



Introduction
Schistosomiasis is one of the most prevalent neglected tropical diseases in developing countries and is closely associated with poor sanitation, lack of clean water and low socioeconomic conditions (Danso-Appiah et al., Reference Danso-Appiah, Minton, Boamah, Otchere, Asmah, Rodgers, Bosompem, Eusebi and De Vlas2016). According to data from the World Health Organization (WHO, 2020a), this parasitosis is endemic in 78 countries. It is estimated that there are more than 200 million individuals with schistosomiasis globally and approximately 1 billion people live in areas at risk for transmission of the disease (Oliveira et al., Reference Oliveira, Magalhães, Elias, de Castro, Favero, Lindholz, Oliveira, Barbosa, Gil, Gomes, Graeff-Teixeira, Enk, Coelho, Carneiro, Negrão-Corrêa and Geiger2018). In Brazil, data from the Ministry of Health's National Survey on Prevalence of Schistosomiasis and Geo-Helminths (INPEG) estimated about 1.5 million people infected with Schistosoma mansoni in the country (almost 1% of the population) between 2011 and 2014 (Katz, Reference Katz2018). According to data from the Information System of the Schistosomiasis Control Program (SISPCE), Department of Informatics of the Unified Health System (DATASUS), analysis of the results of the examinations conducted over a longer period of time (2010–2015) estimated the positivity rate in the country at 4.4% (Brasil, 2017).
The diagnostic method most commonly used in epidemiological surveys for schistosomiasis mansoni is the Kato-Katz (KK) technique. However, the KK sensitivity decreases in individuals with low parasite loads. Thus, KK cannot be considered a ‘gold standard’. The WHO also recommends circulating cathodic antigen (CCA) testing in areas of active disease transmission (World Health Organization, 2020b).
The point-of-care (POC)-CCA test is a rapid qualitative diagnostic test for detection of S. mansoni infection. It detects a specific carbohydrate antigen associated with the parasite's gut. Adult worms regurgitate this antigen, which circulates in the bloodstream of the infected individual, is eliminated by the kidneys and can be detected in urine (van Dam et al., Reference van Dam, Wichers, Ferreira, Ghati, van Amerongen and Deelder2004). The use of urine rather than stool increases the acceptance of the testing in affected populations. In addition, the possibility of performing the testing in the field increases the speed with which results can be obtained and reduces requirements for modern equipment and advanced training (Utzinger et al., Reference Utzinger, Becker, van Lieshout, van Dam and Knopp2015).
In recent years, POC-CCA has been used in several endemic areas for schistosomiasis in Africa (Bärenbold et al., Reference Bärenbold, Garba, Colley, Fleming, Haggag, Ramzy, Assaré, Tukahebwa, Mbonigaba, Bucumi, Kebede, Yibi, Meité, Coulibaly, N'Goran, Tchuem Tchuenté, Mwinzi, Utzinger and Vounatsou2018; Rubaba et al., Reference Rubaba, Chimbari, Soko, Manyangadze and Mukaratirwa2018). Studies in areas where KK has a prevalence of ⩾50%, POC-CCA positivity is similar, showing a good performance when compared to KK (Kittur et al., Reference Kittur, Castleman, Campbell, King, Colley and Colley2016; Sanneh et al., Reference Sanneh, Joof, Sanyang, Renneker, Camara, Sey, Jagne, Baldeh, Ceesay, Sambou and Ogoussan2017; Fuss et al., Reference Fuss, Mazigo, Tappe, Kasang and Mueller2018; Okoyo et al., Reference Okoyo, Simiyu, Njenga and Mwandawiro2018). However, in areas with prevalence of ⩽50%, the POC-CCA is much more sensitive compared to KK, with an increase of 1.5- to 6-fold higher in the detection power as the prevalence by KK decreases (Tchuem Tchuenté et al., Reference Tchuem Tchuenté, Kueté Fouodo, Kamwa Ngassam, Sumo, Dongmo Noumedem, Kenfack, Gipwe, Nana, Stothard and Rollinson2012; Adriko et al., Reference Adriko, Standley, Tinkitina, Tukahebwa, Fenwick, Fleming, Sousa-Figueiredo, Stothard and Kabatereine2014; World Health Organization, 2020a, 2020b). As a result, there are still many uncertainties regarding the specificity and sensitivity of the POC-CCA test, especially with reference to the interpretation of weak ‘trace’ results, which are considered positive by the manufacturer.
In Africa, most studies find that POC-CCA is more sensitive compared to KK, but in Brazil the situation is different, with low sensitivity of POC-CCA in areas that have low KK prevalence (Bezerra et al., Reference Bezerra, Leal, Sousa, Pinheiro, Ramos, Silva-Moraes and Katz2018; Oliveira et al., Reference Oliveira, Magalhães, Elias, de Castro, Favero, Lindholz, Oliveira, Barbosa, Gil, Gomes, Graeff-Teixeira, Enk, Coelho, Carneiro, Negrão-Corrêa and Geiger2018). For further investigation of this phenomenon, we compared the performance of POC-CCA with KK, in an area of high endemicity, and we evaluated whether there is a correlation between the intensity of the immunochromatographic reaction of the POC-CCA test with the parasite load.
Materials and methods
Study area
The study was conducted in 2018 in the locality of Siebra, in the municipality of Maruim, Sergipe state, Brazil. This rural community has 179 residents, with similar numbers of men and women. The age range varies from 1 to 82 years (mean age 27.6 years), most people live in brick homes and are predominantly subsistence farmers. Siebra (10°44′6″ latitude and 37°04′35″ longitude) is located 32 km from the state capital, Aracaju (IBGE, 2016). According to data from the State Health Department, the last schistosomiasis assessment in Siebra was in 2008, showing a prevalence of 37.9% of S. mansoni infection in the community.
Ethical considerations
The study was approved by the ethics committee of the Federal University of Ceará – UFC (2647566) and by the ethics committee of the Federal University of Sergipe UFS (2806891). It was conducted in accordance with Resolution 466/12 of the National Health Council. District health authorities and the entire community were informed about the purpose, procedures, risks and potential benefits of the study. Prior to enrolment and collection of biological materials, written consent was obtained from participants. Parents/guardians and their children provided written consent for to participate in the research.
Sample collection
After giving consent, study participants provided three stool samples on alternating days, one urine sample and one fingerstick blood sample. Individuals who did not provide one of the requested biological samples, or did not deliver samples of sufficient quality and quantity to perform the procedures were excluded. Two slides per stool were prepared in loco by the KK technique using the Helm-Test® kit produced by Bio-Manguinhos-Fiocruz (Rio de Janeiro, RJ, Brazil). Urines were aliquoted and transported under refrigeration to the laboratory where they were stored at −20°C. Capillary blood was collected on filter paper (Tropbio Pty Ltd, QLD, Australia), dried, and stored at −20°C.
Kato-Katz
The six KK slides prepared for each study participant were screened for the presence of S. mansoni eggs (Katz et al., Reference Katz, Chaves and Pellegrino1972; Berhe et al., Reference Berhe, Medhin, Erko, Smith, Gedamu, Bereded, Moore, Habte, Redda, Gebre-Michael and Gundersen2004). The intensity of infection was expressed as eggs per gram (EPG) feces and infected individuals were classified as having low (1–99 EPG), moderate (100–399) or heavy (⩾400 EPG) intensity infections according to WHO guidelines (World Health Organization, 2011).
Circulating cathodic antigen test (POC-CCA)
For POC-CCA diagnosis, all urine specimens were thawed and processed according to the manufacturer's instructions (Rapid Medical Diagnostics, Pretoria, South Africa). All kits used were part of the same lot (lot no. 180703067). The tests were classified using the G (G1–G10) score scale as standard, with G1 considered negative, G2 and G3 considered trace and G4–G10 being positive, according to the reaction intensity of the test band (Casacuberta-Partal et al., Reference Casacuberta-Partal, Hoekstra, Kornelis, van Lieshout and van Dam2019). Positive results were stratified (Table 1) using a semi-quantitative scale at 1+ (G4 and G5), 2+ (G6 and G7) and 3+ (G8–G10) (Casacuberta-Partal et al., Reference Casacuberta-Partal, Hoekstra, Kornelis, van Lieshout and van Dam2019). All tests were read by two trained investigators throughout the study. In cases of discordant results, a third investigator was consulted until a consensus was reached.
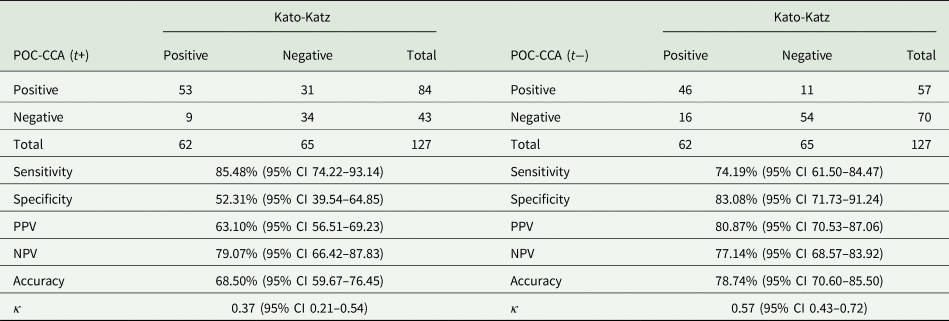
Table 1. Prevalence of schistosomiasis according to KK and POC-CCA method, considering trace as positive (t+) and trace as negative (t−), in the 127 individuals tested

POC-CCA filter test (POC-CCA-FLT)
The samples that were negative or ‘trace’ by POC-CCA but were from persons who were egg positive by the KK technique, were concentrated by filtering 0.5 mL of urine through a 30-kDa membrane (MRCF0R030, Merck Millipore, Darmstadt, Germany), and then centrifuged for 30 min, at 2000 g. The pellet was resuspended in 0.05 mL distilled water, and then tested again by POC-CCA (Grenfell et al., Reference Grenfell, Taboada, Coutinho, Pedrosa, Assis, Oliveira, Cruz, Almeida, Silva-Moraes, Katz and Coelho2018).
Enzyme-linked immunosorbent assay (ELISA)
For the ELISA, dried blood spots were sent to the Division of Parasitic Diseases and Malaria at the Centers for Disease Control and Prevention in Atlanta, GA USA. In brief, the sample of blood was transferred to a 1.5 mL microtube and incubated at 4°C overnight with 250 μL of 0.1 m phosphate-buffered saline (PBS) containing 0.3% Tween 20 and 5% nonfat milk. After overnight incubation on a shaker, the samples were transferred to Immulon 2HB plates (ThermoScientific, Rochester, NY) that had been coated with 100 μL of 2 μg mL−1 soluble schistosome egg antigen in 0.1 m sodium bicarbonate buffer, pH 9.6. Standards, controls and samples were diluted to a 1:50 concentration with 0.01 m PBS, pH 7.2/0.3% Tween-20/5% milk and allowed to incubate on the plate at room temperature for 30 min. All standards, controls and samples were run in duplicate. Plates were washed five times with PBS containing 0.3% Tween 20. The conjugate used was mouse anti-human IgG HRP (SouthernBiotech, Birmingham, AL) prepared at a dilution of 1:50 000 in 0.01 m PBS, pH 7.2/0.3% Tween-20 and incubated for 30 min. Following incubation with the conjugate and washing plate as above, room temperature SureBlue™ TMB substrate (SeraCare Life Sciences, Gaithersbug, MD) was allowed to incubate for 5 min prior to the addition of 1 N sulphuric acid to stop any further reaction. A standard curve of 0–500 arbitrary units (AU) using pooled positive sera was included on each plate. The cutoff used for positives is 40 AU.
Statistical analysis
All data were entered into Excel spreadsheets (Microsoft Corp., Redmond, WA, USA) for management and analysis. To determine the performance of each method, we calculated the sensitivity, specificity, positive (PPV) and negative (NPV) predictive values using MedCalc® statistical software, version 19.1 (Osten, Belgium). The agreement between the results of the KK and POC-CCA techniques, as well as the relationship of parasitic load (EPG) with the intensity of the reaction detected by POC-CCA was evaluated using the kappa index, calculated using the MedCalc® program. The graphics were created using GraphPad Prism® 6, version 6.1 for Windows (GraphPad Software, La Jolla California, USA).
Receiver operating characteristic (ROC) curves were used to compare sensitivity and specificity between tests, evaluating the true-positive rate vs the false-positive rate.
The correlations between the mean EPG, determined by KK egg counts and the intensity of the POC-CCA reaction, classified through the semi-quantitative scale, were calculated using the nonparametric Spearman test. Differences were considered statistically significant when P < 0.05.
Results
Of the 179 inhabitants of Siebra, 127 (70.95%) participated in the study; 55 (43.31%) were men and 72 (56.69%) were women, with an average age of 27.2 years. The prevalence for S. mansoni, according to the KK technique, was 48.82% (62/127).
Stratification of parasitic load by EPG showed 29.03% (18/62) with heavy intensity infections, 16.13% (10/62) with moderate intensity infections and 54.84% (34/62) with low intensity infections. The geometric mean EPG of the participants was 390.3 [95% confidence interval (CI) 230.5–530.1].
The POC-CCA results showed 57 positives (44.88%), 27 ‘trace’ (21.26%) and 43 negatives (33.86%). The positivity index for schistosomiasis by POC-CCA was 66.14% (84/127), considering (t+) and 44.88% (57/127), considering (t−) (Table 1).
Positive results are stratified in Table 2 by age group and diagnostic method used. Children aged 10–14 years presented the highest percentage of positivity. Of the positive individuals, identified by the KK technique, 29% were in the age groups under 15 years and approximately 34% in the age groups between 19 and 29 years. From 50 years onwards, the positivity rates reduced to approximately 10%, in both diagnostic methods used.
Table 2. Prevalence in the different methods used, stratified by age group

A greater concordance was identified between the KK and POC-CCA results when trace was considered negative and the diagnostic failure was higher when trace was considered positive. Of the individuals who were egg positive by the KK technique, 25.8% were negative by POC-CCA (t−). Among the 43 individuals negative by POC-CCA (t+), 20.93% (9/43) were egg positive by the KK technique. Only 25.93% (7/27) of the individuals who had trace POC-CCA had detectable eggs in their stool (Table 3).
Table 3. Analysis of agreement and diagnostic accuracy of POC-CCA, compared to KK results
CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value; k, Kappa coefficient.
The agreement, calculated using the kappa index, considering POC-CCA (t+) and KK, was 68% (k = 0.37), considered as a discrete agreement (standard error: 0.0859). Sensitivity was 85.48% and specificity was 52.31%, with a PPV of 63.10%, NPV of 79.07% and accuracy of 68.50% (Table 3). When we considered POC-CCA (t−), we observed that the agreement improved to 78% (k = 0.57), considered as a moderate agreement (standard error: 0.0728). Sensitivity dropped to 74.19%, but specificity increased to 83.08%. PPV, NPV and accuracy were 80.87, 77.14 and 78.74%, respectively (Table 3).
When ROC curve analyses were performed using the KK results as reference, POC-CCA (t+) had smaller sensitivity. The POC-CCA, when the trace was considered negative, had higher discriminatory power, with an area under the curve (AUC) of 0.786 (Fig. 1).

Fig. 1. ROC curves and AUC of CCA results using KK as reference.
Table 4 presents the classification of POC-CCA results, stratified by G score and the semi-quantitative scale. The semi-quantitative scale classified 47.37% (27/57) of the positive individuals as 3+ (high reactivity), 21.05% (12/57) as 2+ (moderate reactivity) and 31.58% (18/57) as 1+ (low reactivity). G10 was the only class that showed 100% correlation with individuals with heavy intensity parasitic infection. Among the negative and POC-CCA (t+) individuals who had S. mansoni eggs in their feces, 87.50% had low intensity infections, with a maximum of six eggs in a total of six slides analysed. Another important finding is that POC-CCA (t−) failed to detect infection in 16 (22.86%) egg-positive individuals.
Table 4. Results of POC-CCA, classified by G-score and semi-quantitative scale, ELISA, KK and parasitic load

*Visual score based on the semi-quantitative scale; R, reactive; NR, non-reactive.
Evaluating the agreement only between the positive individuals in the POC-CCA (G4–G10), that is, considering trace as negative, we found a weak agreement between the parasitic load found by KK and the intensity of the immunochromatographic reaction defined by the semi-quantitative scale, with an agreement index of 54%, κ of 0.29 and standard error of 0.1128. The correlation between these tests by the Spearman calculation was moderate (r = 0.54; P < 0.001; 95% CI 0.305–0.723) (Fig. 2).
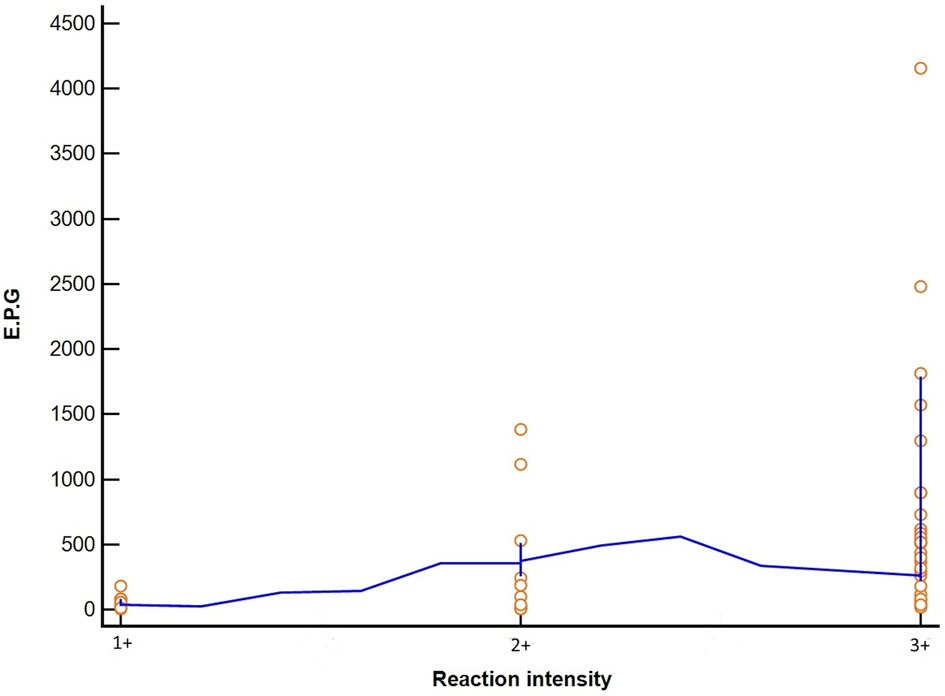
Fig. 2. Correlation between intensity of POC-CCA test bands (G4–G10), classified by semi-quantitative scale, and comparison with parasitic loads according to the KK technique.
We reevaluated the nine POC-CCA ‘trace’ individuals who were KK positive using the POC-CCA filtration (POC-CCA-FLT) technique as well as eight POC-CCA negative individuals who were egg positive. All subjects with ‘trace’ results before urine filtration were positive after the antigen concentration step, five increased to 1+, three to 2+ and one to 3+. Among the eight individuals with eggs that were initially POC-CCA negative, six (75%) became positive, with low reaction intensity (four were 1+ and two were 2+) and two remained negative (25%).
When we evaluated POC-CCA and ELISA results in KK positive individuals, separated by intensity of infection, the ELISA was positive for 90.32% of the individuals with eggs in their stool and was 100% reactive in individuals with moderate and heavy intensity EPG (Table 5).
Table 5. Results of ELISA and POC-CCA techniques stratified according to the parasite load determined by the KK method

EPG, Eggs per gram of feces; R, reactive; NR, non-reactive.
Table 5 shows the classification of the stratified results of KK positivity in relation to the POC-CCA and ELISA, of 28/62 (45.2%) individuals with high and moderate EPG, 100% were positive in the POC-CCA, and all were reactive in the ELISA technique. Of 34/62 (54.8%) who presented low EPG, the POC-CCA (+) detected 21/34 (61.8%), and the ELISA 28/34 (82.35%).
Discussion
The locality of Siebra (Maruim, SE, Brazil) is a highly endemic area, with schistosomiasis prevalence >45%. The average parasite load of the population was 380.3 EPG, where the majority (57.14%) presented low parasite load, but almost 30% had heavy intensity infections. These rates can be explained by the water contact activities of the community (92.74% of the population reports contact), and very poor access to drinking water (9.50%) and sanitary sewage (6.70%). These environmental characteristics are similar in most of the hyperendemic areas, where the poor sanitation conditions contribute to transmission (Saucha et al., Reference Saucha, da Silva, Amorim, Saucha, da Silva and Amorim2015).
The high prevalence of schistosomiasis in this area is worrying because it is concentrated in children and economically active age groups, leading to persistence in disease transmission and increasing the risk development of severe pathology, along with an increase in the disability-adjusted life-year index, which directly affects the population's living conditions and perpetuates the cycle of poverty (Nascimento and de Oliveira, Reference Nascimento and de Oliveira2010). Data from the Schistosomiasis Control Program (PCE) show that of the 6248 parasitological tests (KK technique) performed in the municipality of Maruim between 2000 and 2011, 26.2% were positive. Of these, 48.9% had low parasitic load, 30.7% had moderate intensity infections and 20.4% had heavy intensity infections. Only patients who had S. mansoni eggs in their feces were treated and no other control action was developed by the PCE. As of 2012, the programme did not carry out activities in the municipality as a result of cuts in the federal, state and municipal government health budgets and the prioritization of financial resources towards combating arboviruses (Brasil, 2017).
The POC-CCA (t−) had similar prevalence results to the KK method; however, the number of false negatives (16/127) resulted in only a moderate agreement between these methods. Among the POC-CCA negative (20.93%) and trace (25.92%) participants, some were egg positive with a very low parasitic load (3.9–48 EPG). Other studies performed in Brazil had negative POC-CCA results in individuals with light intensity infections, with most discordant results occurring when trace results were considered positive (Bezerra et al., Reference Bezerra, Leal, Sousa, Pinheiro, Ramos, Silva-Moraes and Katz2018; Oliveira et al., Reference Oliveira, Magalhães, Elias, de Castro, Favero, Lindholz, Oliveira, Barbosa, Gil, Gomes, Graeff-Teixeira, Enk, Coelho, Carneiro, Negrão-Corrêa and Geiger2018; Sousa et al., Reference Sousa, Van Dam, Pinheiro, de Dood, Peralta, Peralta, Daher, Corstjens and Bezerra2019). We also found that some POC-CCA positive individuals were egg negative by KK, similar to other studies showing POC-CCA is more sensitive than stool microscopy (Ashton et al., Reference Ashton, Stewart, Petty, Lado, Finn, Brooker and Kolaczinski2011; Colley et al., Reference Colley, Binder, Campbell, King, Tchuenté, N'Goran, Erko, Karanja, Kabatereine, van Lieshout and Rathbun2013; Sousa-Figueiredo et al., Reference Sousa-Figueiredo, Betson, Kabatereine and Stothard2013).
When trace was considered positive, prevalence was possibly overestimated, as there was an increase in sensitivity but a reduction in specificity and PPV. These data are similar to those of studies conducted in communities on the shores of Lake Victoria, Africa (Standley et al., Reference Standley, Lwambo, Lange, Kariuki, Adriko and Stothard2010) and Januária in northern Minas Gerais, Brazil (Oliveira et al., Reference Oliveira, Magalhães, Elias, de Castro, Favero, Lindholz, Oliveira, Barbosa, Gil, Gomes, Graeff-Teixeira, Enk, Coelho, Carneiro, Negrão-Corrêa and Geiger2018). These results in disparate regions suggest that POC-CCA has more accurate results when trace is considered negative.
The intensity of the POC-CCA reaction (semi-quantitative scale) showed moderate (r = 0.54) correlation with parasitic load based on EPG but agreement between tests was poor (κ = 0.29). The correlation may have been affected by the wide range of EPG values in persons with a class 3+ POC-CCA. Individuals with G8 and G9 POC-CCA scores had diverse parasitic loads (19.9–1812 EPG). Category G10, also class 3+, was the only one in which all individuals had a high parasite load (516–4156 EPG). Class 2+ (G6 and G7) also included individuals with very low egg counts. Our test agreement was similar to what Casacuberta et al. (Reference Casacuberta-Partal, Kinunghi, Vennervald and Olsen2016) found in a highly endemic area in southeastern Uganda (r = 0.660) and what Silveira et al. (Reference Silveira, Costa, Ray, Suzuki, Hsieh, de Fraga and Caffrey2016) observed in low and moderate intensity areas in southeastern Brazil (r = 0.625). However, the agreement rate (κ = 0.29) in our study was much lower than seen in southeastern Brazil (κ = 0.66). This suggests that EPG cannot be inferred based only on the intensity of the POC-CCA reaction.
POC-CCA-FLT improved accuracy over conventional POC-CCA; however, we observed that some samples (25%) continue to show false negative results (KK positive but and negative in conventional POC-CCA and POC-CCA-FLT). By contrast, all trace individuals in the conventional POC-CCA who were KK positive had a positive POC-CCA-FLT result. A study conducted in two cities in southeastern Brazil, where the POC-CCA and POC-CCA-FLT tests were evaluated compared to the KK results, also showed that the POC-CCA FLT had superior results in the diagnosis of schistosomiasis compared to traditional POC-CCA (Grenfell et al., Reference Grenfell, Taboada, Coutinho, Pedrosa, Assis, Oliveira, Cruz, Almeida, Silva-Moraes, Katz and Coelho2018). However, the addition of the filtration step makes the test cease to be point-of-care. It also increases costs because adding the 30 kDa filter (MRCF0R030, Merck Millipore, Darmstadt, Germany) raises the price by 102.46%.
Although POC-CCA (t−) detected fewer egg-positive individuals compared to POC-CCA (t+), it still had a higher diagnostic accuracy based on percent agreement, the kappa index, accuracy and AUC. However, for decision-making regarding individual or community-wide treatment, both missed a considerable number of infections (over 20%), which could lead to undertreatment and a perpetuation of schistosomiasis transmission. But if we consider that in an area of high endemicity, the main objective is to reduce prevalence of high intensity infections to <5% and prevent development of severe disease, whether trace is considered positive or negative becomes irrelevant, since the POC-CCA (45.75 and 67.72%, t− and t+ respectively) and KK (48.73%) result in the same mass treatment decision determined by the Brazilian Ministry of Health (Brasil, 2019).
Of the 127 individuals analysed by ELISA, 74 were reactive, suggesting that 59.05% of the residents of Siebra had contact with the parasite. The tests used showed 100% agreement in individuals with heavy and moderate intensity parasitic loads. Those classified with light intensity infections by KK showed some false negative by ELISA and POC-CCA. Although these losses were not significant, our data show that both the POC-CCA and the ELISA have differences diagnostic reactivities in individuals with low intensity infections.
Studies in both Brazil and Africa show that POC-CCA has greater sensitivity compared to KK (Shane et al., Reference Shane, Verani, Abudho, Montgomery, Blackstock, Mwinzi, Butler, Karanja and Secor2011; Chernet et al., Reference Chernet, Kling, Sydow, Kuenzli, Hatz, Utzinger, van Lieshout, Marti, Nickel, Labhardt and Neumayr2017; Fuss et al., Reference Fuss, Mazigo, Tappe, Kasang and Mueller2018), however it is worth mentioning that in our study we found a number of individuals who were POC-CCA negative with the presence of eggs, as reported in other studies as well (Siqueira et al., Reference Siqueira, Couto, Taboada, Oliveira, Carneiro, Oliveira, Coelho and Katz2016; Lindholz et al., Reference Lindholz, Favero, CdM, Candido, de Souza, dos Santos, Morassutti, Bittencourt, Jones, Pierre and Graeff-Yeixeira2018).
Conclusion and future directions
Our data suggest that POC-CCA (t−) results are closer to those KK (individuals with heavy intensity infections) and show a better agreement between tests, leading to higher diagnostic accuracy. Nevertheless, there are still a high number of false negatives even in an area of high endemicity. A moderate positive correlation was observed between the reaction of POC-CCA intensity with parasitic load, but with large disagreement of individual results between tests, calling into question the use of the POC-CCA semi-quantitative scale to estimate infection intensity.
As observed by others in Brazil, POC-CCA-FLT improves the test accuracy and sensitivity compared to conventional POC-CCA. However, the addition of this one step makes the test no longer point-of-care and doubles the test costs.
Acknowledgements
We thank the Secretary of State of Health of Sergipe and the Secretary of Health of the municipality of Maruim for their technical support, the people of the Siebra community for their collaboration in implementing this project; Dr Govert van Dam of the University of Leiden in the Netherlands for giving us the parameters for reading the POC-CCA and for donating the Rapid Medical Diagnostics POC-CCA kits; Dr William Evan Secor from the Division of Parasitic Diseases and Malaria, Centers for Disease Control and Prevention, Atlanta, GA, USA, for the ELISA support. We also acknowledge The Federal University of Sergipe and CAPES for granting scholarships to the postgraduate students involved in this study.
Author contributions
Conceived of or designed study: FSMB, MCCP and LB; performed research: DFB, FSMB and MCCP; analysed data: FSMB, DFB and MCCP; contributed new methods or models: RTF, AGV and LB; wrote the paper: DFB and MCCP; wrote sections and revising it critically: DFB, MCCP, LB, AGV, RTF and FSMB. All the authors approved the final version of the manuscript.
Financial support
This work was supported by the CAPES – Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (grant for DFB).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical standards
The authors assert that all procedures contributing to this study comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study was approved by the Ethics Committee of the Federal University of Ceará – UFC (No. 2647566) and by the Ethics Committee of the Federal University of Sergipe UFS (No. 2806891).
Informed consent
Written informed consent was obtained from all individual participants included in the study. The parents/guardians and their children provided written consent for to participate in the research.







