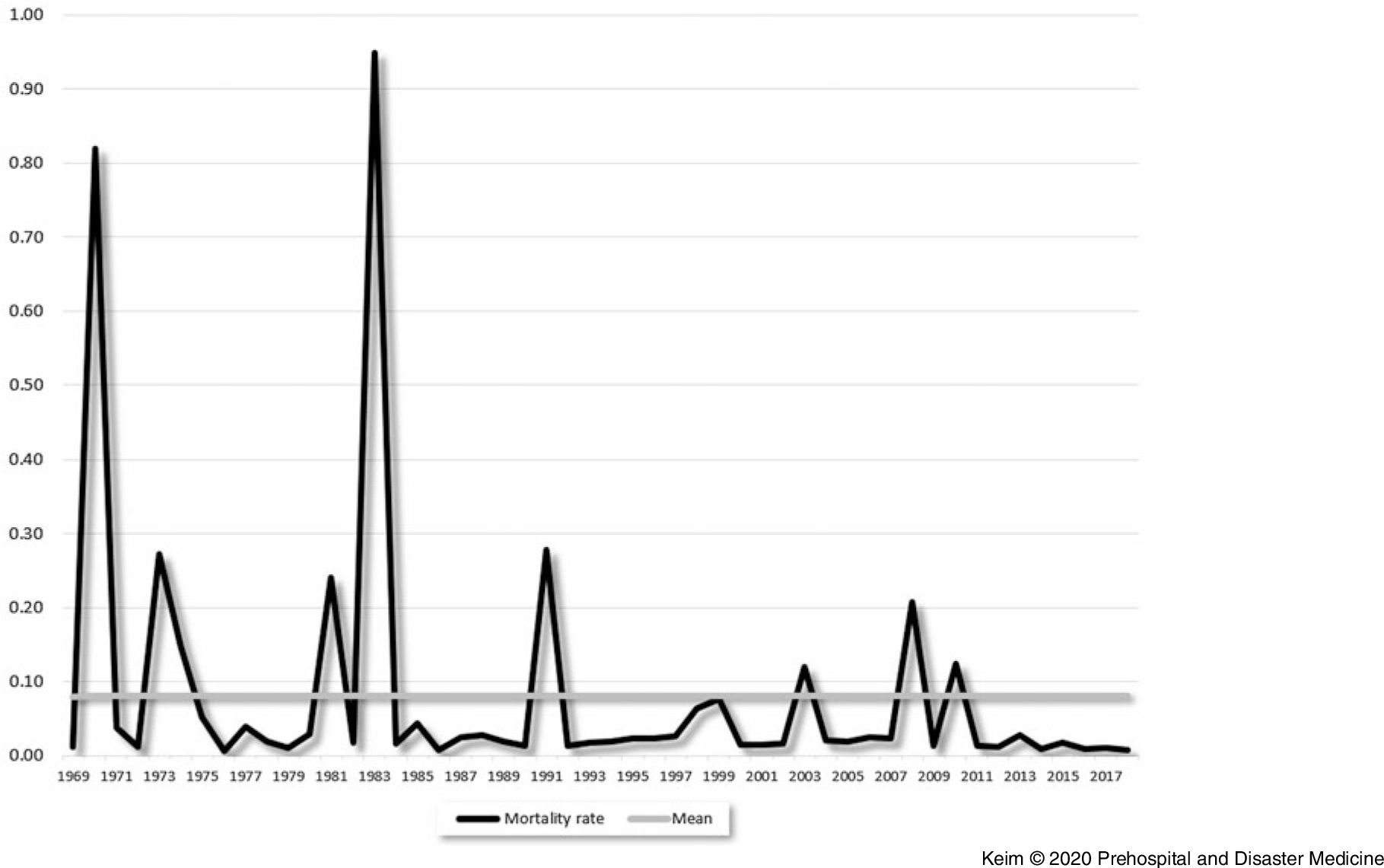
Most (89%) global mortality during this period was caused by storms (39%), droughts (34%), and floods (16%); followed by heat wave (8%), landslides (2%), cold (1%), and wildfire (<1%). The global crude death rate for EWE-related mortality during this period was 0.08 deaths per 100,000 persons. Figure 3 represents the annual global incidence rate of mortality (deaths per 100,000 persons) attributable to EWE disasters over a 50-year period. There are nine notable peaks that rise above the mean. Seven of the nine spikes were mainly attributable to only one hazard per year: storms (3); drought (3); and heat (1). During the other two years (1999 and 2010), increases were caused mainly by two hazards per year (floods and storms; and heat and drought), respectively.

Figure 3. Annual Global Incidence Rate of Mortality due to EWE Disasters (1969-2018).
Results of multiple regression and ANOVA calculations performed to evaluate the association between the dependent variable of mortality incidence rate were as follows for the independent variables of: exposure rate (R2 = 0.04; F significance = 0.35; and P value = .95); as well as for hazard incidence (R2 = 0.04; F significance = 0.35; and P value = .18).
Global Morbidity from EWE Disasters
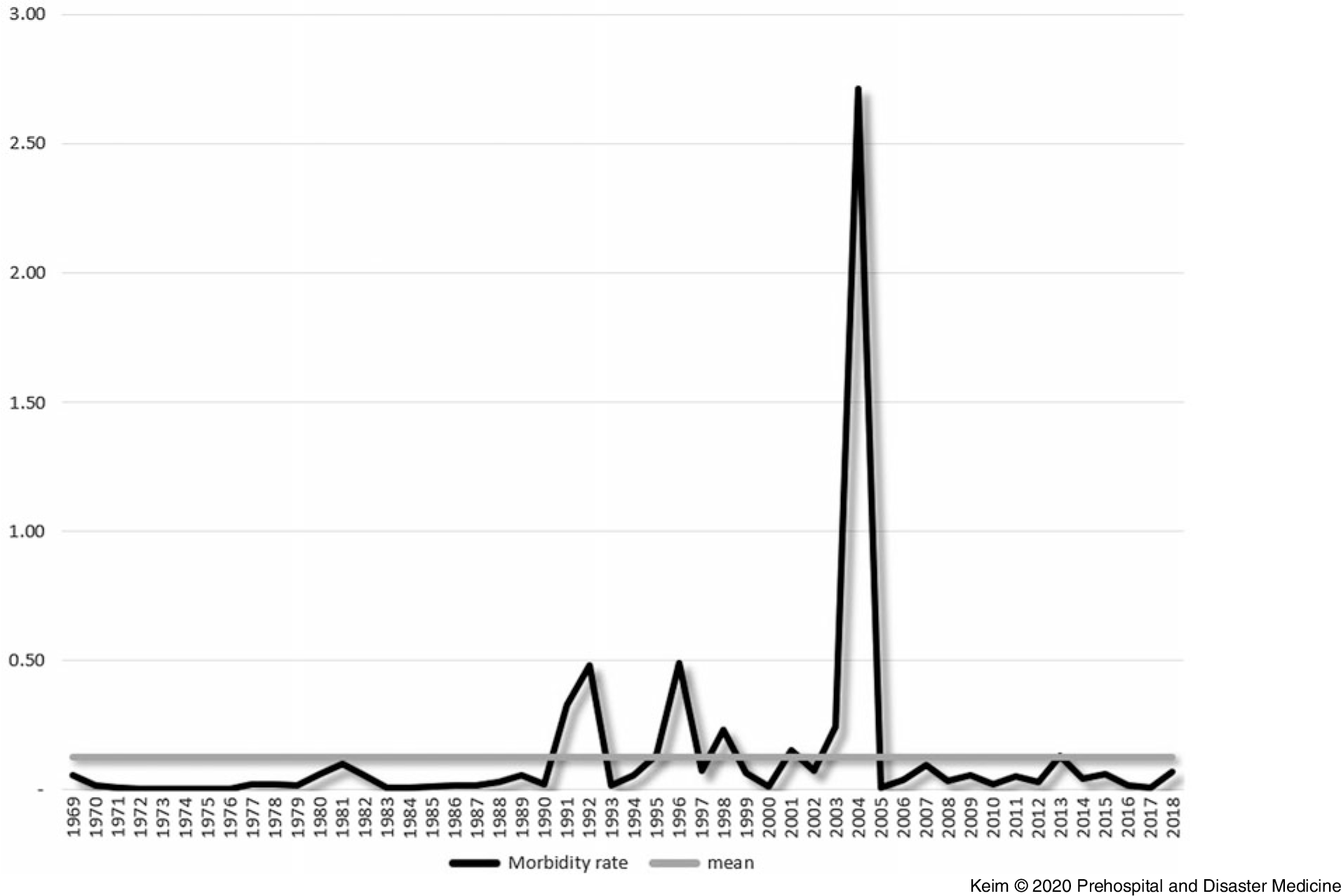
During the 50 years studied, EWE disasters caused nearly four million (3,998,466) cases of disease. Nearly one-half of global morbidity from EWE disasters was caused by cold (47%); with 31% caused by floods; and 18% caused by storms; followed by heat (4%), drought <1%), and wildfire (<1%). The mean annual incidence rate of EWE-related morbidity (injuries and illness) during this period was 0.13 cases per 100,000 persons. Figure 4 represents the annual global incidence rate of EWE-related morbidity over a 50-year period.

Figure 4. Annual Global Incidence Rate of Morbidity due to EWE Disasters (1969-2018).
There were eight years when annual morbidity occurred above the mean. Seven of the eight peaks could be directly attributed to increases caused mainly by only one hazard: floods (4); storms (2); and cold (1). During the remaining peak year (2013), 55% of the annual morbidity was due to heat and 37% was due to storms. It should also be noted that according to these data, during 2004, 98% of the 1,800,000 cases of EWE-related morbidity were reportedly due to the cold. This value represents a 22-fold increase over the annual average for all cold weather disasters during the same timeframe.
Results of multiple regression and ANOVA calculations performed to evaluate the association between the dependent variable of morbidity incidence rate were as follows for the independent variables of: exposure rate (R2 = 0.01; F significance = 0.69; and P value = .98); as well as for hazard incidence ((R2 = 0.01; F significance = 0.69; and P value = .42).
Discussion
During the past 50 years (1969-2018), 22,173 disasters (ie, caused by biological, natural, technological, extraterrestrial, and conflict hazards) were responsible for an estimated 6.2 million deaths and US$3.4 trillion in damages world-wide.7 One-half (50%) of these disaster events were climate-related and 95% of all people affected by disasters during this time were affected by climate-related disasters.7
Overall, the results of this study characterize a significant source of morbidity and mortality occurring on a global scale. To place this in context, the number of people affected world-wide by EWE disasters during the past 50 years (~seven billion) is roughly equivalent to the entire world’s population of current day.
Disaster-related health risk is caused by the joint probability of occurrence for both hazards and human exposures.Reference Keim8 In this study, there was an observed trend of increasing EWE hazard incidence, in the setting of no significant change in the measures (eg, number of persons affected) or potential proxies of exposure (eg, morbidity and mortality).
These results suggest with a high degree of certainty that the annual incidence of EWE disasters is increasing. There is also a moderate degree of evidence of an association between the incidence of EWEs and human exposure rates (ie, number of persons affected per 100,000 population). However, there were no significant changes noted for rates of EWE-related exposures, morbidity, or mortality during the past 50 years.
Limitations of the Study
In general, the effects of disaster events are the subject of gross approximations and aggregations that have a great deal of imprecision. The availability and quality of data has likely increased and improved over time and the use of multiple data sources increased reporting. However, in many events, deaths are unknown or unrecorded; for other outcomes such as injured and affected, reporting frequency is even lower, which likely contributes to a substantial under-estimation of the impacts of EWE disasters on human populations. While the available data are sufficient for a cursory analysis of global EWE disaster impacts and trends, improved reporting of EWE outcomes would improve the accuracy of the data and the validity of such conclusions.
Conclusion
During the past 50 years, floods and tropical cyclones were the most common EWE disasters, comprising 47% and 30% of all EWE disasters, respectively. Most EWE-related disaster mortality was caused by hazards related to tropical cyclones (39%), droughts (34%), and floods (16%). Nearly all EWE-related disaster morbidity was caused by hazards associated with cold weather (47%), floods (31%), and tropical cyclones (18%).
The results of this study strongly suggest that the incidence of EWEs is increasing, and that the incidence of EWEs is also associated with the rate of human exposure. However, there is insufficient evidence of an associated increase in health risk or human exposures to EWEs over time. In effect, during the past 50 years, while the incidence of health hazards has been increasing, the resultant health risks (in terms of morbidity and mortality) have remained relatively the same.
Further study is necessary to ascertain if this lack of association between hazard incidence and health risk may be an indicator of human capacity for resilience related to the absorption, adaptation, and transformation of climate-related risk.Reference Keim8
Conflicts of interest
none