


INTRODUCTION
Pediatric traumatic brain injury (TBI) affects a large number of children worldwide and causes a range of symptoms and impairments that vary according to pre-morbid factors and injury severity (Dewan et al., Reference Dewan, Mummareddy, Wellons and Bonfield2016). Even the mildest form of TBI, concussion, can lead to transient and sometimes persistent physical (e.g., dizziness), cognitive (e.g., confusion), emotional (e.g., irritability), and somatic (e.g., fatigue) changes known as post-concussive symptoms (PCS) (Zemek et al., Reference Zemek, Barrowman, Freedman, Gravel, Gagnon, McGahern and Osmond2013). In some cases, concussion can lead to psychological problems (Emery et al., Reference Durish, Yeates and Brooks2016) or cognitive deficits, though the latter often appear to be associated with pre-morbid problems (Babikian et al., Reference Babikian, Satz, Zaucha, Light, Lewis and Asarnow2011; Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018). Taken together, concussion can have a deleterious effect on a person’s quality of life (Fineblit et al., Reference Field, Collins, Lovell and Maroon2016). Research on the consequences of pediatric concussion has logically focused on identifying the negative effects of the condition and what factors are associated with poor outcome (Iverson et al., Reference Hung, Carroll, Cancelliere, Cote, Rumney, Keightley and Cassidy2017; Yeates, 2010). These studies are critical to understanding the gravity of these brain injuries, identifying children most at risk for impairments, and improving the management and treatment of concussion in children. Given these potentially detrimental consequences, however, it is easy to lose sight of the fact that most children who sustain concussion ultimately recover well, with few, if any, long-term effects (Carroll et al., Reference Carroll, Cassidy, Peloso, Borg, von Holst, Holm and Pepin2004). As such, there may be considerable value in focusing on the other face of concussion by investigating the positive outcomes and their predictors.
Course of Symptom, Cognitive, and Psychosocial Recovery
The results of a large-scale, prospective cohort study of persistent PCS (PPCS) suggested that approximately 30% of children between 5 and 18 years continue to experience symptoms 1 month after their injury (Zemek et al., Reference Yeates2016). Conversely, these data can be taken to highlight that 70% of children have relatively good outcome after 1 month and are on their way to full recovery. Prolonged symptom duration is increasingly being attributed to pre-morbid factors (Barlow, Reference Barlow2016), and substantial evidence suggests that significant cognitive and motor impairments are relatively rare and do not carry over in the mid to long term (Anderson et al., Reference Anderson, Catroppa, Morse, Haritou and Rosenfeld2005; Asarnow et al., Reference Asarnow, Satz, Light, Zaucha, Lewis, McCleary, Broman and Michel1995; Babikian et al., Reference Babikian, Satz, Zaucha, Light, Lewis and Asarnow2011; Bijur & Haslum, Reference Bijur, Haslum, Broman and Michel1995; Brooks et al., Reference Brooks, McKay, Mrazik, Barlow, Meeuwisse and Emery2013; Fay et al., Reference Emery, Barlow, Brooks, Max, Villavicencio-Requis, Gnanakumar, Robertson, Schneider and Yeates1993; Hung et al., Reference Huber2014; Rieger et al., 2013; Studer et al., Reference Steindel2014; Yeates, 2010). Using a statistically derived definition, Beauchamp and colleagues (Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018) found that only about 10% of children who sustain concussion exhibit neuropsychological impairment 1 month post-injury. The same study also found that cognitive difficulties were predicted by pre-morbid factors; however, performance on acute tests of cognition also significantly predicted cognitive difficulties at 4 weeks post-concussion, and acute symptoms predicted cognitive difficulties 12 weeks after the injury, suggesting that the neuropsychological outcome in children and adolescents is not solely attributable to the presence of pre-injury problems. There is also some evidence for psychological, social, and behavioral disturbance after pediatric concussion (Catroppa et al., Reference Catroppa, Hearps, Crossley, Yeates, Beauchamp, Fusella and Anderson2017; Taylor et al., Reference Sullivan, Kempe, Edmed and Bonanno2015); however, at least three studies, including two systematic reviews, indicate that these problems rarely persist beyond the acute/subacute period and prognosis in these domains is generally good (Emery et al., Reference Durish, Yeates and Brooks2016; Keightley et al., Reference Iverson, Gardner, Terry, Ponsford, Sills, Broshek and Solomon2014; Plourde et al., Reference Petersen, Scherwath, Fink and Koch2018). Together, these findings suggest that a preponderance of children recover well from concussion.
Quality of Life after Pediatric Concussion
A disruption of one or more domains of functioning after concussion may result in an overall diminution of decrease in children’s quality of life, though the proportion of children affected is not clear. Children with PPCS reported poorer quality of life compared with those who recovered from their injury (Moran et al., Reference Moons, Donders, Stijnen and Harrell2012; Novak et al., Reference Nalder, Hartman, Hunt and King2016; Russell et al., Reference Rubin2017); however, the evidence as to whether those deemed to have recovered clinically also experience reduced quality of life is contradictory (Novak et al., Reference Nalder, Hartman, Hunt and King2016; Russell et al., Reference Rubin2017). Some data suggest that poorer quality of life is present regardless of injury severity (DeMatteo et al., Reference DeMatteo, Hanna, Yousefi-Nooraie, Lin, Mahoney, Law and McCauley2014) and lasts between 3 and 6 months post-injury (Brown et al., Reference Brown, Kenardy, Chandler, Anderson, McKinlay and Le Brocque2016). However, other research suggests that most children who sustain concussion have adequate or good quality of life. For example, several studies indicated that the quality of life of children with mild TBI is not affected in the first 3 months post-injury (Petersen et al., Reference O’Neill, Acherson, Johnston, Wilkins, Brown, Novack and Schwebel2008), nor up to 24 months post-injury (Rivara et al., Reference Rieger, Lewandowski, Callahan, Spenceley, Truckenmiller, Gathje and Miller2011).
Wellness and Positive Outcome after TBI
In light of the overall good prognosis for a majority of children who sustain concussion, it is relevant to consider the results of a small number of studies that have looked at positive outcomes after TBI. For example, a systematic review by Sullivan and colleagues (Reference Studer, Goeggel Simonetti, Joeris, Margelisch, Steinlin, Roebers and Heinks2016) indicated that psychological resilience, generally defined as a modifiable, dynamic, and positive adaptation process in the context of significant adversity (Luthar et al., Reference Lovell, Collins, Podell, Powell and Maroon2000; Sullivan et al., Reference Studer, Goeggel Simonetti, Joeris, Margelisch, Steinlin, Roebers and Heinks2016), is associated with better outcome after TBI in adults (e.g., better quality of life, less fatigue and stress, fewer depressive symptoms, fewer PCS) (Losoi et al., Reference Little and Rubin2015; McCauley et al., Reference McCauley, Wilde, Anderson, Bedell, Beers, Campbell and Yeates2013; Merritt et al., Reference McNally, Bangert, Dietrich, Nuss, Rusin, Wright and Yeates2015). The presence of other positive character strengths, such as coping, courage, and hope, has also been found to contribute to better outcomes after TBI in adults (Belanger et al., Reference Belanger, Barwick, Kip, Kretzmer and Vanderploeg2013; Hanks et al., Reference Goreth and Palokas2014). Using an alternative approach to positive outcomes, Braden and colleagues (Reference Braden, Cuthbert, Brenner, Hawley, Morey, Newman and Harrison-Felix2012) examined health status, health-related self-efficacy, health-promoting behaviors, and subjective wellbeing in adults with moderate–severe TBI and found that the levels of these indicators are similar to those in other disability groups, suggesting that health and wellbeing can reflect optimal outcome after TBI. One study to date that has focused on resilience in pediatric concussion and found that psychological resilience (as defined by factors related to personal competence, tenacity, tolerance of negative affect, positive acceptance of change, control, and spiritual influences) was a significant predictor of PPCS in children aged 8–18 years (Durish et al., Reference Di Battista, Soo, Catroppa and Anderson2018).
Many of the constructs referred to in relation to the positive outcomes of brain injury (e.g., resilience, character strengths, quality of life, healthy behaviors) can be conceptualized under the broader umbrella of wellness, defined by the World Health Organization as a state of complete physical, mental, and social wellbeing, and not merely the absence of disease or infirmity (WHO, Reference White, Royston and Wood1946). Some conceptions of wellness even go beyond the notion of minimal recovery from injury, referring to a state of optimal functioning. In this sense, the National Wellness Institute posits that wellness is a dynamic process that strives towards individual achievement of full potential (Hettler, Reference Hawley and Joseph1976). Applying this to the domain of TBI, Hawley and Joseph (Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde2008) suggested that wellness may not simply be a return to status quo, but that recovery may actually involve going beyond pre-morbid levels of functioning.
The positive indicators of outcome, and wellness more specifically, have received limited attention in relation to TBI and are nearly absent from the pediatric TBI literature. The few studies that have documented wellness after TBI have done so in participants with more severe injuries, despite mTBI/concussion representing 90% of the TBI population and thus an important financial and societal burden. There is limited information available on the predictors of wellness after pediatric TBI, although such data could be valuable in determining which variables predict good prognosis and in identifying specific loci of intervention for improving positive outcomes in those at risk for post-concussion difficulties.
OBJECTIVES
The aim of this study was to determine what pre-existing, demographic, and injury factors are predictive of wellness after pediatric concussion. In accordance with existing notions (Bezner & Hunter, Reference Bezner and Hunter2001; Diener, Reference Diener1984; WHO, Reference White, Royston and Wood1946), wellness is defined not only by the absence of PPCS and cognitive difficulties, but also by the presence of a subjective, global, positive indicator, namely good quality of life. A comprehensive predictive model was tested in a large sample of children and adolescents who sustained concussion and were assessed acutely in a pediatric emergency department and followed up 1 and 3 months post-injury. We hypothesized that a combination of pre-existing, demographic, and injury factors would contribute to wellness.
METHODS
Design
This was a planned substudy of a larger prospective, longitudinal, multicenter cohort study conducted among nine university-affiliated hospitals in 2013–2015 (The 5P Study). The full study protocol and details on the complete sample are provided elsewhere (Zemek et al., Reference Zemek, Farion, Sampson and McGahern2013b). Here, we summarize the methods and present the data pertaining to the participants who enrolled into the neuropsychological follow-up portion of the larger study. The neuropsychological substudy was offered in the ED at four of the nine study sites at the time of enrollment in the parent study and was conducted at 4 and 12 weeks post-injury.
Participants
Participants in the neuropsychological substudy were children (N = 311, aged 6–18 years, 35% female) who presented to the EDs of four tertiary pediatric hospitals (Children’s Hospital of Eastern Ontario, Toronto Sick Kids Hospital, Montreal Children’s Hospital, Ste-Justine Hospital). Children were eligible to participate in the larger parent study if they were aged between 5 years and 17 years + 11 months at the time of presentation to the ED, if they sustained a concussion as defined by Zurich consensus statement (McCrory et al., Reference McCauley, Wilde, Miller, Frisby, Garza, Varghese and McCarthy2009), if the concussion occurred within the preceding 48 hr, and if they were proficient in English or French. The following exclusion criteria were applied at recruitment to determine eligibility: (a) Glasgow Coma Scale score <13; (b) abnormality on structural head CT or MRI (if performed clinically); (c) multisystem injury requiring hospitalization, operating room, or procedural sedation; (d) neurosurgical intervention, intubation, or ICU admission required; (e) intoxication at the time of ED presentation as per clinical judgment; (f) absence of traumatic injury as a primary event; (g) severe pre-existing neurological developmental delay resulting in communication difficulties; (h) insurmountable language barrier; (i) inability to follow up by phone or electronic mail; (j) previously enrolled in the same study (to ensure individuals who sustained another concussion during the course of the longitudinal study were not re-enrolled once they had completed follow-up).
PROCEDURE
ED Enrolment and Screening
The study was approved by the local research ethics committees of the four participating sites. Written informed consent was obtained from the participants and/or their parents prior to participation and verbal assent was obtained for all participants. The data were obtained in compliance with the Helsinki Declaration. Information and details regarding participants’ demographics, past medical and developmental history, injury characteristics, and acute symptoms were collected at enrolment by a research assistant or nurse, using the validated Acute Concussion Evaluation inventory in the ED (Gioia et al., Reference Fineblit, Selci, Loewen, Ellis and Russell2008). Information regarding past medical and developmental history was obtained via parent report and included questions regarding the presence or absence of a history of migraine, mood, sleep or developmental problems, such as attention-deficit hyperactivity disorder (ADHD) or learning disabilities. All data were acquired and managed in real time using the Research Electronic Data Capture (REDCap; Harris et al., Reference Harrell2009) application. Depending on their preferences, enrolled patients/parents completed follow-up questionnaires and surveys either electronically through REDCap or via telephone. Participants received email reminders 24 hr preceding each survey deadline; research assistants telephoned non-responders up to five times offering standardized verbal surveys.
Post-concussive Symptoms
Physical, cognitive, emotional, and sleep-related symptoms were reported acutely in the ED by parents completing the 20-item Post-Concussion Symptom Inventory (PCSI; Gioia et al., Reference Gioia, Collins and Isquith2009; Sady et al., Reference Russell, Selci, Chu, Fineblit, Ritchie and Ellis2014), which included providing a baseline estimate corresponding to “pre-injury” ratings of the symptoms. The PCSI was then completed by participants at all the broader study follow-up time points (1, 2, 4, 8, and 12 weeks post-concussion), and these also included a baseline rating. Thus, PCSI delta scores were used for each time point (i.e., change in PCSI between a given time point’s baseline and the actual time point rating). The acute ED ratings (delta scores) were used as a predictor variable (i.e., PCS ratings from the ED minus pre-injury PCS ratings assessed in the ED), whereas the 4- (i.e., PCS ratings at 4 weeks minus pre-injury symptoms assessed at 4 weeks) and 12-week ratings (i.e., PCS ratings at 12 weeks minus pre-injury symptoms assessed at 12 weeks) were used as part of the definition for the main outcome variable (wellness).
Acute Balance and Cognitive Screening
The Standardized Assessment of Concussion–Child Version (SAC-C) was administered in the ED as part of the Child-Sport Concussion Assessment Tool (McCrory et al., Reference McCrory, Meeuwisse, Johnston, Dvorak, Aubry, Molloy and Cantu2013). The SAC-C is a 30-point objective assessment of acute cognition comprising four indices: orientation (4 points), immediate verbal memory (15 points), concentration (6 points), and delayed verbal recall (5 points). The modified Balance Error Scoring System (BESS), a brief static postural stability assessment tool to measure performance on double-leg stance and tandem stance conditions, was also administered in the ED.
Neuropsychological Assessment
The neuropsychological test battery performed at 4 and 12 weeks post-injury included either eight (6–7-year-olds) or nine (≥8-year-olds) standardized scores (either z-, T-, or standard scores) covering intellectual functioning, attention, working memory, executive functioning, verbal memory, processing speed, and psychomotor abilities. Full details of the neuropsychological protocol are published elsewhere (Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018).
Quality of Life
Quality of life was documented at 4 and 12 weeks post-injury using the Pediatric Quality of Life Inventory (PedsQL) (Desai et al., Reference Desai, Zhou, Stanford, Haaland, Varni and Mangione-Smith2014). The generic version of the questionnaire measures the core dimensions of health in terms of physical (eight items), emotional (five items), social (five items), and school (five items) functioning, providing a total score representing a transformation of the sum of scores on a 0–100 range. Participants ≥8 years completed the self-report version, and a parent proxy version was used for participants 6–7 years old.
STATISTICAL ANALYSES
Definitions
Wellness
The criteria used to define wellness in the analyses were based on existing conceptualizations of wellness (Diener, Reference Diener1984; WHO, Reference White, Royston and Wood1946), which require the absence of impairment in addition to the presence of a positive outcome. Applying this to the context of concussion and to the data available for this cohort, it was defined as:
Wellness = absence of PPCS + absence of cognitive inefficiency + presence of optimal quality of life
To reflect the notion that wellness describes a state of optimal outcome, participants were classified as “less well” if any of the above criteria were unmet. For descriptive purposes, if any one of the three definition components was missing and all others were “well,” the participant’s data were not used (N = 270 at 4 weeks post-injury and N = 180 at 12 weeks post-injury). The three components were combined to represent the construct of wellness, and their respective cut-off scores were defined as follows.
Persistent Post-concussive Symptoms
PPCS was the primary outcome of the larger cohort study and was defined according to the International Statistical Classification of Disease and Related Health Problems, Tenth Revision (Steindel, Reference Seiger, Goldwater and Deibert2010) as the persistence of at least three symptoms compared with the state of being prior to the injury. An individual symptom was defined as “a positive difference between the current PCSI minus the perceived preinjury symptom rating” (Zemek et al., Reference Zemek, Farion, Sampson and McGahern2013b). To be classified as having no PCS, at least 85% of the PCSI items had to be completed.
Cognitive Inefficiency
Cognitive inefficiency was defined based on an adaptation of the published, statistically derived Neuropsychological Impairment Rule (Beauchamp et al., Reference Beauchamp, Brooks, Barrowman, Aglipay, Keightley, Anderson, Yeates, Osmond and Zemek2015), which determines the presence of neuropsychological impairment based on an individual’s performance on a large battery of neuropsychological measures. To fully capture more subtle cognitive changes typical of concussion in the current cohort, a less conservative approach used by Beauchamp et al. (Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018) was applied here. Thus, cognitive inefficiency was considered to be present when an individual performed 1.0 SD below the mean on two or more neuropsychological measures. To be classified, participants had to have completed at least six of the battery subtests.
Quality of Life
The presence of optimal quality of life was defined as a score at or above the population means reported by Varni and colleagues (Reference Varni and Burwinkle2003) for the same measure. Age-appropriate norms were used for 6–7, 8–12, and 13–18-year-olds.
Modeling Strategy
To determine the predictors of wellness following concussion, we derived a comprehensive multivariable logistic regression model that incorporated data at both follow-up time points (i.e., wellness at 4 and 12 weeks treated as repeated outcomes, represented in separate rows in the dataset). Since previous research is limited on the predictors of wellness following concussion, we elected an “exploratory” modeling strategy that enabled the consideration and testing of a broad range of candidate predictors, but also the opportunity to add flexibility to model specifications by accommodating complex (e.g. non-linear) predictor–outcome relations. To this end, the model strategy had three main components: (1) an initial a priori selection of candidate predictors to be assessed within the confines of the sample size, (2) multiple imputation of missing data on candidate predictors and model outcomes, and (3) implementation of a model fitting procedure that involves a conservative backward elimination step and subsequent refitting where flexible splines were incorporated in the regression.
Selection of Candidate Predictive Factors
The a priori selection of candidate predictive factors (i.e., independent variables) considered conceptual relevance, hypothesized associations with outcome based on study investigators’ clinical experience, and data features [e.g., variable completeness (i.e., <15% missing values), presence of meaningful score variability, no significant correlation [i.e., r<0.7] with other predictor candidates]. Additional considerations ensured a sufficiently broad coverage of domains, encompassing sociodemographic factors, patient history, and injury mechanism, as well as clinical presentation (e.g., scores from the SAC and PCSI collected acutely in the ED), within the constraints of the available sample size. Specifically, our approach was to keep within an approximate 10:1 event-per-variable ratio throughout the entire modeling process. The 20 candidate variables ultimately selected included: time (4 or 12 weeks), site (four levels, reference set to the largest level; n = 103), age (continuous), sex (males vs. females), maximum symptom duration of previous concussion (five levels: no previous concussion to longer than 8 weeks symptom duration), personal history of migraine (yes/no), history of developmental problem (yes/no: learning disability, ADHD, other developmental problem), history of mood/sleep disorders (yes/no), duration of lost consciousness (continuous), injury mechanism (sports related vs. others), post-traumatic amnesia (yes/no), acute ED PCSI physical factor score (range 0–6), acute ED PCSI fatigue factor score (range 0–6), acute ED PCSI emotional factor score (range 0–6), acute ED PCSI cognitive factor score (range 0–6), SAC orientation score (range 0–4), SAC immediate memory score (range 0–15), SAC delayed recall score (range 0–5), SAC concentration score (range 0–6), and BESS tandem stance score (range 0–7). Summary statistics of these variables (e.g., median, IQR, range, percentage) as well as additional descriptive variables of interest are provided in Table 1.
Table 1 Participants’ demographic, pre-morbid, and clinical characteristics

Notes: aIncludes developmental disorders, ADHD, and learning disabilities (e.g., dyslexia, dyscalculia). bThe seizure variable was excluded from modeling because there were too few cases. cThis was dichotomized to sports/recreational vs. other for modeling. dIncludes amnesia before and/or after the event, but only amnesia after the event was considered in modeling to reflect ongoing impairments in memory formation. eDouble-leg stance was not considered for modeling because of high correlation (r > 0.6) with tandem stance.
Abbreviations: ED = emergency department; IQR = interquartile range; MVC = motor vehicle collision; PCSI = Post-Concussion Symptom Inventory; SAC = Standardized Assessment of Concussion.
Multiple Imputation
To add robustness in model fitting, we performed an initial multiple imputation of missing data for all relevant variables (i.e., all candidate predictors and outcomes with any missing values) using a chained equations approach (Little & Rubin, Reference Lee, Yang, Lee and Teng2002; Moons et al., Reference Merritt, Lange and French2006; van Buuren, Reference Taylor, Orchinik, Minich, Dietrich, Nuss, Wright and Yeates2012; van Buuren et al., Reference van Buuren2006). Through this process, “educated guesses” of missing data were generated on a variable-by-variable basis based on the interrelationships among the variables included in the imputation model. The chained equations approach affords unique univariate imputation techniques to be employed according to the type of target variable being imputed. Specifically, the predictive mean matching strategy was used for imputing missing values from numeric variables (continuous or ordinal), and logistic regression was the basis for imputing missing values for categorical variables. At the end, multiple sets of imputed data were generated to help capture the variability/uncertainty of the imputed values. To optimize imputation performance, we initially considered a comprehensive set of 169 variables collected from the parent study as potential auxiliary variables for inclusion in the imputation model. Of these, 62 were ultimately selected. As with our candidate predictors, these auxiliary variables encompassed a wide range of factors, including constituent items of various scales common in concussion research (e.g., specific items from the PCSI, PedsQL, and SAC; scores from specific neuropsychological tests and balance tests), with the key condition being that, to be selected, they must be reasonably well completed (i.e., >50% data available) among the subset of observations that had incomplete data on any variables intended for modeling (i.e., candidate predictors or model outcomes). Thus, combining outcome measures and 19 candidate predictors, a comprehensive 83-variable imputation model was derived. In accordance with the current recommendations (I.R. White et al., Reference White2011), the imputation procedure was repeated seven times to match the percentage of patients with incomplete data (on intended model covariates or outcome) in the sample (6.8%). This created seven unique, imputed datasets available for further analysis. Notably, no imputation was performed on missing data due to non-participation. The imputed dataset was constructed based only on the eligible observations of individuals who participated at a given time point. Thus, the amount of missing data among those who did participate was only 17/287 (5.9%) at week 4 and 16/196 (8.2%) at week 12.
Model Fitting Procedure
After multiple imputations, a preliminary logistic regression model with all 19 candidate predictors was fitted for each of the seven imputed datasets. To pool the results, parameter estimates were then averaged across all models and imputation-adjusted variance estimates were computed according to Rubin’s rule (Rubin, Reference Rivara, Koepsell, Wang, Temkin, Dorsch, Vavilala and Jaffe2004). To correct for intra-subject correlation due to clustering (i.e., repeated outcomes at different weeks may be provided by the same participant), standard errors of model parameters were further adjusted using the Huber–White method (Huber, Reference Hettler1967; H. White, Reference Waber, Boiselle, Forbes, Girard and Sideridis1980). Then, a conservative backward stepwise elimination was performed to retain the variables that contributed most to outcome prediction using a cut-off of p > 0.25 (for removal). The acceptable variance inflation factor for each retained covariate (<5) was verified at this step. To allow for the exploration of the nature of the predictor–outcome relationship (e.g., non-linearity), as a final step the model was refitted by incorporating flexible restricted cubic spline functions with three knots at 0.1, 0.5, and 0.9 quantiles (Harrell, Reference Hanlon, Demery, Martinovich and Kelly2015) for all continuous predictors that remained in the model, and the same corrections were re-applied to the estimated standard errors as above to arrive at the final multivariable model. Interaction terms were not considered, as priority for degree-of-freedom spending was given to the testing of a more comprehensive set of individual predictors and also to exploring the potential non-linearity effects.
Contributions of individual predictors were summarized by an overall Wald chi-square statistic, which provides an indication of the relative importance of model predictors. Adjusted odds ratios and p-values were also estimated based on specific contrast hypotheses. For each continuous predictor (with associated spline terms), a multiple degree-of-freedom joint test of the predictor and associated non-linear terms was performed. Estimated adjusted odds ratios were based on a contrast of the 25th vs. 75th quantile values. For categorical predictors, a contrast of all predictor levels against the reference level was performed. Discrimination performance of the model was assessed by the c-statistic (averaged from models derived from each imputed dataset). All analyses were performed using R version 3.3.2 (rms, mice packages; R Core Team, Reference Plourde, Yeates and Brooks2016).
RESULTS
Final Sample Characteristics
The recruitment flowchart is presented in Figure 1, and participant characteristics are described in Table 1. As reported elsewhere (Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018), the participants enrolled in the neuropsychological follow-up tended to be slightly younger, were more likely to have had a previous concussion, had a greater prevalence of a family history of migraine, and displayed greater PCS at 4 and 12 weeks post-injury than those in the larger parent study. There was no significant difference in PCSI between children who participated in the 4-week post-injury follow-up and those who completed both the 4- and 12-week follow-up (frequency of PPCS between groups: p = 0.776; all PCSI factor score differences between p = 0.14 and 0.69). Children who completed week 4 (but not week 12) tended to be slightly older (M = 12.35; SD = 3.07 years) than those who completed both time points (M = 11.36; SD = 3.08) or only the week 12 time point (M = 11.04; SD = 2.91 years) (p = 0.02).

Fig. 1 Flowchart of recruitment for the main study and those enrolled in the neuropsychological follow-up in four of the study sites.
Outcome Distribution for Wellness Variables
Table 2 presents the outcome distribution for the main study variables. This table is based on unimputed data so as to describe the actual number of cases that were classified according to the wellness definition. Of the 270 participants who had completed wellness data, 112/270 (41.5%) were defined as well at 4 weeks post-injury, and the rate increased to 94/180 (52.2%) at 12 weeks post-injury (difference 10.7%; 95% CI = 2–20%). Of the 172 individuals who participated at both time points, 151 had (non-imputed) wellness outcome values at both time points. Among these 151 participants, 60 were classified as “well” at week 4, of which 13 (20%) were less well at week 12. Among the 115 subjects who participated only at week 4 (missing at week 12), 45 (39.1%) were “well” at week 4, 60 (52.2%) were less well at week 4, and 10 (8.7%) were indeterminate due to missing component score(s).
Table 2 Outcome distribution of wellness variables

Note: Frequencies represent raw, unimputed cases.
Abbreviation: PCS = post-concussion symptoms.
Table 3 presents the correlations between the wellness sub-criteria (cognitive inefficiency, PPCS, quality of life) and the overall wellness score, and Table 4 shows the frequency distribution for each of the wellness sub-criteria, and combinations thereof, in relation to the classification of “less well” at 4 and 12 weeks post-injury.
Table 3 Correlations between the variables comprising wellness and the wellness composite

Abbreviations: PPCS = persistent post-concussion symptoms; QOL = quality of life.
Table 4 Distribution of how the three wellness components contributed to a classification of “less well” (absence of wellness) at 4 and 12 weeks post-injury

Abbreviations: PPCS = persistent post-concussion symptoms; QOL = quality of life.
Wellness Prediction Model
Table 5 presents the results of the logistic regression predicting wellness, including the contribution of 13 predictor variables. The overall model was significant (χ2 = 85.92, df = 21, p < 0.001) and five variables were found to have a significant effect on the outcome (wellness): age, mechanism of injury, history of developmental problem, acute ED PCSI physical symptoms, and SAC concentration. Sex and history of mood/sleep disorders approached significance. The resulting c-statistic was modest (c = 0.730), but satisfactory (i.e., >0.70).
Table 5 Wald chi-square statistic from model fit for logistic regression predicting wellness after pediatric concussion

Notes: Bold implies significant predictors at p < .05.
Abbreviations: PCSI = Post-Concussion Symptom Inventory; SAC = Standardized Assessment of Concussion.
The relations of predictor variables with wellness are illustrated in Figure 2, and the model contrasts and odds ratios are presented in Table 6. Older participants and those who reported a history of developmental problems (ADHD or learning difficulties) were less likely to be well. Those who sustained sports/recreational injuries and those who had higher scores on the SAC concentration subscale were more likely to be well. Female sex and the presence of a history of mood or sleep disorders were again just at the cut-off for significance and were associated with a greater likelihood of not meeting the wellness criteria (p = 0.054 and 0.050, respectively). Although the overall Wald chi-square statistic was not significant in the previous analysis, acute ED ratings of PCSI cognitive symptoms emerged in the odd ratios as a significant predictor.
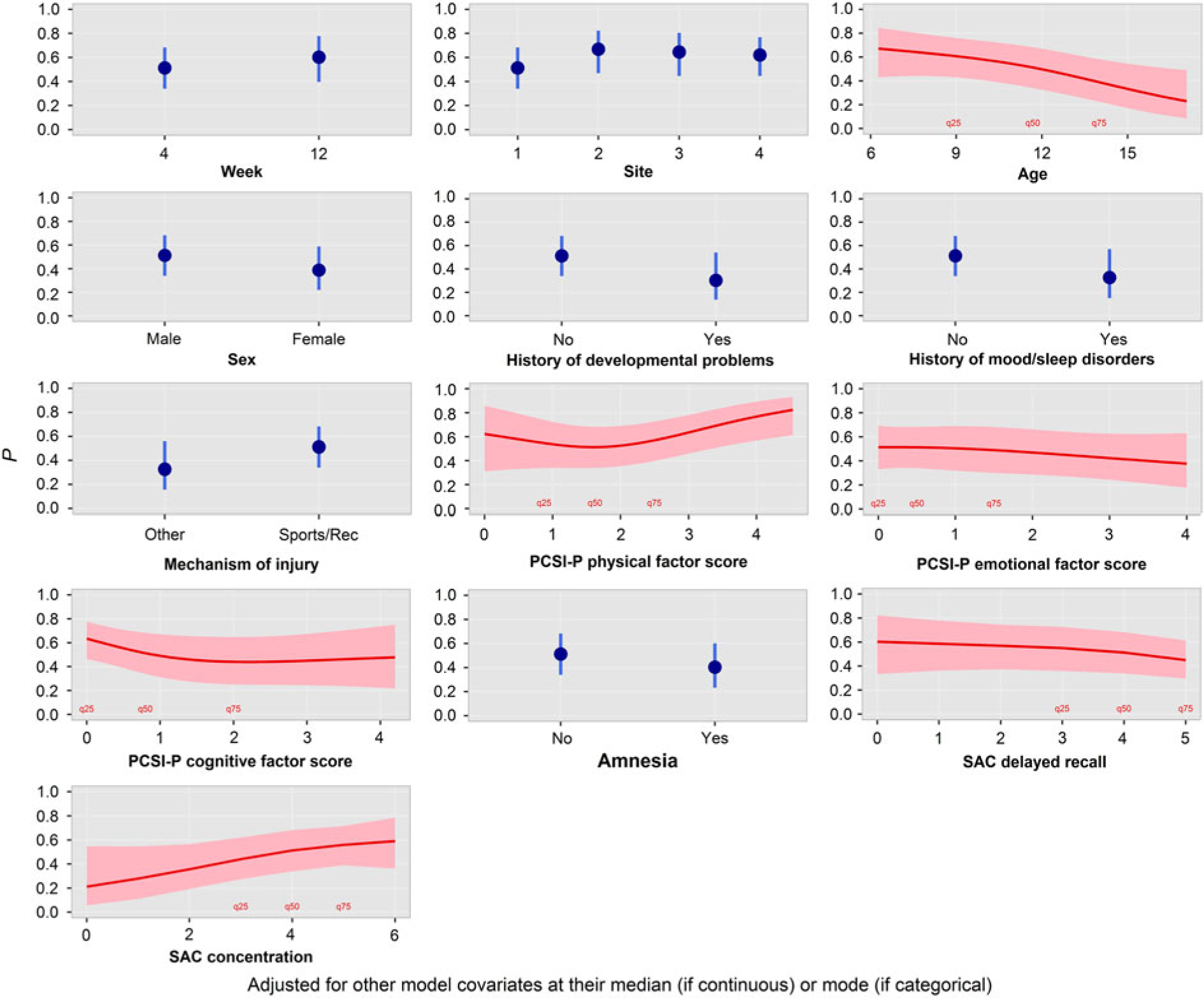
Fig. 2 Partial effect plots illustrating the relation of each predictor variable with the wellness outcome.
Table 6 Adjusted odds ratios for wellness predictor variables

Notes: Bold indicates significant predictors at p < .05. Range is 75th vs. 25th quantiles for continuous/ordinal variables.
Abbreviations: Hx = history; OR = odds ratio; PCSI = Post-Concussion Symptom Inventory; SAC = Standardized Assessment of Concussion; SE = standard error.
DISCUSSION
This study aimed to determine what factors are associated with the probability of being well after a childhood concussion, where “wellness” was defined as the absence of PPCS or cognitive difficulties combined with optimal quality of life at 4 and 12 weeks post-injury. Of the children who had sufficient data to determine wellness, 41.5% were considered to be well at 4 weeks, and this increased, though not significantly, to just over half the group (52.2%) at 12 weeks post-injury. The individual components of wellness (cognitive inefficiency, PPCS, quality of life) were all moderately to strongly correlated with the global outcome and, in isolation, had similar frequency distributions in children classified as less well. At both 4 and 12 weeks post-injury, the most common reason for being less well was a combination of PPCS and lower quality of life (37% and 31%). Given the paucity of research focusing on wellness after TBI and the novel approach used here, it is premature to determine whether this is a typical rate of wellness after concussion and whether it is comparable to other patient cohorts.
Various factors related to pre-morbid status, demographics, and injury were predictive of wellness. In particular, younger children (in the 6–8-year range) were more likely to be considered well after injury than older children. This is in keeping with other studies and reviews suggesting that age is associated with outcome after mild TBI. This body of evidence generally indicates that older children have an increased risk of PPCS (Babcock et al., Reference Babcock, Byczkowski, Wade, Ho, Mookerjee and Bazarian2013; Field et al., Reference Fay, Jaffe, Polissar, Liao, Martin, Shurtleff and Winn2003; Iverson et al., Reference Hung, Carroll, Cancelliere, Cote, Rumney, Keightley and Cassidy2017; Scopaz & Hatzenbuehler, Reference Sady, Vaughan and Gioia2013; Zemek et al., Reference Zemek, Barrowman, Freedman, Gravel, Gagnon, McGahern and Osmond2013a, Reference Yeates2016), although some studies suggest that this effect may be related to mechanisms of injury in different age groups (e.g., adolescents more likely to be involved in more severe mechanisms) or to measurement bias (e.g., adolescents better able to recognize and report symptoms). The wellness indicators used here combined three outcome domains (symptoms, cognition, quality of life), which may be differentially associated with age, making the results difficult to compare with previous work. Nonetheless, the current findings suggest that when these three domains are considered together, among children aged 6–18 years, younger children with concussion are more likely to be well 1 and 3 months post-injury.
The absence of pre-injury problems (mainly learning disabilities and ADHD, but also mood and sleep disorders) also emerged as a significant predictor of being well. This result aligns with previous work highlighting the significance of pre-morbid problems in neuropsychological prognosis after concussion (Babikian et al., Reference Babikian, McArthur and Asarnow2013; Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018; see also Goreth & Palokas, Reference Gioia, Schneider, Vaughan and Isquith2018). A direct association between diagnosis of a learning disability (Balazs et al., Reference Balazs, Miklosi, Toro and Nagy-Varga2016; Waber et al., Reference Varni, Burwinkle, Seid and Skarr2019) or ADHD (Klassen et al., Reference Keightley, Cote, Rumney, Hung, Carroll, Cancelliere and Cassidy2004; Lee et al., Reference Klassen, Miller and Fine2019; Varni & Burwinkle, Reference van Buuren, Brand, Groothuis-Oudshoorn and Rubin2006) and reduced quality of life has also been reported. Thus, participants with these pre-injury diagnoses may have experienced poorer quality of life and thus an increased likelihood of not meeting the criteria for wellness even before their injury, and this could either have been maintained or compounded by concussion through a double-hazard effect. However, it is not possible to objectively ascertain whether quality of life was lower in some participants before they sustained their injury, as the design did not include a pre-injury (retrospective) measure of this domain. Notably, a history of learning disability, ADHD, or other developmental disorders did not emerge as a predictor in this sample when PCS was studied in isolation (Zemek et al., Reference Yeates2016), suggesting that this particular predictor is especially relevant to cognitive functioning or quality of life.
Children who scored higher on the SAC concentration subtest were more likely to be well after concussion. This test of working memory assesses performance based on backward digit span and recitation of the months of the year in reverse order. To our knowledge, only two other studies (Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018; O’Neill et al., Reference Novak, Aglipay, Barrowman, Yeates, Beauchamp, Gravel and Zemek2015) have focused on the predictive utility of this measure in concussion, despite its inclusion in the widely used Sports Concussion Assessment Tool (Davis et al., Reference Davis, Purcell, Schneider, Yeates, Gioia, Anderson and Kutcher2017). A previous study in the same sample found that the SAC immediate memory and concentration subtests were predictive of better neuropsychological performance at 4 and 12 weeks post-injury (Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018). The current findings suggest that intact acute working memory may be especially useful in foretelling wellness after pediatric concussion, although these findings need to be replicated in independent samples. Future work could also look into identifying a level or cut-off for the SAC concentration subtest that could provide clinicians with a marker for prognosis and thereby facilitate referral forfollow-up.
Past work focusing on the negative effects of concussion have shown an effect of sex as a risk factor for poor outcome, with female sex predicting overall risk of concussion and increased PCS, for example (McNally et al., Reference McCrory, Meeuwisse, Aubry, Cantu, Dvoøák, Echemendia and Turner2013; Scopaz & Hatzenbuehler, Reference Sady, Vaughan and Gioia2013; Zemek et al., Reference Yeates2016). The findings of the current study were inconclusive in regard to the association between sex and wellness, though the results did align in the expected direction; males were more likely to be designated as being well when symptoms, cognition, and quality of life were considered jointly.
Despite it being used as a common measure of PCS after concussion (McCauley et al., Reference Luthar, Cicchetti and Becker2012), no components of the acute ED ratings of PCSI unambiguously emerged as being especially useful in predicting wellness. The PCSI physical factor score, which taps into symptoms such as dizziness, balance problems, sensory sensitivity, and nausea, was initially identified as a predictor based on the Wald chi-square statistic, but the relation was not in the expected direction (greater presence of physical symptoms predicted wellness). The exploration of the partial effect plots indicated that most participants in the sample fell in the 0–2.5 range, which showed little effect. The estimated effects of acute ED ratings of PCSI physical scores at more extreme ranges (e.g., >3.5) were based on fewer participants, suggesting that the results were driven by a few influential scores. The PCSI physical factor score was no longer predictive when the adjusted odds ratios were considered. The exploration of the partial effect plot for the PCSI cognitive factor score, which taps into symptoms of impaired concentration, memory, and speed of processing, showed a borderline effect in the 25–75 percentile range and the results were in the expected direction (fewer cognitive symptoms associated with being well); however, there was no strong evidence for an overall effect, given that the Wald chi-square statistic was not significant (p = .09), and thus the effect of this variable may only be modest at best.
Finally, mechanism of injury emerged as a significant predictor of wellness. Individuals who sustained sports or recreational injuries were more likely to be well than those who sustained other types of injuries (mainly falls, motor vehicle collision [MVC], and assault). Seiger and colleagues (Reference Scopaz and Hatzenbuehler2015) similarly found that youth aged 13–21 years who sustained concussion during sports (football and soccer) had shorter recovery periods and better visual memory and motor speed scores on the Immediate Post Concussion Assessment Tool (Lovell et al., Reference Losoi, Silverberg, Waljas, Turunen, Rosti-Otajarvi, Helminen and Iverson2005) than those who sustained concussion due to MVC. They suggest that this effect may be due to increased pressure on athletes to return to play, but highlight that true cognitive differences may also be present and that the unique mechanisms associated with MVC (e.g., higher velocity, different forces) may play a role in the severity of the injury. In an earlier study conducted in adults with mild TBI, Hanlon and colleagues (Reference Hanks, Rapport, Waldron-Perrine and Millis1999) also found that participants with sports-related injuries generally fared better on neuropsychological tests than those who sustained injury through assault, falls, or MVC.
The current findings contribute to a growing body of work that supports the value of examining indicators of positive outcome to better understand TBI. While the concept of wellness lacks a consensual definition, the breadth of the work so far in TBI suggests that positive outcomes can range from specific constructs such as resilience (Losoi et al., Reference Little and Rubin2015; McCauley et al., Reference McCauley, Wilde, Anderson, Bedell, Beers, Campbell and Yeates2013), character traits (Hanks et al., Reference Hanks, Rapport, Waldron-Perrine and Millis2014), and positive psychological growth (Hawley & Joseph, Reference Hawley and Joseph2008), to broader themes such as healthy behaviors (Braden et al., Reference Braden, Cuthbert, Brenner, Hawley, Morey, Newman and Harrison-Felix2012) or quality of life (Di Battista et al., Reference Di Battista, Soo, Catroppa and Anderson2012), and that more work is needed to understand how these factors combine and evolve to influence recovery. The definition of wellness used here was based on a straightforward conceptualization combining the absence of impairment with a single indicator of suitable functioning and was applied only to the outcome of concussion. Future work could broaden this definition to other spheres of functioning (e.g., occupational, physical, social, intellectual, spiritual, emotional) and could contribute to the empirical validation of resiliency models for TBI (see, e.g., Nalder et al., Reference Moran, Taylor, Rusin, Bangert, Dietrich, Nuss and Yeates2018).
Strengths and Limitations
A strength of the study is its longitudinal nature and the analytic approach used, which allowed the investigation of the evolution of wellness across time. Of note, however, only a subset of participants was truly followed over time with complete data at all time points. The statistical model included a range of variables chosen via a rigorous approach. The c-statistic, however, was relatively modest, suggesting that other significant predictors are yet to be identified.
The proposed definition of wellness is useful in that it combines three domains of functioning that are relevant to concussion: symptoms, cognition, and quality of life. However, because these domains inherently rely on different measurement approaches (self-report, parent report, neuropsychological testing), this introduces possible measurement biases that are age-related. For example, the neuropsychological testing may provide a more accurate reflection of a child’s status in the younger age group than the use of self- or parent report of PCS or quality of life at the same age. Related to the issue of measurement bias, evidence suggests that self and parent proxy ratings on questionnaires, such as those used here, show only limited agreement (Balazs et al., Reference Balazs, Miklosi, Toro and Nagy-Varga2016; Sady et al., Reference Russell, Selci, Chu, Fineblit, Ritchie and Ellis2014). The PCSI was completed by different raters in the ED (parent) and at follow-up (participant). Additionally, we did not collect data on the identity of the raters (mothers vs. fathers) in the ED. This procedure may have introduced rater-related biases.
While the sample is one of the largest for which neuropsychological outcomes of concussion have been systematically tested, the sample is characterized by a selection bias, because participants could choose to opt in or out of the neuropsychological substudy. The presence of PPCS in this subgroup was somewhat higher than that in the larger study sample (39% vs. 30–33%), suggesting that the children in the neuropsychology substudy had greater symptom burden and may therefore have been less likely to be classified as well compared to the broader population of children with concussion. Another limitation of the sample is the absence of a control group. It is possible that the demographic predictors of wellness would be the same in an uninjured population of children.
It is possible that a pre-morbid history of cognitive problems and SAC test scores are related. That is, the participants presenting with pre-morbid learning disabilities or ADHD may have performed more poorly on the SAC regardless of their concussion. Children with pre-existing cognitive or psychological difficulties appear to constitute a particular subset of the concussion population that may require specific attention, given the possibility that concussion may compound their difficulties (Beauchamp et al., Reference Beauchamp, Aglipay, Yeates, Desire, Keightley, Anderson and Zemek2018; Iverson et al., Reference Hung, Carroll, Cancelliere, Cote, Rumney, Keightley and Cassidy2017; Plourde et al., Reference Petersen, Scherwath, Fink and Koch2018). Information on pre-morbid cognitive problems was limited in this study to parent report and was not verified quantitatively or through medical reports, which may have introduced inconsistencies in diagnoses and reporting. Related to this, pre-injury functioning was not taken into account for the quality-of-life criterion, which was only based on current ratings relative to normative standards.
CONCLUSIONS
The findings of the study indicate that younger age, absence of pre-morbid cognitive/developmental problems, sports/recreational injuries, and better acute working memory are associated with a greater probability of wellness after pediatric concussion. The advantage of using wellness to characterize recovery after concussion is that the construct takes into account multiple factors. Accordingly, a status of optimal functioning is more difficult to attain using this definition, but may better reflect an individual’s overall perception of recovery in everyday life. The current approach is not meant to minimize the significant and worrisome impact that concussion may have on child development, but rather to emphasize the value of focusing on the large proportion of children who do recover well from their injuries, to inform future research and clinical practice, ultimately leading to better management, treatment, and recovery. Future research should include comparison groups and should further examine the psychological reactions to injury that might influence outcome, as well as document more extensively pre-injury functioning where possible. These additional steps are necessary to pave the way for identifying intervention targets that promote optimal, positive outcomes.
ACKNOWLEDGMENTS
Brian Brooks receives royalties from the sale of the book, Pediatric Forensic Neuropsychology (2012, Oxford University Press), and three pediatric neuropsychological tests [Child and Adolescent Memory Profile (ChAMP; Sherman and Brooks, 2015; PAR Inc.), Memory Validity Profile (MVP; Sherman and Brooks, 2015; PAR Inc.), and Multidimensional Everyday Memory Ratings for Youth (MEMRY; Sherman and Brooks, 2017; PAR Inc.)]. Keith Yeates is supported by the University of Calgary Robert and Irene Ward Chair in Pediatric Brain Injury. He receives royalties for book sales from Guilford Press and Cambridge University Press, and occasionally serves as a paid expert in forensic cases. Miriam Beauchamp receives royalties for book sales from Guilford Press. This study was supported by project funding from the Canadian Institutes of Health Research (R.Z. 293380) and by a Fonds de la Recherche en Santé du Québec salary awards to M.H.B. We would like to acknowledge the input and contributions of the entire 5P Study team, with particular thanks to the coordinators and assistants at the neuropsychology substudy sites and to Mary Aglipay for initial assistance with the statistical analyses.








