



Introduction
The Middle East and North Africa (MENA) region has been, like many parts of the world, a hotbed for terrorist activities. Since the 1970s, 27.4% of all terrorist attacks took place in MENA, accounting for over 46,000 attacks, the highest of any region of the world. Reference Tin, Margus and Ciottone1,2 The “war on terror” campaign following the September 11, 2001 attacks in the United States primarily targeted extremist groups located in numerous countries, particularly in countries in South Asia and the Middle East. Terrorist attacks can affect both demand for and provision of health care services and often places a unique burden on first responders, hospitals, and health systems. Furthermore, intentional injuries to health care workers, damage to health care facilities, and general political instability can have significant psychosocial repercussions on the community and cause an efflux of health workers out of the region, placing further strain on already stressed systems. 3
This study aims to provide an epidemiological description of all terrorism-related attacks in the Middle East sustained from 1970-2019. These data will be useful in the development of education programs in Counter-Terrorism Medicine (CTM) and provide an insight into potential attacks in the future.
Methods
Data collection was performed using a retrospective database search through the Global Terrorism Database (GTD). 4 This database is open-access with publicly available data collection methodology utilizing artificial intelligence that identifies events from news media around the world and confirms them through human examination by the National Consortium for the Study of Terrorism and Responses to Terrorism (START; College Park, Maryland USA). The GTD defines terrorist attacks as “the threatened or actual use of illegal force and violence by a non-state actor to attain a political, economic, religious, or social goal through fear, coercion, or intimidation.” 5 The GTD does not include acts of state terrorism, contains no personal identifiers for victims, and links specific events to open-source news articles.
The GTD was searched using the internal database search functions for all events which occurred in Iraq, Yemen, Turkey, Egypt, Syria, West Bank and Gaza Strip, Israel, Lebanon, Iran, Saudi Arabia, Bahrain, Jordan, Kuwait, United Arab Emirates, North Yemen, Qatar, and South Yemen from January 1, 1970 - December 31, 2019. Cyprus (classified under Western Europe) and Oman were not listed under “Middle East” and were therefore not available for inclusion. Years 2020 and 2021 were not yet available at the time of the study. Primary weapon type, primary target type, country where the incident occurred, and number of deaths and injuries were collated by two separate data extractors and compared to locate any conflicts in extraction. No missing or inaccurate data/events were discovered during the course of the research.
Results were exported into an Excel spreadsheet (Microsoft Corp.; Redmond, Washington USA) for analysis. Ambiguous events (this field is only systematically available with incidents occurring after 1997) were excluded when there was uncertainty as to whether the incident met any of the criteria for GTD inclusion as a terrorist incident. Attacks met inclusion criteria if they fulfilled the following three terrorism-related criteria, as set by the GTD. These criteria are determined within the database and not by the authors:
-
- Criterion I: The act must be aimed at attaining a political, economic, religious, or social goal.
-
- Criterion II: There must be evidence of an intention to coerce, intimidate, or convey some other message to a larger audience (or audiences) than the immediate victims.
-
- Criterion III: The action must be outside the context of legitimate warfare activities (ie, the act must be outside the parameters permitted by international humanitarian law, particularly the admonition against deliberately targeting civilians or non-combatants).
Results
A total of 41,837 attacks occurred in the Middle East from 1970-2019 accounting for 24.9% of all terrorist attacks around the world. A total of 100,446 deaths were recorded with 187,447 non-fatal injuries. Fifty-six percent of all attacks in the region occurred in Iraq (23,426), 9.4% in Yemen (3,929), and 8.2% in Turkey (3,428), as shown in Table 1 and Figure 1.
Table 1. Attacks, Deaths, and Injuries in the Middle East
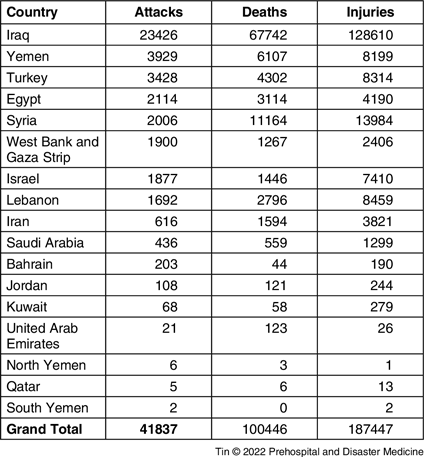
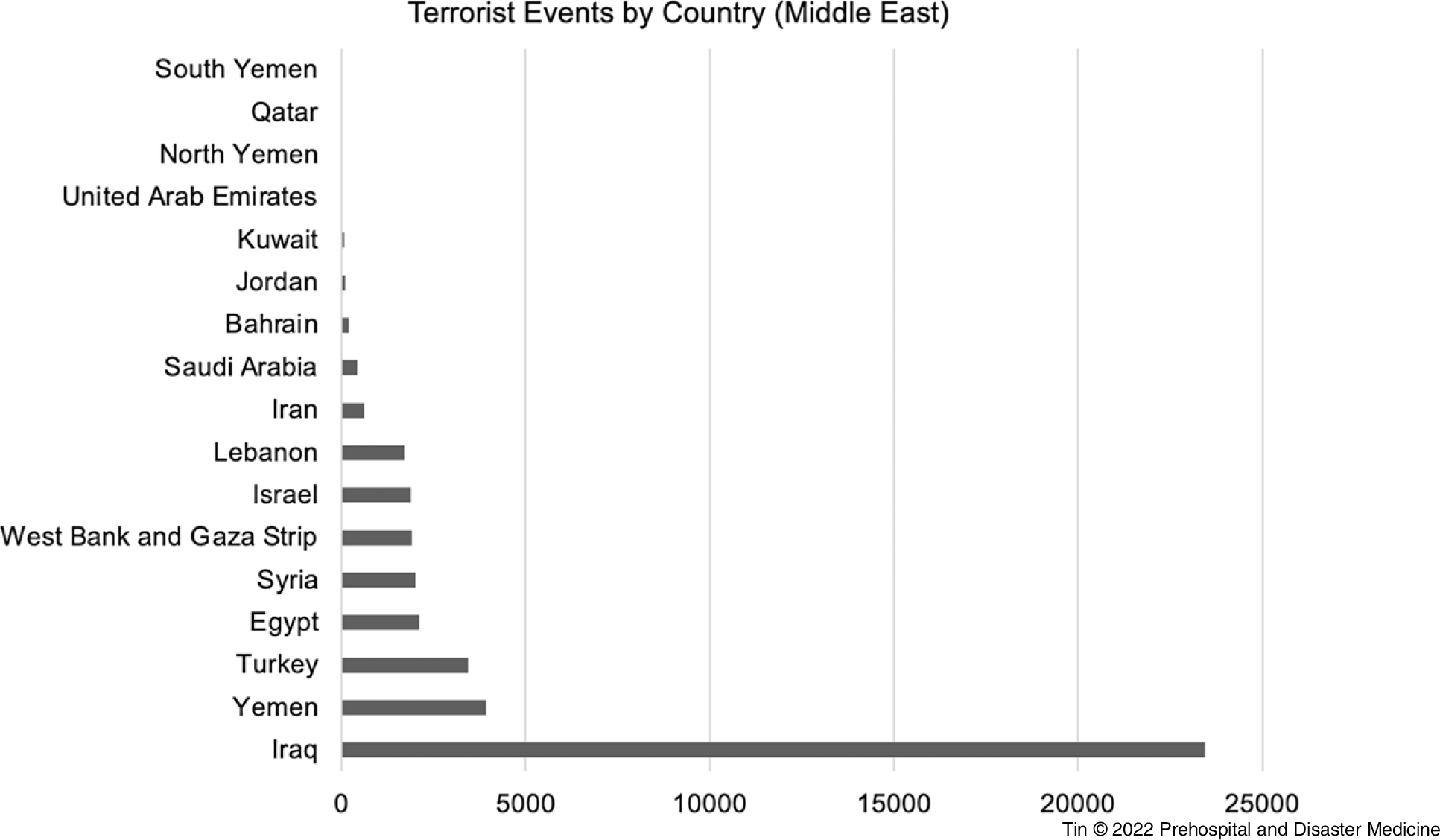
Figure 1. Terrorist Attacks by Country (Middle East).
“Private Citizens and Properties” were targeted in 37.6% (15,735) of attacks, 15.4% (6,423) targeted “Police,” 9.6% targeted “Businesses” (4,012), and 9.6% targeted “Governments” (4,001; Figure 2).
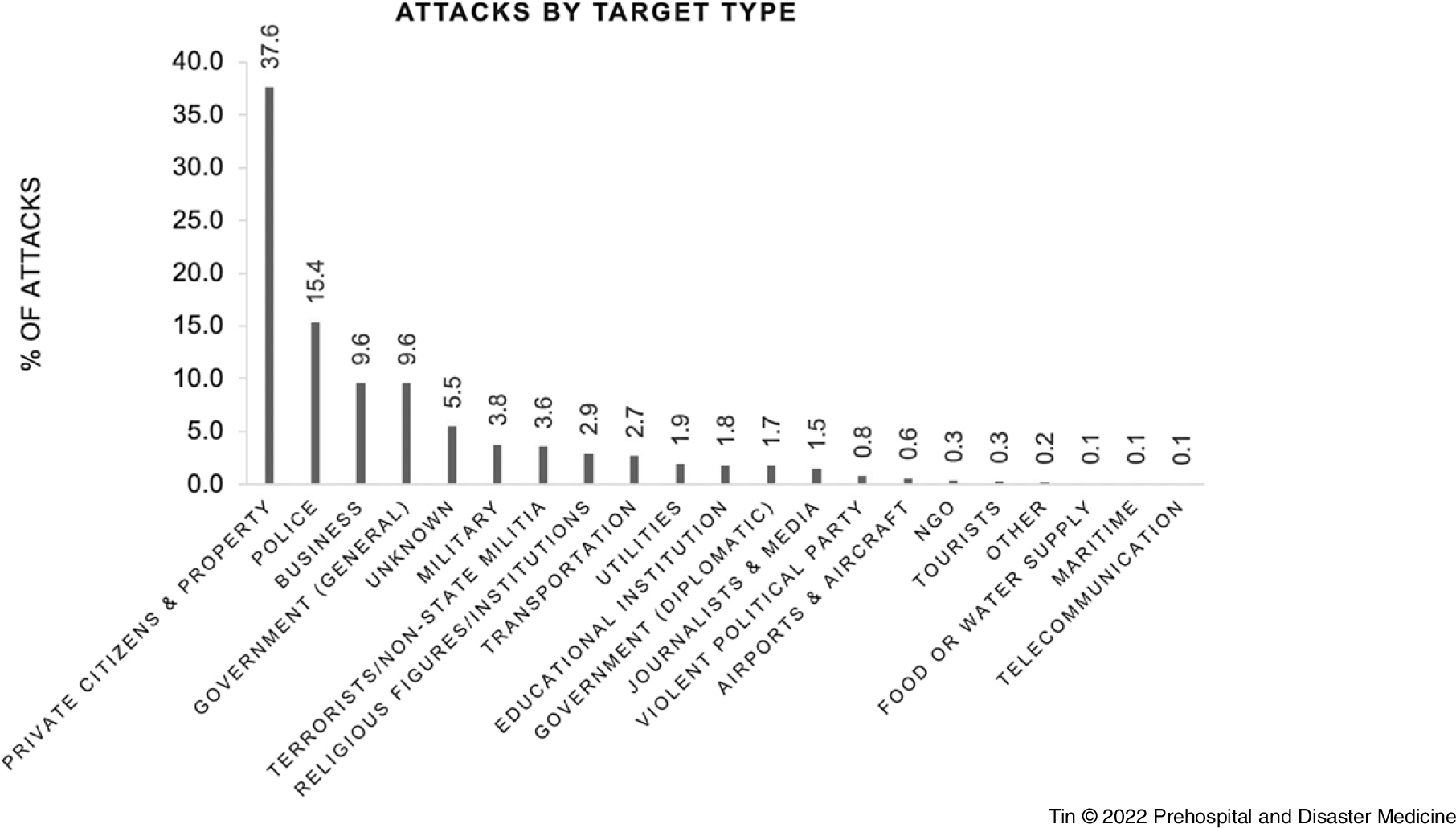
Figure 2. Attacks by Target Type.
Abbreviation: NGO, nongovernmental organization.
Explosives were used in 68.4% of attacks (28,607), followed by firearms in 20.4% of attacks (8,525; Figure 3).

Figure 3. Breakdown by Attack Modality.
The year 2014 saw a peak in terrorist activity, but there has been a downtrend in attacks since (Figure 4).
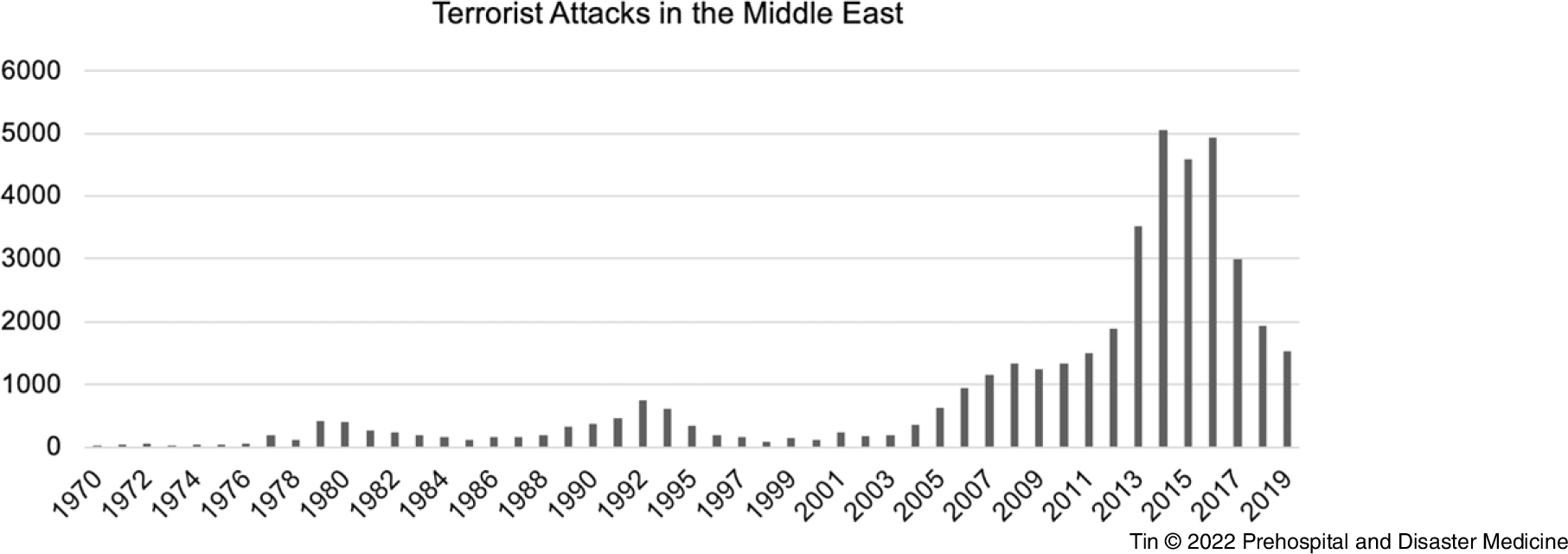
Figure 4. Number of Terrorist Attacks in the Middle East 1970-2019.
A total of 24,975 attacks were attributed to “unknown” perpetrator groups, 5,276 were attributed to the Islamic State of Iraq and the Levant (ISIL), 2,148 to Houthi extremists (Ansar Allah), and 1,543 to Kurdistan Workers’ Party (PKK).
Discussion
Middle Eastern and North African countries have historically been clustered into a single MENA region by international, economic, and academic organizations based on geographical, political, and cultural similarities. It is, however, important to acknowledge that socio-political circumstances, counter-terrorism mechanisms, and health care systems are unique to individual countries and as such, discussions regarding CTM analysis should ideally be individualized to each specific country. As such, several concepts in the discussion may not be generalized to all MENA regions, given the differences in the geopolitical situation among the different countries.
While there has been a downtrend in terrorist attacks both globally and in the Middle East the past several years, and especially since the start of the COVID-19 pandemic, experts predict a surge in activity as the world emerges from lockdowns and restrictions. 6 Western countries are facing problematic right-wing, white supremacy, and political extremist activity whereas countries in the Middle East, such as Iraq and Yemen, have their unique problems: on-going humanitarian, security, and political crises are often intertwined with deteriorating health care systems, with high burnout rates among physicians, nurses, and other medical professionals in the region associated with harsh work conditions, stress, and exposure to violence and conflict. Reference Tin, Hart and Ciottone7–Reference Alsabri, Alhadheri, Alsakkaf and Cole9 Health care workers have always been at the forefront of the response to terrorist attacks. Despite that, the effect on them has been very limited in the literature, especially during the “Arab Spring” and the subsequent events. Reference Bou-Karroum, Daou and Nomier10,Reference Bou-Karroum, El-Harakeh and Kassamany11 The Arab Spring destabilized several governments resulting in a significant increase in terrorist attacks with many today still arguing that the instability in the MENA region is not only about differences in religion, cultures, or identities, but about power, political control, and social privileges. Reference Horton12
In the 1970s, Iraq had developed a free, centralized, and universal health care system, funded by the country’s oil export profits. It was considered at the time to have some of the best health care facilities in the Middle East with 97% of the urban population and 71% of the rural population having access to free health care. 13 The 1980s and 1990s, under the rule of Saddam Hussein, were marked by significant deterioration of the socio-political circumstances in Iraq. Health care funding was de-prioritized, sectarian conflict, and the rise of ISIL led to unrest and a pro-terrorism dictatorship led to sanctions, forcing nongovernmental organizations (NGOs) to evacuate and thousands of local health care workers to flee or risk being killed or kidnapped. Reference Lafta and Al-Nuaimi14–Reference Woods16 Iraq’s health care system remains in crisis today with a shortage of drugs and staffing, with an average life expectancy of 70 years, far below average for the region. 17
As a result, the cultural and religious factors can influence disaster response strategies differently than in most Western countries. In Lebanon, for example, hospitals perform cultural analyses, taking into consideration the prevailing political parties within their catchment, and have strategies in place to physically separate patients and families from opposing sides of the feud whilst they are in hospital. Reference Iskandar, Rahbany and Shokor18 Gender-based sensitivities around the mixing of the sexes may also delay access to acute medical care in vulnerable populations. Reference Van der Zee19–Reference Davis22
The use of explosives and firearms as primary attack modalities in the Middle East follows the global trend in terrorist methodologies. Reference Tin, Margus and Ciottone1 Chemical, biological, radiological, nuclear (CBRN) attacks, though rare, remain a significant threat in the region. Syria saw the use of Sarin gas in 2013 which killed 1,400 civilians and severely affected thousands more and Sulfur Mustard filled rockets were launched in Iraq in 2016. Reference Sezigen and Kenar23,Reference Rosman, Eisenkraft and Milk24
Emerging technologies are also likely to feature in near-future terrorist attacks. The Islamic State and Houthi rebels have already demonstrated alacrity and capability to deploy unmanned aerial systems for both reconnaissance and offensive operations. Reference Marcus25–Reference Clarke27 This poses a real risk on much bigger communities, given the long-range reach of such technologies, and steps must be taken to prepare health care systems to deal with any unexpected incidents resulting from emerging technologies. Reference Tin, Kallenborn, Hart, Hertelendy and Ciottone26,Reference Pledger28
The emergence of CTM as a Disaster Medicine sub-specialty was borne out of the increasingly complex health care impacts of terrorist events. Health care systems and professionals, as well as security and intelligence agencies, need to be aware of historic and potential future attack methodologies and understand the unique death and injury patterns of specific attack modalities and target types. While retrospective studies provide enormous educational benefits, CTM specialists also need to be forward looking and both leverage the positive utilities and anticipate the nefarious use of novel and emerging technologies. Reference Tin, Kallenborn, Hart, Hertelendy and Ciottone26,Reference Tin, Hart, Hertelendy, Kallenborn and Ciottone29
Limitations
The GTD is a comprehensive record of global terrorist events. It is maintained by the National Consortium for the Study of Terrorism and Responses to Terrorism and is the basis for other terrorism-related measures, such as the Global Terrorism Index (GTI). Reliance wholly on the GTD is partially mitigated by confirmation with other lay sources and searches for other online searches, but if there are incidents not reported in the GTD, this could limit the veracity of the findings. Using pre-existing databases such as the GTD as a data source inherently introduces potential challenges such as miscoding errors or data entry errors. Furthermore, the lack of a universally agreed-upon definition of the term terrorism can create inconsistencies between databases in the labelling of such events. Clear and detailed documentation of terrorist events is further hindered by restrictions on reporting, the lack of independent corroboration, and the lack of transparency within government sources.
Conclusion
Despite a decline in terrorist attacks since a peak in 2014, terrorist events remain an important cause of death and injuries around the world, and especially in the Middle East where 24.9% of historic attacks took place. The Middle East follows the global trend in attack methodologies with prominent use of explosives, followed by firearms, as primary terrorist weapons. While MENA countries are often clustered together by economic and academic organizations based on geographical, political, and cultural similarities, there are significant differences in terrorist events between countries within the region. This is likely a reflection of the complexities of the intricate interplay between politics, culture, security, and intelligence services unique to each country.
Conflicts of interest/funding
No conflict of interest or financial disclosure to declare.





