Introduction
Family-centered care involves consideration of the family context in care planning discussions and decisions and is one of the cornerstones of palliative care (National Consensus Project for Quality Palliative Care, 2018; Kokorelias et al., Reference Kokorelias, Gignac and Naglie2019). Yet, there is still a lack of high-quality family-centered interventions in palliative care (Areia et al., Reference Areia, Gongora and Major2020). While research has shown that family caregivers experience significant anxiety and reduced quality of life due to the caregiving experience (National Academies of Sciences & Medicine, 2016), it remains unclear what specific elements make family-centered interventions effective and how to improve communication with family caregivers (Deek et al., Reference Deek, Hamilton and Brown2016). The Global State of Care Report by the International Alliance of Carer Organizations identifies communication and information exchange between family caregiver and healthcare provider as one of four areas in need of improvement for family-centered care (International Alliance of Carer Organizations, 2018).
Understanding caregiver communication behaviors with physicians is important in improving multi-level communication and palliative care interventions for family caregivers. Physicians, nurses, and nurse practitioners report that a lack of collaboration exists with caregivers due to fluctuating levels of caregiver involvement, inability to reach caregivers, and provider time constraints (American Association of Retired Persons, 2019). Yet, physicians are most likely to speak with caregivers (Skufca, Reference Skufca2019) and are most likely to provide a referral to palliative care; however, communication difficulties are commonly reported as a barrier to an effective physician–caregiver relationship (American Association of Retired Persons, 2019). These difficulties may be due, in part, to how palliative care is introduced to the family and whether or not the family caregiver understands the goals of palliative care. National research has shown that caregivers are painfully unaware of palliative care and among those who have heard of palliative care, the majority do not see it as separate from hospice care and death (Dionne-Odom et al., Reference Dionne-Odom, Ornstein and Kent2019). Physician–caregiver interactions also tend to focus only on medical tasks (Skufca, Reference Skufca2019), which means that important psychosocial caregiver needs are often overlooked. Additionally, the majority of physicians currently in practice learned communication skills on the job, without a curriculum or evidence-based learning techniques, and communication competency for interactions with caregivers varies (Back et al., Reference Back, Fromme and Meier2019).
As the majority of palliative care services are through physician referral, a closer look at caregiver communication with physicians is warranted in order to learn more about best approaches for improving family-centered communication and care outcomes. Poor family caregiver outcomes are associated with caregivers’ unmet need for information during care transitions, including the patient's prognosis and treatment, symptoms and side effects, and names of the healthcare providers (Shin et al., Reference Shin, Cho and Kim2018; McCusker et al., Reference McCusker, Yaffe and Lambert2020). Family caregivers often lack information about the help that physicians can offer and do not always have supportive relationships with providers (Schulz et al., Reference Schulz, Beach and Friedman2018). In the United States, almost a third of caregivers report at least one unmet supportive care need (Mollica et al., Reference Mollica, Smith and Kent2020).
Communicating with physicians and nurses is highly stressful for caregivers who struggle to accept a patient's poor condition, hold unrealistic expectations about the patient's quality of life after hospitalization, or experience a lack of trust with the healthcare team (Wittenberg et al., Reference Wittenberg, Goldsmith and Ragan2020b). Available online resources instruct caregivers to introduce themselves to the care team, share patient symptom management information, ask questions, request that the healthcare provider explain further, and communicate assertively (Keast et al., Reference Keast, Butow and Juraskova2020). However, these communication tasks may not be in alignment with disease-related family communication techniques, such as open or closed communication about illness (Rosland et al., Reference Rosland, Heisler and Piette2012), and research has shown that communication burden, such as initiating conversations about illness, impacts caregiver physical, social, psychological, and spiritual quality of life (Wittenberg et al., Reference Wittenberg, Borneman and Koczywas2017a).
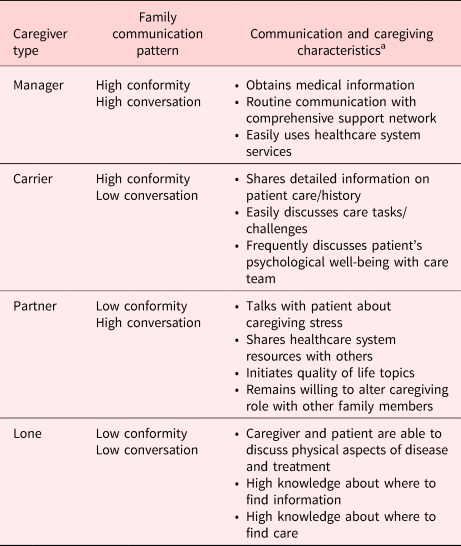
Family communication patterns influence the ways that patients and caregivers communicate with providers (Rosland et al., Reference Rosland, Heisler and Piette2012; Rauscher et al., Reference Rauscher, Hesse and Campbell-Salome2020). Family communication patterns are related to an individual's cognitive flexibility, interpersonal skills, and information processing (Greene et al., Reference Greene, Morgan and Anderson2014) and consist of family rules/scripts for communicating (McLeod and Chaffee, Reference McLeod and Chaffee1973; Ritchie and Fitzpatrick, Reference Ritchie and Fitzpatrick1990; Fitzpatrick and Ritchie, Reference Fitzpatrick and Ritchie1994). These family rules are governed by two family beliefs regarding conformity and conversation, with each dimension of communication representing a high and low end. The Family Caregiver Communication Typology (Table 1) provides a framework for understanding family communication during illness and gives shape to four caregiver communication types (Wittenberg et al., Reference Wittenberg, Kravits and Goldsmith2017b). Family members share a unique relational history; thus, not all family members are the same family caregiver type (Caughlin et al., Reference Caughlin, Mikucki-Enyart and Middelton2011; Wittenberg et al., Reference Wittenberg, Ferrell and Goldsmith2016). The emergent caregiver type is dependent upon the relationship between the care recipient and the family caregiver based on communication patterns established over time within the family system.
Table 1. Overview of Family Caregiver Communication Typology

a Wittenberg et al. (Reference Wittenberg, Goldsmith and Ragan2020a).
The four caregiver types of the Family Caregiver Communication Typology are Manager, Partner, Carrier, and Lone caregivers (Wittenberg et al., Reference Wittenberg, Goldsmith and Ragan2020a). Manager caregivers serve as a self-appointed family spokesperson, limiting other family members, and the patient in the decision-making process; Carrier caregivers surrender to family and patient authority, absorbing the greatest burden, and experiencing the most costly sacrifices; Partner caregivers emphasize education about the disease, placement options, and familial efforts to flexibly play varying roles in their work with patient and providers; and finally, Lone caregivers experience no familial support or shared burden, and focus primarily on the biomedical concerns of care (Wittenberg et al., Reference Wittenberg, Goldsmith and Ragan2020a).
Caregiving requires communication skills for improving healthcare during clinical visits (Office of Disease Prevention and Health Promotion, 2019) and active involvement in health care requires self-efficacy in communicating with physicians (Capone and Petrillo, Reference Capone and Petrillo2014). Recent research has utilized content and linguistic observations to conclude four variations of active or passive caregiver communication with physicians, revealing a range from trusting, resigned, egalitarian, and aggressive communication (Peters et al., Reference Peters, Dykes and Heckel2019). Similarly, family caregiver communication type informs the communication behaviors exhibited with healthcare providers (Wittenberg-Lyles et al., Reference Wittenberg-Lyles, Goldsmith and Oliver2012). Despite observational data findings, research has not yet accounted for self-report measures from caregivers. The aim of our present work seeks to determine if caregiver types differ in their perceived communication self-efficacy with physicians. Our objective was to further validate the model of Family Caregiver Communication Typology by ascertaining whether or not differences exist and if there is a relationship between communication self-efficacy and caregiver outcomes (anxiety and quality of life) across the four caregiver communication types.
Methods
Given the difficulty of recruiting diverse caregivers in healthcare settings (Hansen et al., Reference Hansen, Petrinec and Hebeshy2019), an online survey was used to reach a representative population of family caregivers (King et al., Reference King, O'Rourke and DeLongis2014; Whitaker et al., Reference Whitaker, Stevelink and Fear2017). At a Hispanic-serving institution, which has at least 25% of undergraduate full-time students that self-identify as Hispanic, undergraduate and graduate students completed university-required online research training and certification. Following a 1-h course lecture about family caregiving and the study protocol highlighting caregiver eligibility criteria, students received credit if they invited a qualified family caregiver to contact the research team to participate. Convenience sample methods were used to recruit eligible caregivers by posting the study on Facebook and/or sharing study information with personal connections via email. Caregivers had to be a friend or family member providing support to a person with chronic illness, defined as "someone who has to go to the doctor often or take medicine all of the time." Caregivers had to be at least 18 years of age. Interested caregivers meeting the inclusion requirements were emailed a link to the online survey. No incentive was offered to caregivers for their participation. The survey was conducted between February and April 2019. Participation was voluntary and anonymous. This research activity was considered exempt under the supporting university's Institutional Review Board (#1156666), with a waiver of written informed consent.
Measures
Family Caregiver Communication Tool
Family caregiver communication type was assessed using the Family Caregiver Communication Tool. The tool is a 10-item cognitive measure of communication patterns dependent upon the frequency, range, and congruence of communication within the patient's family (Wittenberg et al., Reference Wittenberg, Ferrell and Goldsmith2016). Congruent with family communication patterns theory, the 10-item tool has two subscales (conformity and conversation) and uses a response scale ranging from 0 (never) to 4 (frequently). The maximum range of scores for each subscale of the tool is from 0 to 20, with higher scores indicating a stronger communication pattern. To determine a caregiver type, the median score is used as the cutoff point between the two subscales (0–11 is low; 12–20 is high). The conversation and conformity subscales demonstrated sufficient internal consistency: α = 0.80 and α = 0.67, respectively.
Communication Perceived Self-Efficacy Scale
The degree to which caregivers feel they are able to communicate with the patient's physician was assessed using the Communication Perceived Self-Efficacy Scale (Capone and Petrillo, Reference Capone and Petrillo2014). The scale measures three dimensions of communication on a scale of 0 (not capable) to 5 (completely capable): ability to provide and collect information, ability to express concerns and doubts, and ability to verify information. Higher scores reflect greater perceived capability of communicating with physicians. The three subscales were reliable measures of self-efficacy related to seeking/giving information (α = 0.92), expressing concerns (α = 0.82), and verifying information (α = 0.85).
Caregiver Quality of Life
The Caregiver Quality of Life-Revised Index measures self-reported quality of life in four domains (emotional, social, financial, and physical) (Courtney et al., Reference Courtney, Demiris and Oliver2005). The instrument uses an 11-point scale anchored with 0 to indicate the lowest quality and 10 to indicate the highest quality. The maximums core for each dimension is 10, with a total maximum score of 40 that is derived by summing the four items. The internal consistency (α = 0.77) of the index was satisfactory.
Anxiety
Anxiety was measured with the Generalized Anxiety Disorder (GAD-2) questionnaire (Konstantakopoulos et al., Reference Konstantakopoulos, Sofianopoulou and Touloumi2013). The 2-item form asks participants about the frequency of feeling nervous and worrying over a two-week period. The answers are scored from 0 (not at all) to 3 (nearly every day). A score ≥3 on the GAD-2 detects stress disorders with acceptable levels sensitivity (70–86%) and specificity (81–83%). In the current sample, the GAD-2 was a reliable measure of anxiety (α = 0.84).
Results
A total of 220 caregivers completed the online survey. Full sample demographics are presented in Table 2. Overall, caregivers were providing care for patients with Type 2 Diabetes (40.0%), Alzheimer's disease or dementia (33.6%), cancer (21.8%), or chronic obstructive pulmonary disease (COPD) (3.2%). Participants’ caregiving experience ranged from 1 month to 26 years (M = 3.64 years; SD = 4.42 years). All four caregiver types were represented in the sample: Manager (54.5%), Partner (13.2%), Carrier (25.0%), and Lone (6.4%).
Table 2. Full sample demographics (N = 220)

A one-way ANOVA determined family caregiver communication types do differ in their perceived communication self-efficacy. The results revealed that there were significant differences in communication self-efficacy among family caregiver communication types (F(3,206) = 3.824, p = 0.011). Post hoc analyses find that Partner caregivers (M = 4.06, SD = 0.656) have higher perceived communication self-efficacy than Manager caregivers (M = 3.58, SD = 0.780) and Carrier caregivers (M = 3.46, SD = 0.826).
A similar trend emerged when we examined differences by caregiver type using each self-efficacy subscale. A series of one-way ANOVAs revealed significant differences in verifying information (F(3,211) = 3.54, p = 0.016) and providing/collecting information (F(3,211) = 4.00, p = 0.009). Partner caregivers report higher self-efficacy for providing/collecting information (M = 4.17) than Carrier (M = 3.54) and Manager (M = 3.58) caregivers. Partner caregivers also report more self-efficacy for information verifying (M = 4.17) than Carrier (M = 3.63) and Manager (M = 3.65) caregivers. Means and standard deviations by family caregiver communication type for each subscale are displayed in Table 3.
Table 3. Perceived communication self-efficacy mean scores by family caregiver type

To determine the relationship between communication self-efficacy and caregiver outcomes for all family caregiver communication types, we ran Pearson correlations for communication self-efficacy, quality of life, and anxiety per caregiver type. Pearson correlation coefficients are presented in Table 4. For all caregiver types, communication self-efficacy was not significantly correlated with anxiety, and the analysis revealed no correlation between communication self-efficacy and quality of life for Lone and Partner caregivers. A significant positive correlation was found among all three dimensions of communication self-efficacy and emotional QOL for Carrier caregivers; the ability to verify information was significantly associated with increased social QOL for these caregivers. We found a significant positive correlation between communication self-efficacy and social, financial, and physical QOL for Manager caregivers. The correlation between communication self-efficacy and emotional quality of life was not significant.
Table 4. Communication self-efficacy and caregiver outcomes correlations

* Statistically significant.
Discussion
To explore family caregiver communication with physicians, this study examined differences in perceived communication self-efficacy and how communication self-efficacy influences caregiver outcomes of anxiety and quality of life. Differences in communication self-efficacy do exist among the four caregiver communication types, providing further evidence that the Family Caregiver Communication Typology represents variance in caregiver communication behaviors. Partner caregivers garnered the highest perceived communication self-efficacy with physicians, specifically in providing, collecting, and verifying information. A somewhat surprising finding was that communication self-efficacy was not associated with anxiety in our sample. This finding appears to be contrary to previous research on caregiver anxiety (Teo et al., Reference Teo, Baid and Ozedemir2019) and warrants future investigation. However, our results suggest that a caregiver's ability to manage information and express concerns or doubts is more strongly associated with their perceptions of emotional, social, financial, and physical quality of life than feelings of nervousness, worry, or anxiety.
Study findings here demonstrate the influential role of family conversation and conformity on caregiver communication burden for interactions with physicians. The Partner caregiver represents families with high conversation patterns (broad range of topics and increased frequency of communication) and low conformity (adherence to family values and expectations). This open communication environment appears to increase caregivers’ self-efficacy communicating with physicians about information related to the care recipient's needs. These results suggest that open and collaborative communication environments can reduce communication burden for Partner caregivers. Previous research suggests that Partner caregivers experience lower psychological distress (Wittenberg et al., Reference Wittenberg, Kravits and Goldsmith2017b); however, in our study, communication self-efficacy was not correlated with quality of life for Partner caregivers as it was for Carrier and Manager caregivers. We posit that the negative effects of limited communication self-efficacy on quality of life may be buffered by Partner caregivers’ increased perception of support available to them by family and physicians. Recent research has found that high conversation a significant predictor perceived social support (Bevan et al., Reference Bevan, Urbanovich and Vahid2019). Coupled with our findings, this suggests that even in the event that Partner caregivers face challenges related to communication self-efficacy, they may not experience diminished quality of life because they perceive they have family and healthcare providers to rely on for support. Still, our results suggest that limited communication self-efficacy can result in diminished quality of life for caregivers whose families value conformity (Manager and Carrier), regardless of whether their family's conversation orientation.
Findings in this project are consonant with related research linking caregivers with low-expressive family types to lower levels of quality of life (Nissen et al., Reference Nissen, Trevino and Lange2016). Carrier caregivers (high conformity/low conversation) stem from low-expressive family systems, with similar findings here revealing that these caregivers have low emotional quality of life associated with perceived communication self-efficacy. Initial research on the four caregiver communication types found that Carrier caregivers feel least prepared for caregiving across the four types (Wittenberg et al., Reference Wittenberg, Kravits and Goldsmith2017b). Our study findings confirm that Carrier caregivers have the lowest perceived communication self-efficacy, which likely contributes to feeling unprepared. Caregiver perceptions of their own competency are directly related to psychological outcomes of caregivers (Teo et al., Reference Teo, Baid and Ozedemir2019). Of significance to the typology of caregivers, having a sense of mastery over caregiver tasks lowers risk of depression and is associated with lower anxiety (Teo et al., Reference Teo, Baid and Ozedemir2019). Taken together, these findings highlight the self-efficacy risks for the Carrier caregiver, emerging from a family environment of low conversation and high conformity, and likely in most need of interventions to address their sense of preparedness and support.
Caregiving preparedness, the ability to take care of both the physical and emotional needs of the care recipient (Vellone et al., Reference Vellone, Valentina and Durante2020), helps inform caregiver communication self-efficacy with physicians; this and similar studies help provide the linkages of knowledge to better understand the impact of communication in reducing barriers to palliative care and increasing preparedness for caregivers. Most unique to the study here is the consideration of the family communication pattern influence on caregiver–physician communication. The types examined in this work are meant to provide tailored care for the caregiver and support for providers who encounter caregivers and their unique needs. Individual caregiver needs will exceed the typology definitions here, and there is more to learn about caregiver communication needs and types across time and disease progress as caregiver burden evolves.
Although this study provides insight on family caregiver communication and caregiving outcomes, it was limited. First, the study was disproportionately comprised of three of the four caregiver types, with a limited sample of Lone caregivers. Although Lone caregivers are consistently the smallest type represented in every study on the Family Caregiver Communication Typology, a stronger representation of this group is needed. Second, the cross-sectional study design limits study conclusions about causality. Participants were self-identified family caregivers who participated online, limiting the generalizability of findings. However, the study sample was more culturally diverse than typical caregiving samples which are dominated by Caucasians (Hepburn and Siegel, Reference Hepburn and Siegel2020). Future research is needed to obtain a larger sample size to overcome these issues and explore additional communication variables as potential mediators.
Linking caregiver type communication patterns to self-efficacy and quality of life outcomes hold promise for the applied utility of the typology and its future integration into physician communication training. In a national survey, most physicians (88%) acknowledged seeing better outcomes and higher caregiver satisfaction (73%) when they share information with families (American Association of Retired Persons, 2019). While physician communication training primarily consists of skills for information giving or gathering (Boucher et al., Reference Boucher, Gemme and Dragomir2020), a recent systematic review of communication training programs for oncology providers found that there was no difference between trainees (physicians and nurses) who have had and have not had communication training (Moore et al., Reference Moore, Rivera and Bravo-Soto2018). There continues to be a need to develop evidence-based communication skills training programs for physicians (Back et al., Reference Back, Fromme and Meier2019). It has been noted that a relationship-centered communication skills curriculum in medical education is needed (England et al., Reference England, Howell and White2020) and the typology offers specific approaches for achieving skills such as "generating rapport" and "eliciting all concerns and summarizing"; the Family Caregiver Communication Typology demonstrates how communication should be tailored to varying communication styles of the caregiver.
Findings from this study demonstrate a need for physicians and other healthcare providers to learn more about family caregiver communication types in order to develop and implement family-centered care. Caregivers benefit from reflective discussions with physicians about the unique concerns of their caregiving situation, which does impact their sense of support and connectedness and increases their feeling of being prepared to deal with the day-to-day challenges with their care recipient (Slater et al., Reference Slater, Aoun and Hill2019). The caregiver's ability to find information and ask for help is a key factor in obtaining supportive resources for caregiving tasks (Northouse et al., Reference Northouse, Katapodi and Song2010; Ferrell and Wittenberg, Reference Ferrell and Wittenberg2017) and having additional resources lowers caregiver stress (Empeno et al., Reference Empeno, Raming and Irwin2011).
In palliative care, communication is a process that facilitates access and utilization of services, thus impacting the effect of health care for the patient, family, and healthcare provider (Hasson et al., Reference Hasson, Nicholson and Muldrew2020). Given that caregiver psychological outcomes are strongly associated with a patient's well-being, the development of interventions should target the caregiver and patient as a unit of care (Teo et al., Reference Teo, Baid and Ozedemir2019). Family caregiver, the care recipient, and supporting family members who are involved with providing care, and even family members on the periphery should all be included in future research to fully capitalize on the powerful resources of the family/support system engaged in the caregiving experience (Bevan et al., Reference Bevan, Urbanovich and Vahid2019). A family-centered approach improves communication and quality decision-making (Hsu et al., Reference Hsu, Gray and Murray2019) and findings here provide an initial evidence-base for use of the typology in shaping tailored family-centered care.
Multi-level communication strategies that address matters of health literacy, care team involvement, telecare outreach, and caregiver tracking and charting are needed to address the ways and needs of caregivers for understanding and navigating health communication and the healthcare system (Parker and Ratzan, Reference Parker and Ratzan2019). Caregiver communication patterns can be identified in order to guide healthcare providers’ communication with caregivers, guide the creation of interventions, inform caregivers themselves of their own patterns, and assist health systems in tailoring messages in specific ways for caregivers. Attention to the communication needs of caregivers, with specific attention to the family caregiver communication type, shows promise as a key component to a family-centered approach (Kokorelias et al., Reference Kokorelias, Gignac and Naglie2019).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.