



INTRODUCTION
Motivation is a multi-faceted construct that encompasses the cognitions, emotions, and behaviors involved in the activation, execution, and persistence of goal-directed behavior (Kleinginna & Kleinginna, Reference Kleinginna and Kleinginna1981). Reduced motivation is often noted as a consequence of heavy and/or chronic cannabis use (Volkow et al., Reference Volkow, Swanson, Evins, DeLisi, Meier, Gonzalez and Baler2016). This phenomenon is commonly referred to as “amotivational syndrome,” a term that describes the introversion, passivity, and lack of achievement orientation commonly observed among adult cannabis users (McGlothlin & West, Reference McGlothlin and West1968). A recent systematic review of studies examining associations between cannabis use and motivation concluded that evidence from cross-sectional studies was equivocal (Pacheco-Colón, Limia, & Gonzalez, Reference Pacheco-Colón, Limia and Gonzalez2018). Evidence from two longitudinal studies using cross-lagged panel models, on the other hand, lends support to the hypothesis that heavy cannabis use leads to reductions in motivation and/or reward sensitivity among adults (Lac & Luk, Reference Lac and Luk2018; Martz et al., Reference Martz, Trucco, Cope, Hardee, Jester, Zucker and Heitzeg2016).
Several positron emission tomography studies have also examined associations between cannabis use and dopamine, an important neurotransmitter in the context of motivation due to its role in reward-seeking behavior (Berridge, Reference Berridge2007). Results from these studies suggest that adult heavy cannabis users showed reduced dopamine synthesis capacity and reactivity in cortico-striatal areas (Bloomfield, Morgan, Kapur, Curran, & Howes, Reference Bloomfield, Morgan, Kapur, Curran and Howes2014; Volkow et al., Reference Volkow, Wang, Telang, Fowler, Alexoff, Logan and Tomasi2014). These dopaminergic alterations also correlated with lower ratings of motivation on self-report questionnaires (Bloomfield et al., Reference Bloomfield, Morgan, Kapur, Curran and Howes2014; Volkow et al., Reference Volkow, Wang, Telang, Fowler, Alexoff, Logan and Tomasi2014). However, because these studies focused on adults with high levels of cannabis use, it is not yet clear whether these findings generalize to individuals with lower levels of use or who have been using for shorter periods of time.
The effects of cannabis use on motivation are even less clear among adolescents, with the few extant studies yielding mixed results (Jager, Block, Luijten, & Ramsey, Reference Jager, Block, Luijten and Ramsey2013; Lane, Cherek, Pietras, & Steinberg, Reference Lane, Cherek, Pietras and Steinberg2005; Pacheco-Colón et al., Reference Pacheco-Colón, Coxe, Musser, Duperrouzel, Ross and Gonzalez2017). Nonetheless, a large body of work suggests that cannabis use during adolescence leads to poorer educational outcomes, including higher rates of school dropout, lower academic achievement, and lower educational attainment (Fergusson & Boden, Reference Fergusson and Boden2008; Lynskey & Hall, Reference Lynskey and Hall2000; Pacheco-Colón, Ramirez, & Gonzalez, Reference Pacheco-Colón, Ramirez and Gonzalez2019). These findings are presumed to reflect lower academic motivation, although this assertion has rarely been tested empirically. One recent study found that even weekly cannabis use was associated with increased academic aspirations despite worsening academic performance, which suggests that cognitive and behavioral aspects of motivation may be differentially impacted by cannabis use (Patte, Qian, & Leatherdale, Reference Patte, Qian and Leatherdale2017).
In addition, findings from longitudinal studies suggest that adolescent cannabis use may result in increases in depressive psychopathology, including apathy, as well as other related constructs like anhedonia (Pacheco-Colón et al., Reference Pacheco-Colón, Ramirez and Gonzalez2019). However, evidence is mixed, and the temporality of these associations is not yet clear. For instance, using a parallel process model, one study found that significant associations between cannabis use and anhedonia at baseline, as well as between baseline anhedonia and escalation in cannabis use over time (Leventhal et al., Reference Leventhal, Cho, Stone, Barrington-Trimis, Chou, Sussman and Strong2017). This suggests that greater anhedonia may be a risk factor for, rather than a consequence of escalation in cannabis use. On the other hand, another study with similar methodology found that greater adolescent cannabis use at baseline predicted increases in depressive symptoms over time among males, whereas baseline depression failed to predict changes in cannabis use (Assari, Mistry, Caldwell, & Zimmerman, Reference Assari, Mistry, Caldwell and Zimmerman2018). Despite many such findings, the role of depression in the relationship between cannabis use and motivation is still uncertain, as many studies have failed to control for effects of depression.
We previously examined cross-sectional associations between cannabis use and self-reported motivation in a small subset of participants (n = 79), finding null results; however, we were underpowered to detect small effects (Pacheco-Colón et al., Reference Pacheco-Colón, Coxe, Musser, Duperrouzel, Ross and Gonzalez2017). The current study expands on our prior investigation by examining longitudinal associations between cannabis use and various aspects of motivation – namely, apathy, disengagement, persistence, planning, self-efficacy, and valuing school – in a relatively large sample of adolescent cannabis users. Specifically, we use parallel process latent growth curve modeling (LGCM) to examine (1) whether frequency of cannabis use is associated with motivation at baseline, (2) whether baseline frequency of cannabis use predicts changes in motivation over time, (3) whether baseline motivation predicts changes in cannabis use over time, and (4) whether changes in cannabis use predict changes in motivation over time. To the best of our knowledge, this study is the first to apply parallel process analyses to examine longitudinal relationships between cannabis use and self-reported motivation in a sample of adolescents at risk for escalation in cannabis use. A parallel process model allows for the simultaneous estimation of growth in two variables and for the examination of bidirectional influences between these variables. We hypothesize that adolescents with high levels of cannabis use will report lower motivation at baseline, and that increases in cannabis use will predict reductions in motivation. Further, we anticipate that greater cannabis use at baseline will predict declines in motivation over time, whereas the association between baseline motivation and change in cannabis use will be nonsignificant.
MATERIALS AND METHODS
Participants
Participants were 401 adolescents recruited from Miami-Dade County middle and high schools, as well as through flyers posted throughout the community and word-of-mouth referrals. The sample consisted of participants from a study examining longitudinal associations between decision making, episodic memory, and cannabis use trajectories (R01 DA031176, PI: Gonzalez); main outcomes for that study are discussed elsewhere (Duperrouzel et al., Reference Duperrouzel, Hawes, Lopez-Quintero, Pacheco-Colón, Coxe, Hayes and Gonzalez2019). Eligibility for the parent study was ascertained via phone screen. Participants were between the ages of 14–17 at baseline and able to read and write English. In order to recruit a sample at risk for escalation in cannabis use, the sample overrepresented participants with recent use of cannabis. Specifically, use of alcohol, cigarettes, or cannabis – even if minimal – was an inclusion criterion. However, by design, approximately 10% of the sample was allowed to have no history of substance use so that, in addition to having some representation of non-users in the sample (who may still eventually initiate and escalate use during the study), participation in the study did not invariably identify our adolescent participants as substance users. Exclusion criteria included self-reported developmental disorders, birth complications, in utero drug exposure, neurological disorders, history of a traumatic brain injury or loss of consciousness for >10 minutes, a history of formal diagnosis or treatment for a mental health disorder (excluding attention deficit/hyperactivity disorder (ADHD) and conduct disorders given their high comorbidity with adolescent substance use), and use of psychotropic medications with known neurocognitive effects (with the exception of stimulants for ADHD). Although a self-reported formal diagnosis of a mental health disorder (except ADHD) was an exclusionary criterion at the time of screening, participants were not excluded if they later developed a mental health disorder over the course of the study, or if their responses to a structured clinical interview suggested that they met criteria for a disorder during a study assessment.
Participants were also not enrolled in the study if their responses during screening indicated heavy use of alcohol (defined as >13 drinks in a week, or >6–7 drinks in a day, on more than three lifetime occasions) or cannabis (defined as using multiple times per day, every day, for >12 weeks) or an alcohol or cannabis use disorder based on responses to items from the Substance Dependence Severity Scale (Miele et al., Reference Miele, Carpenter, Smith Cockerham, Trautman, Blaine and Hasin2000). Finally, with the exception of alcohol, nicotine, and cannabis, participants who reported prior use of any drug more than 10 times, any use in the 2 weeks prior to screening, or use of any drug to a greater extent than cannabis were excluded from the study.
Importantly, the primary aims of the parent study involved the identification of factors that may influence growth in cannabis use, as well as the development of a cannabis use disorder. Toward this end, we chose to exclude participants with very heavy use of cannabis or a cannabis use disorder in order to minimize the recruitment of individuals who were already at ceiling levels of use. Although participants were excluded during screening if their responses suggested prolonged more than daily use or a cannabis use disorder, we did not exclude participants if they developed a cannabis or other substance use disorder during the study, or if their answers to a structured clinical interview suggested that they met criteria for a substance use disorder during any study assessment, including baseline. Indeed, despite our screening efforts, 22% of our participants met criteria for a lifetime cannabis use disorder at the baseline assessment, and an additional 25% developed a cannabis use disorder over the course of the study. In addition, approximately one quarter of our sample reported daily or near daily use by the final assessment wave. Our sample’s detailed demographic, substance use, and mental health characteristics at each assessment wave are shown in Table 1.
Table 1. Participant demographic, substance use, and mental health characteristics by assessment wave
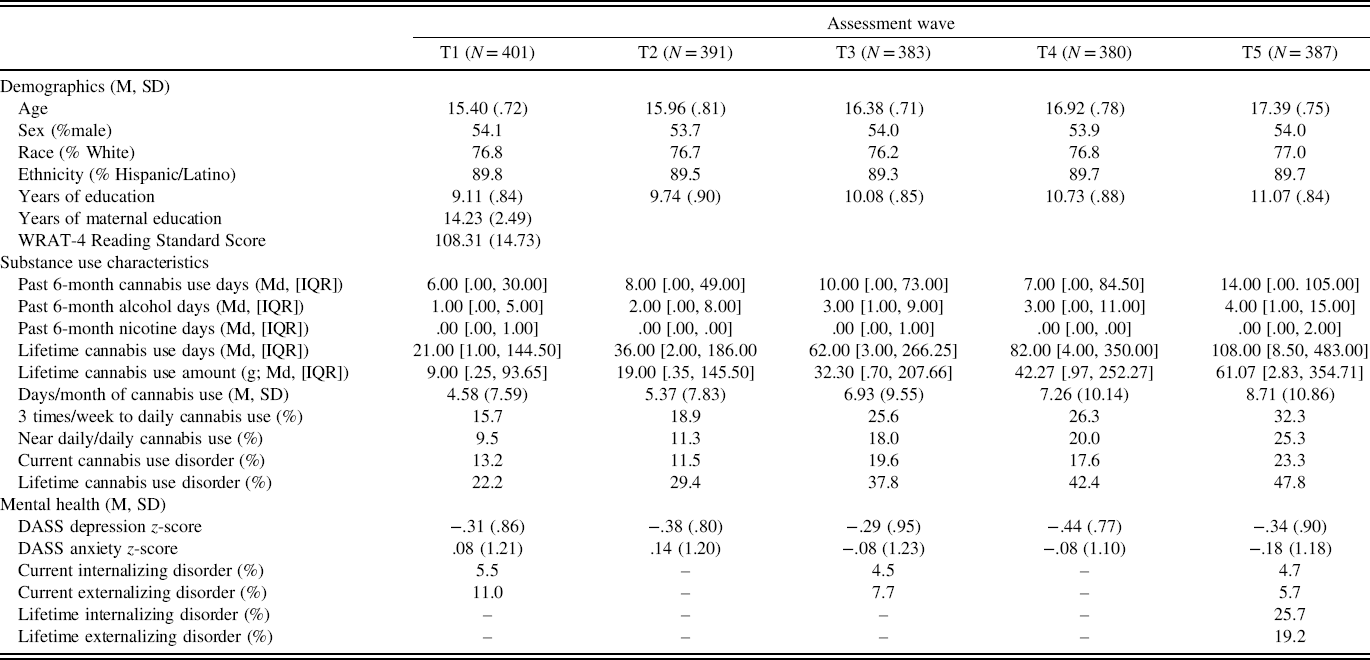
Note: M = Mean; SD = standard deviation; Md = median; IQR = interquartile range; WRAT-4 = Wide Range Achievement Test, 4th Edition; DASS = Depression, Anxiety, and Stress Scale, 21-Item Form. Participants were classified as having an internalizing disorder if they met diagnostic criteria for generalized anxiety disorder, panic disorder, obsessive compulsive disorder, major depression, dysthymia, or mania. Participants were classified as having an externalizing disorder if they met diagnostic criteria for attention deficit/hyperactivity disorder, oppositional defiant disorder, or conduct disorder. “Near daily” was defined as using on most days.
Procedure
We obtained participant assent and parental consent for all participants prior to the baseline assessment. Participant consents were also obtained for those youths who turned 18 years old during the course of the study. Study procedures and protocols were approved by the Institutional Review Board at Florida International University.
The study involved five assessments conducted at 6-month intervals over 2 years. These consisted of in-person assessments conducted at baseline (T1), 1-year follow-up (T3), and 2-year follow-up (T5), as well as telephonic assessments at the 6-month (T2) and 18-month (T4) follow-ups. Substance use and mental health data were collected at each of the five measurement waves (T1–T5), whereas motivation data were collected only during in-person assessments (T1, T3, and T5).
Measures
Substance use
The Drug Use History Questionnaire is a detailed semi-structured interview used to assess frequency and amount of use of 16 different drug classes during a participant’s lifetime, the past 6 months, and the past 30 days (Duperrouzel et al., Reference Duperrouzel, Hawes, Lopez-Quintero, Pacheco-Colón, Coxe, Hayes and Gonzalez2019; Rippeth et al., Reference Rippeth, Heaton, Carey, Marcotte, Moore, Gonzalez and Group2004). Consistent with prior studies from our team (Hawes, Trucco, Duperrouzel, Coxe, & Gonzalez, Reference Hawes, Trucco, Duperrouzel, Coxe and Gonzalez2018), we used past 6-month frequency (in days) of cannabis use at each timepoint as our primary measure of cannabis use. To account for the influence of other substance use on different aspects of motivation, we covaried for past 6-month frequency of alcohol and nicotine use at each timepoint.
Motivation
The Apathy Evaluation Scale (AES) is an 18-item self-report questionnaire that defines apathy as a lack of motivation not attributable to diminished levels of consciousness, cognitive impairment, or emotional distress (Marin, Biedrzycki, & Firinciogullari, Reference Marin, Biedrzycki and Firinciogullari1991). The AES exhibits evidence of strong reliability (Cronbach’s α = .94) and validity (Marin, Firinciogullari, & Biedrzycki, Reference Marin, Firinciogullari and Biedrzycki1993; Marin et al., Reference Marin, Biedrzycki and Firinciogullari1991). AES items are rated on a four-point scale (not at all, slightly, somewhat, and a lot), with higher scores indicative of more apathy (less motivation). We used the summed total AES score as the measure of apathy for our analyses.
The Motivation and Engagement Scale (MES) is a 44-item self-report questionnaire that assesses high school students’ motivation and engagement (Liem & Martin, Reference Liem and Martin2012). The MES has demonstrated evidence of acceptable reliability (Cronbach’s α = .77–.79) and validity, as well as a stable factor structure among high school students (Liem & Martin, Reference Liem and Martin2012). MES items are rated on a seven-point scale (1 = strongly disagree, 7 = strongly agree), with higher scores indicating higher levels of the given construct. The MES assesses motivation through 11 subscales that allow for a more fine-grained analysis of different aspects of motivation and engagement relevant to high school-aged youth. We selected for analyses only those subscales thought to be consistent with our definition of motivation (see Introduction), and/or with definitions used in prior studies examining cannabis use and motivation (Kleinginna & Kleinginna, Reference Kleinginna and Kleinginna1981; Lac & Luk, Reference Lac and Luk2018). Given strong associations between cannabis use and educational outcomes, we also included subscales that assessed school-related motivation and beliefs. Thus, the current study used the following five age-adjusted MES subscale scores: disengagement (i.e., “students’ inclination to give up in their academic work or in achievement setting more generally”), self-efficacy (i.e., “students’ belief and confidence in their ability to do well in their learning”), persistence (i.e., “the extent to which students sustain their engagement”), planning (i.e., “the extent to which students plan their academic work and tasks”), and valuing school (i.e., “students’ belief about the usefulness, importance, and relevance of the academic work they engage in”; Liem and Martin, Reference Liem and Martin2012).
Mental Health
The Depression, Anxiety, and Stress Scale is a 21-item scale used to assess symptoms of depression, anxiety, and stress during the past week (Henry & Crawford, Reference Henry and Crawford2005). Items were rated on a four-point scale, ranging from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). To account for the influence of depression on motivation, we used the seven-item depression subscale as a covariate at each timepoint.
Of note, prior work suggests that ADHD impacts motivation (Volkow et al., Reference Volkow, Wang, Newcorn, Kollins, Wigal, Telang and Swanson2011). However, despite ADHD diagnosis not being exclusionary for our study, only 10 participants met criteria for an ADHD diagnosis at the baseline assessment, which was not sufficient for separate group analyses.
Demographic information
We collected demographic information, including age, sex, race, and ethnicity at the baseline assessment. Due to known sex differences regarding the cognitive effects of cannabis use (Crane, Schuster, Fusar-Poli, & Gonzalez, Reference Crane, Schuster, Fusar-Poli and Gonzalez2013), we included sex as a covariate in our analyses; we also controlled for the effect of participants’ age at the baseline assessment.
Analytic Plan
We used LGCM to characterize developmental patterns of cannabis use and motivation over the 2-year study period. First, we ran separate unconditional linear growth models for cannabis use across all five timepoints, as well as for each measure of motivation over the three available timepoints. Given its count nature and non-normality, the cannabis use variable was modeled both as a continuous variable and with a zero-inflated negative binomial distribution in order to determine the best-fitting model for our data. We then specified a series of six separate multivariate (i.e., parallel process) LGCMs. Each of these parallel process models combined the cannabis use growth curve with one of the motivation growth curves, to be estimated simultaneously.
To address the study hypotheses, the following parameters were specified for each parallel process model: (1) the intercept of the relevant motivation index (i1) was correlated with the cannabis use intercept (i2); (2) the slope of each process was regressed on the intercept of the alternate process (i.e., motivation slope regressed (s1) on cannabis use intercept (i2) and cannabis use slope (s2) regressed on motivation intercept (i1; see Figure 1), and (3) the slope of the motivation index (s1) was regressed on the slope of cannabis use (s2). Finally, all models were tested again and compared after accounting for theoretically relevant confounds (sex, baseline age, depression, alcohol use, and nicotine use).
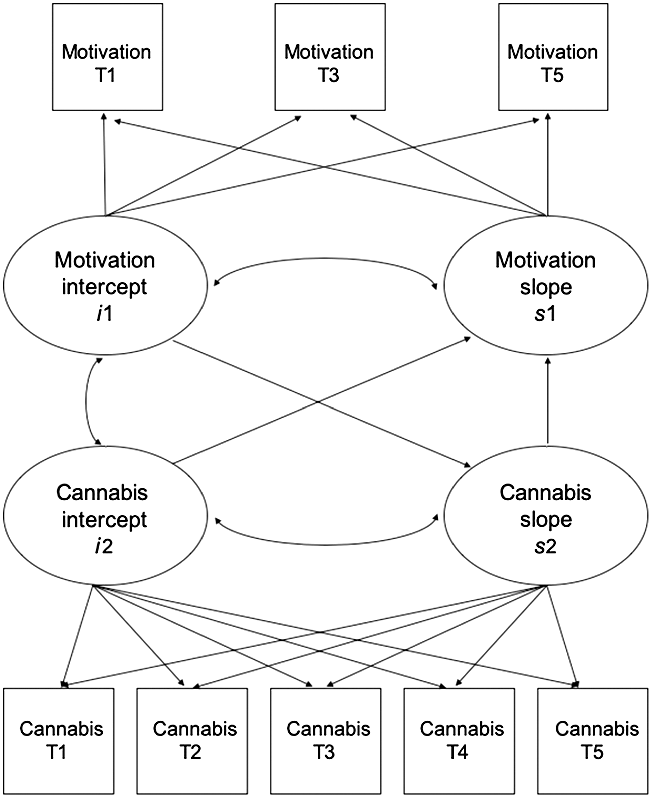
Fig. 1. Parallel process LCGM of cannabis use and motivation, with directional representing directional paths between variables, and curved lines representing covariances modeled.
Analyses were conducted using Mplus 8 (Muthén and Muthén, Reference Muthén and Muthén1998-2017). All models were specified using maximum likelihood estimation with standard errors and a chi-squared statistic that are robust to non-normality (i.e., MLR). Model fit was assessed using absolute fit indices, such as the Comparative Fit Index (CFI) and Root Mean Square Error of Approximation (RMSEA), as well as relative fit indices, such as the sample-size adjusted Bayesian Information Criterion (SABIC) and the Akaike Information Criterion (AIC). CFI values of .95 or greater were used to indicate excellent fit, and values between .90 and .94 were used to indicate acceptable fit (McDonald & Ho, Reference McDonald and Ho2002). RMSEA values less than .05 were used to indicate excellent fit, whereas values between .05 and .10 were used to indicate acceptable fit (McDonald & Ho, Reference McDonald and Ho2002). Due to the count nature of the data, however, absolute fit indices are not provided by Mplus for all analyses involving the cannabis use variable.
Missing data
Of the 401 participants who completed the baseline assessment, 391 completed the 6-month follow-up assessment (98%), 383 completed the 1-year follow-up assessment (96%), 380 completed the 18-month follow-up assessment (95%), and 387 completed the 2-year follow-up assessment (96.5%), indicating low numbers of missed assessments throughout the study. We found no differences on any of the variables used in the current study when comparing participants with complete data and those who missed assessments. All participants provided complete substance use and mental health data at their baseline assessment. However, because collection of motivation data began 22 months after parent study onset, 39 participants did not have motivation data at any timepoint (N = 362 for analyses including only the motivation variables).
To handle missing data, we used full information maximum likelihood (FIML) estimation. FIML can be applied to an incomplete dataset to produce parameter estimates that accurately describe the entire sample. This approach uses information from all available data points to construct parameter estimates under the assumption that the data are missing at random, as is the case in the current study. Even in instances when data are not missing at random, FIML still tends to produce less distorted parameter estimates than other techniques that are traditionally employed to handle missing data, including listwise and pairwise deletion (Collins, Schafer, & Kam, Reference Collins, Schafer and Kam2001; Enders & Bandalos, Reference Enders and Bandalos2001; Wothke, Reference Wothke2000). This is especially true when the proportion of missing data is relatively low (<10%), as in the current investigation (Little, Jorgensen, Lang, & Moore, Reference Little, Jorgensen, Lang and Moore2014). When the current analyses were re-run excluding those participants with no motivation data, the primary results were identical to those using FIML estimates. These analyses are available upon request from the primary author.
RESULTS
Patterns of Cannabis Use and Motivation Over Time
As shown in Table 2, the unconditional LGCM of cannabis use showed better fit when cannabis use was modeled as a count variable using a zero-inflated negative binomial distribution. We therefore used this approach to model cannabis use across all subsequent parallel process models. Overall, there was a significant increase in mean levels of cannabis use over time (p < .001), which represented a moderately sized effect. There was also a significant amount of variability in the slope of cannabis use, suggesting that individual participants varied substantially in their cannabis use trajectories.
Table 2. Fit indices and estimates for unconditional linear growth models of cannabis use and motivation indices

**p < .001, *p <.05. Variance (σ2) estimates are unstandardized. All other estimates are presented in standardized metric.
Note: CU = cannabis use; AES = Apathy Evaluation Scale; MES = Motivation and Engagement Scale; df = degrees of freedom; CFI = Comparative Fit Index; RMSEA = Root Mean Square Error of Approximation; AIC = Akaike Information Criterion; SABIC = Sample-size Adjusted Bayesian Information Criterion; Cov (I/S) = covariance between intercept and slope.
The unconditional growth models of the motivation indices showed excellent to acceptable fit (Table 2). Results were variable for the different motivation indices examined. Specifically, there was a small increase in disengagement (p = .02), with participants showing significant variability in their change in disengagement over time. There was also a moderately sized increase in planning (p = .04) over time. The variability in the planning slope was not significant, which indicates that participants demonstrated similar increases over time. Average rates of change in apathy, persistence, self-efficacy, and valuing school suggested that these aspects of motivation remained stable over time. However, it is important to note that participants varied significantly in their rates of change in apathy and persistence.
Associations Between Cannabis Use and Motivation Over Time
Results from the unadjusted combined models of cannabis use and motivation indicated that the cannabis use intercept was significantly associated with intercepts of the disengagement (p = .001), planning (p = .029), and valuing school (p = .015) subscales (Table 3). The association between the cannabis use and apathy intercepts also trended toward significance (p = .063). These represented modestly sized effects and suggested that adolescents with greater cannabis use at baseline reported higher levels of apathy and disengagement, as well as lower levels of planning and lower perceived value of school at baseline. In addition, the cannabis use intercept significantly predicted the slope of disengagement (p = .032), such that participants with greater cannabis use at baseline showed lesser increases in disengagement over time. Across all models, associations between the intercepts of the motivation subscales and the slope of cannabis use were not significant, indicating that baseline levels of motivation did not predict changes in cannabis use over time (ps = .221–.941). Similarly, associations between the cannabis use slope and the motivation slopes were not significant, suggesting that changes in cannabis use (i.e., slope) did not predict changes in motivation over time (ps = .204–.941).
Table 3. Fit indices and estimates for parallel process models of cannabis use and motivation indices

**p < .001, *p <.05.
Note: CU = cannabis use; df = degrees of freedom; CFI = Comparative Fit Index; RMSEA = Root Mean Square Error of Approximation; AIC = Akaike Information Criterion; SABIC = Sample-size Adjusted Bayesian Information Criterion; Cov (I/S) = covariance between intercept and slope. i1 = motivation index intercept; s1 = motivation index slope; i2 = cannabis use intercept; s2 = cannabis use slope; ←→ = correlation; → = regression path.
As shown in Supplementary Table 1, several covariates demonstrated consistent significant effects across models. For instance, participant age significantly influenced the cannabis use intercept, such that older adolescents reported greater frequency of cannabis use at baseline. Sex significantly impacted the cannabis use intercept and slope, such that males reported greater frequency of cannabis use at baseline, as well as greater increases in cannabis use over time. There was also a significant effect of sex on the intercepts of several motivation indices, suggesting that females reported lower apathy, and greater persistence, planning, and valuing of school than males at baseline. Importantly, depression had a small to moderate effect on several indices of motivation, with greater depression predicting greater apathy and disengagement, as well as lower persistence, planning, and valuing of school. Effects of alcohol and nicotine use on motivation were largely nonsignificant.
After controlling for sex, baseline age, depression, and use of alcohol and nicotine, most associations between cannabis use and motivation attenuated to nonsignificance (Table 4). However, the association between the intercepts of cannabis use and the valuing school subscale remained significant (p = .024). Thus, after controlling for potential confounds, greater cannabis use was cross-sectionally associated with lower valuing of school. There was also a trend toward significance in the association between the cannabis use and disengagement intercepts (p = .073), which suggested that participants with higher levels of cannabis use also reported greater disengagement.
Table 4. Fit indices and estimates for covariate-adjusted parallel process models of cannabis use and motivation indices

**p < .001, *p <.05. All estimates are presented in standardized metric.
Note: CU = cannabis use; df = degrees of freedom; CFI = Comparative Fit Index; RMSEA = Root Mean Square Error of Approximation; AIC = Akaike Information Criterion; SABIC = Sample-size Adjusted Bayesian Information Criterion; i1 = motivation index intercept; s1 = motivation index slope; i2 = cannabis use intercept; s2 = cannabis use slope.
Post-Hoc Exploratory Analyses of Sex Differences
Because sex had a significant effect on both cannabis use and several of the motivation indices in adjusted models, we ran a series of multiple group models to explore whether model parameters differed significantly between males and females. Specifically, we ran the final covariate-adjusted models using sex as a grouping variable, and constraining the associations between cannabis use and motivation to be equal across groups. Using the Wald test of parameter constraints, we found no significant sex differences in the associations between cannabis use and apathy, disengagement, persistence, planning, and valuing school. However, there was a significant sex difference in the association between cannabis use and self-efficacy, particularly between the self-efficacy intercept and the cannabis use slope (Wald = 4.37, p = .037). For females, greater self-efficacy at baseline was associated with greater escalation in cannabis use over time (β = .77, p < .001), whereas this relationship was not significant for males (ß = −.10, p = .709).
DISCUSSION
The current study examined longitudinal associations between adolescent cannabis use and different aspects of self-reported motivation to test the hypothesis that higher levels of cannabis use are associated with lower levels of or reductions in motivation over time. The number of days that participants reported using cannabis during the 6 months prior to study visits increased significantly across the five measurement waves, which occurred every 6 months over 2 years. Our results showed different patterns of change across measures of motivation. Specifically, participants’ disengagement and planning evidenced significant increases over time, whereas apathy, persistence, self-efficacy, and valuing school remained stable. Findings from parallel process models suggest that, at baseline, greater cannabis use frequency was significantly associated with greater disengagement, as well as lower planning and valuing of school. Greater baseline cannabis use also predicted lesser increases in disengagement over time but failed to predict changes in all other motivation indices. However, after controlling for covariates, only the association between cannabis use and valuing school remained significant. Across all models, baseline levels of motivation did not predict change in cannabis use, and change in cannabis use across assessment waves failed to predict changes in motivation over time.
Together, our findings suggest that cannabis users may display lower levels of certain aspects of motivation. However, most of these associations can be explained by other factors, particularly participant demographics, such as age and sex, and depression. Further, despite significant increases in levels of cannabis use in our sample, change in cannabis use did not predict changes in motivation, which suggests that cannabis use may not lead to reductions in motivation over time. Nonetheless, we found that greater cannabis use was associated with lower perceived value of school at baseline, even after controlling for covariates. This is in line with prior work suggesting that adolescent cannabis users tend to adopt alternative, anti-conventional lifestyles which may ultimately contribute to the poorer educational outcomes observed among cannabis users (Fergusson & Boden, Reference Fergusson and Boden2008; Lynskey & Hall, Reference Lynskey and Hall2000).
In addition, results from exploratory analyses suggest that sex may moderate the associations between cannabis use and some aspects of motivation. Surprisingly, females who reported higher levels of self-efficacy at baseline also reported greater escalation in cannabis use over time; this association was not significant for males. These findings are not consistent with those of prior studies that have examined associations between cannabis use and self-efficacy (Lac & Luk, Reference Lac and Luk2018) and do not support an “amotivational syndrome” in cannabis-using females. Rather, although speculative, they suggest that greater confidence in their academic skills may lead adolescent females, but not males, to escalate in their cannabis use without worrying about related academic consequences. More work is needed to determine whether this finding can be replicated in other samples.
We recently reviewed the literature examining effects of cannabis use on motivation and reward sensitivity, concluding that although cross-sectional evidence is mixed, results from two longitudinal studies lend partial support to “amotivational syndrome” (Pacheco-Colón et al., Reference Pacheco-Colón, Limia and Gonzalez2018). Findings from the current study, however, are not consistent with those of previous longitudinal studies. There are several possible explanations for these inconsistencies. First, our study focused on adolescents, while the previous longitudinal studies utilized adult samples (Lac & Luk, Reference Lac and Luk2018; Martz et al., Reference Martz, Trucco, Cope, Hardee, Jester, Zucker and Heitzeg2016). It is possible that negative effects of cannabis use on motivation may only become apparent at the highest levels of use (i.e., chronic daily use) or with greater cumulative use than that observed in the adolescents in our sample. Adolescents in our sample were 14–17 years old at baseline, making this one of the youngest samples studied concerning cannabis use and motivation. Although, by design, the majority of participants reported some cannabis use at study onset, only 15% reported heavy (3 times/week to daily) use at baseline, with approximately one quarter of the sample reaching near daily use by the final assessment (Hawes et al., Reference Hawes, Trucco, Duperrouzel, Coxe and Gonzalez2018). We also excluded participants who, at the time of screening, reported very heavy cannabis use or whose answers suggested the presence of a cannabis use disorder. Thus, it is possible that adolescents in our sample may not have engaged in heavy cannabis use for sufficiently long duration for reductions in motivation to manifest. Future studies should continue to examine consequences of cannabis use during adolescence to examine possible dose–response relationships between cannabis use and motivation.
Additionally, there is significant cross-study variability in the tools used to assess motivation, which include neuroimaging measures, performance-based tasks, and self-report questionnaires. Our study assessed multiple aspects of self-reported motivation and found mixed results, suggesting that cannabis use may be more strongly associated with some aspects of motivation (e.g., school-related motivation) than others (e.g., persistence). However, self-report measures may not be optimal to assess cannabis-related reductions in motivation, as they tend to assess cognitive components of motivation, such as an individual’s perceived persistence. Rather, cannabis use may have a stronger effect on behavioral components of motivation, as captured by performance-based measures, such as effort and willingness to work for a reward (Hirst, Young, Sodos, Wickham, & Earleywine, Reference Hirst, Young, Sodos, Wickham and Earleywine2016; Lane et al., Reference Lane, Cherek, Pietras and Steinberg2005). Interestingly, a recent study found support for amotivational syndrome based on informant-report questionnaires, suggesting that questionnaires may be more sensitive to changes in motivation when ratings are based on behavioral observation rather than introspection (Meier & White, Reference Meier and White2018). It is therefore possible that cannabis use may impact behavior outside of conscious awareness, which could also explain prior findings that cannabis use is associated with higher academic aspirations despite worsening academic performance (Patte et al., Reference Patte, Qian and Leatherdale2017).
Although the current study did not find support for a longitudinal link between escalation in cannabis use and reductions in motivation, there is sufficient knowledge about potential underlying neurobiological mechanisms to warrant concern. As previously mentioned, recent work has found that cannabis users show decreased dopamine synthesis capacity and reactivity in striatal regions (Bloomfield et al., Reference Bloomfield, Morgan, Kapur, Curran and Howes2014; Volkow et al., Reference Volkow, Wang, Telang, Fowler, Alexoff, Logan and Tomasi2014), which may be related to findings of blunted activation in anticipation of non-drug rewards (Martz et al., Reference Martz, Trucco, Cope, Hardee, Jester, Zucker and Heitzeg2016; van Hell et al., Reference van Hell, Vink, Ossewaarde, Jager, Kahn and Ramsey2010). Further, the functioning of the cortico-limbic reward system is modulated by the endocannabinoid system, which is also impacted by cannabis use (Melis, Muntoni, & Pistis, Reference Melis, Muntoni and Pistis2012). More specifically, -9-tetrahydrocannabinol – the primary psychoactive ingredient in cannabis – binds primarily at cannabinoid receptors type 1 (CB1; Pertwee, Reference Pertwee2006), which are densely concentrated in cortico-limbic regions (Glass, Faull, & Dragunow, Reference Glass, Faull and Dragunow1997). Chronic use of cannabis leads to a downregulation of CB1 receptors throughout the brain, which may indirectly impact the cortico-limbic reward system (Hirvonen et al., Reference Hirvonen, Goodwin, Li, Terry, Zoghbi, Morse and Innis2012). Together, these findings suggest that cannabis use may have a significant neurobiological impact on the brain’s reward system and, consequently on motivated behaviors, through its effects on the dopaminergic and endocannabinoid systems. In addition, a substantial body of work suggests that cannabis use may lead to increased depressive symptomology over time (Lev-Ran et al., Reference Lev-Ran, Roerecke, Le Foll, George, McKenzie and Rehm2014). Because reduced motivation is a symptom of depression, it is not clear whether cannabis use may selectively impair motivation or broadly increase depressive symptoms. More work is thus needed to determine which aspects of motivation are most affected by cannabis use and to disentangle associations between cannabis use, motivation, and depression.
The current study has several notable strengths, including the large unique sample of adolescents who were primarily cannabis users, the examination of several different facets of motivation, the inclusion and control of important confounding variables, and the use of longitudinal LGCM techniques that are better able to address questions of temporality. Nonetheless, these findings should be interpreted in light of several limitations. First, our results certainly do not generalize to all adolescents. The parent study inclusion/exclusion criteria were designed to recruit a sample of participants at risk for escalation in cannabis use. It is thus possible that our findings may not apply to adolescents who are not considered “at risk” for escalation in their use. Toward this end, our study also excluded adolescents reporting a cannabis use disorder or prolonged more than daily cannabis use at the time of screening. Although cannabis use increased significantly over the course of the study, the majority of participants did not report heavy, daily cannabis use. Our results may thus not generalize to cannabis users with heavier or more chronic use trajectories. Nonetheless, the relatively lower levels of use reported by our participants are more common than near daily use among adolescents in the general population (Substance Abuse and Mental Health Services Administration, 2019). Thus, we believe that our findings may generalize to a larger proportion of adolescent cannabis users than results from a study that focuses only on daily users or on those with a cannabis use disorder. In addition, our sample was predominantly Hispanic/Latino (89.8%) and White (76.8%), which may limit generalizability to more diverse samples, although no evidence currently suggests that the associations between cannabis use and motivation may vary by race or ethnicity. Second, the measures of motivation employed in this study were based on participant self-report, which may be influenced by social desirability and/or poor insight. Future studies should include both self and informant reports, as it would be informative to determine whether cannabis users exhibit behavior consistent with reduced motivation, which they may not be aware of. In a similar vein, the current study did not employ performance-based measures of motivation or academic achievement. Given the breadth of this construct, a multi-modal approach would be most appropriate when assessing motivation. Cannabis use is also increasingly varied and complex. The current study only employed one index of cannabis use frequency (i.e., days of use) and was thus not able to examine potential effects of method or amount of cannabis use. Nonetheless, frequency indices are slightly more reliable than amount indices in timeline follow-back interviews among adolescents (Levy et al., Reference Levy, Sherritt, Harris, Gates, Holder, Kulig and Knight2004) and are often used to quantify cannabis use in the extant literature.
CONCLUSIONS
Our findings do not support a relationship between cannabis use and reductions in motivation over time in a sample of adolescents at risk for escalation in cannabis use. Although unadjusted models revealed several significant cross-sectional and longitudinal associations between cannabis use and motivation, most attenuated to nonsignificance after controlling for covariates. Nonetheless, even in adjusted models, we found a significant cross-sectional link between cannabis use and lower perceived value of school at baseline. Our findings also indicated that females, but not males, who reported higher self-efficacy at baseline showed greater escalation in cannabis use over time. The current study contributes to the extant literature by examining these associations longitudinally in a large sample of adolescent cannabis users while controlling for important and often overlooked confounds, including sex and depression. Future studies should continue to examine these associations longitudinally to determine whether heavier levels of cannabis use lead to reductions in motivation, and whether these reductions may be responsible for poorer educational and later life outcomes.
Acknowledgments
This work was supported by R01 DA031176 and U01 DA041156 (PI: Gonzalez), and F31 DA047750-01A1 (PI: Pacheco-Colón) from the National Institute on Drug Abuse, as well as NSF CNS-1532061.
Conflicts of interest
The authors declare no conflicts of interest.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S135561772000096X







