


INTRODUCTION
Visual mental imagery occurs when perceptual information is accessed from memory, giving rise to the experience of “seeing with the mind’s eye.” This is not an undifferentiated cognitive process but a collection of abilities that rely on different cerebral structures (Kosslyn, Ganis, & Thompson, Reference Kosslyn, Ganis and Thompson2001). Kosslyn’s model (1980) points out that there are three different imagery processes: generation, which creates the image in the visual buffer (that is a mental screen on which subject visualizes the image); inspection, which allows identifying parts and relations within the image; and transformation, which allows manipulating the image, for example, by rotating or translating it. Evidence from single cases suggests that these processes can be affected in different ways by brain damage. For instance, some patients are impaired on tasks involving the visual generation of mental images but not on transformation tasks, such as a mental rotation test (Farah, Hammond, Levine, & Calvanio, Reference Farah, Hammond, Levine and Calvanio1988), while other patients show the reverse pattern of dissociation (Luzzatti, Vecchi, Agazzi, Cesa-Bianchi, & Vergani, Reference Luzzatti, Vecchi, Agazzi, Cesa-Bianchi and Vergani1998). Moreover, dissociation among different types of transformation processes has been reported. For example, the patient described by Riddoch (Reference Riddoch1990) showed a deficit in both generating and transforming visual mental images, characterized by spared assembly of mental image processes and defective mental rotation processes.
However, it seems that processes which involve generation, inspection and transformation are affected by the stimulus category. Indeed, several studies have suggested that the pattern of brain structures activated during mental imagery depends on the content of the visual image. O’Craven and Kanwisher (Reference O’Craven and Kanwisher2000) showed that a portion of the fusiform face area is more active during the mental imagery of faces than during the mental imagery of scenes, while a portion of the parahippocampal place area is more active during the mental imagery of scenes than during the mental imagery of faces. Ishai, Ungerleider, and Haxby (Reference Ishai, Ungerleider and Haxby2000) reported different activations in temporal and occipital regions depending on the content of mental images (houses, chairs, and faces). Similarly, Kreiman, Koch, and Fried (Reference Kreiman, Koch and Fried2000) recorded single neurons in the human temporal lobe and found that some neurons increased their firing rate only when the subject imagined particular kinds of stimuli. For example, single neurons in the entorhinal cortex fired selectively for objects, but not for faces, cars, animals, food or complex patterns.
In a previous study, we reported the results of a battery of tests assessing different mental imagery abilities in a sample of left and right brain-damaged patients. We found that only right brain-damaged patients affected by hemineglect failed on most of the battery tests, demonstrating that the right hemisphere plays a crucial role in visual mental imagery. We also observed a specific relationship between the hemi-spatial neglect syndrome and deficits in visual mental imagery. In particular, representational neglect patients seemed to be specifically compromised in generating and manipulating topographical mental images (Palermo, Piccardi, Nori, Giusberti, & Guariglia, submitted). Representational neglect is a well-known imagery disorder, but its nature is still unclear and it has been interpreted in different ways. It has been considered the consequence of damage to the cognitive system involved in coding and storing environmental information used for navigation (Guariglia, Padovani, Pantano, & Pizzamiglio, Reference Guariglia, Padovani, Pantano and Pizzamiglio1993; Guariglia, Piccardi, Iaria, Nico, & Pizzamiglio Reference Guariglia, Piccardi, Iaria, Nico and Pizzamiglio2005; Nico, Piccardi, Iaria, Bianchini, Zompanti, & Guariglia, Reference Nico, Piccardi, Iaria, Bianchini, Zompanti and Guariglia2008; Piccardi, Bianchini, Zompanti, & Guariglia, Reference Piccardi, Bianchini, Zompanti and Guariglia2008) or of a deficit in the working memory system (Beschin, Cocchini, Della Sala, & Logie, Reference Beschin, Cocchini, Della Sala and Logie1997; Della Sala, Logie, Beschin, & Denis, Reference Della Sala, Logie, Beschin and Denis2004; Logie, Della Sala, Beschin, & Denis, Reference Logie, Della Sala, Beschin and Denis2005).
However, none of these explanations completely accounts for the results reported in the literature. For instance, reviewing the representational neglect literature, it appears that some patients performed asymmetrically when describing familiar environments but showed no asymmetry on tasks involving objects (i.e., O’Clock test) or arrays of objects (i.e., the inside of a car) (Guariglia et al., Reference Guariglia, Padovani, Pantano and Pizzamiglio1993; Guariglia & Pizzamiglio, Reference Guariglia, Pizzamiglio, Vecchi and Bottini2006; Ortigue et al., Reference Ortigue, Viaud-Delmon, Michel, Blanke, Annoni and Pegna2003; Piccardi et al., Reference Piccardi, Bianchini, Zompanti and Guariglia2008); other patients showed the reverse pattern of dissociation (Grossi, Modaferri, Pelosi, & Trojano, Reference Grossi, Modaferri, Pelosi and Trojano1989). Therefore, these data seem to be better explained by the hypothesis that the different pattern of brain structures activated according to the content of mental images can be differently disrupted. In fact, Guariglia and Pizzamiglio (Reference Guariglia, Pizzamiglio, Vecchi and Bottini2006, Reference Guariglia, Pizzamiglio, Mast and Jäncke2007) hypothesized that two different types of mental representation exist, that is, “topological images” and “nontopological images”, and that they could be selectively damaged in neglect. Topological images are described as mental representations of stimuli in which it is possible to navigate (i.e., familiar city squares), while nontopological ones are representations of objects or visuo-spatial displays (i.e., a clock dial). However, up until now no studies have tried to verify this dissociation.
Specifically, the aim of this work was to determine whether representational neglect can be explained by a deficit in generating, inspecting and transforming images in relation to the content of the images.
For this reason, we analyzed the mental imagery abilities of two patients with different kinds of representational neglect involving, in one case, the representation of objects and, in the other, the representation of environments, to investigate the differences between images of objects and environments. The current study adds to the representational neglect literature an extensive evaluation of each process (generation, inspection, and transformation) involved in the mental imagery in two patients with two type of representational neglect by using the same test battery. For the first time it was demonstrated that each imagery process is damaged and selectively compromised according to the type of image. In fact, Patient 1 that showed a deficit in O’Clock test failed in all imagery processes of object mental representation, while Patient 2 that showed a deficit in Familiar Square Description Test failed in all imagery processes involved in environment mental representation. Using the same battery allowed a real comparison between the two cases.
METHOD
Case Reports
Patient 1 is a 49-year-old, right-handed male hairdresser with 13 years of education. Two months before our examination, he suffered from a vascular accident (stroke) that induced left hemiplegia. A T1 weighted magnetic resonance imaging (MRI) revealed a lesion involving the right frontal, parietal, and temporal regions (Brodmann’s areas, 6, 21, 22, 40; Figure 1).

Fig. 1. Patient 1’s T1-weighted magnetic resonance imaging scan; left and right refer to the side of brain.
The patient was submitted to an extensive neuropsychological evaluation (Table 1). His speech was fluent and informative; his naming and comprehension abilities were intact. The patient had no difficulty on either short- or long-term verbal and spatial memory tests. He also had no deficit in abstract reasoning (Verbal Judgments, Spinnler and Tognoni, Reference Spinnler and Tognoni1987) or in visual integration ability (Street’s Completion Test, Street, Reference Street1931; Spinnler & Tognoni, Reference Spinnler and Tognoni1987). However, a deficient performance was recorded in neglect assessment. The patient showed signs of perceptual neglect on the Standardized battery for the evaluation of visuo-spatial neglect (Pizzamiglio, Judica, Razzano, & Zoccolotti, Reference Pizzamiglio, Judica, Razzano and Zoccolotti1989) and imagery neglect. In particular, the patient performed asymmetrically when he had to imagine two different times on two analog clocks and to decide on which one the clock hands formed the widest angle (a modified version of the O’Clock Test; Grossi et al., Reference Grossi, Modaferri, Pelosi and Trojano1989). In this test, which was composed of 32 items, the clock hands were in the right hemiface in 16 items (e.g., 14:00; 17:00) and in the left hemiface in 16 items (e.g., 8:00; 11:00). The patient correctly solved the right-sided items (score 16/16) but not all of the left-sided items (score 11/16). The correct answers in the left and in the right clock hemiface were transformed into a laterality quotient (LQ = (left elements − right elements)/(left elements + right elements) × 100; Bartolomeo, D’Erme, & Gainotti, Reference Bartolomeo, D’Erme and Gainotti1994). The patient’s LQ was –18.5, which corresponded to a defective performance (cutoff = −16; Piccardi et al., Reference Piccardi, Bianchini, Zompanti and Guariglia2008).
Table 1. Individual patients’ results on the neuropsychological assessment

* Deficit performance; L = left side; R = right side; QL = laterality quotient.
** It is a test of perceptual closure in which the patient is asked to recognize 14 degraded pictures of objects or animals.
*** In this test, each stimulus comprises two black fans, identical in area but different in shape, whereby one appears longer than the other, even though they are equal in length. In the version by Massironi et al. (Reference Massironi, Antonucci, Pizzamiglio, Vitale and Zoccolotti1988), the illusory effect is produced either by the left or by the right extremities of the fans. Patients with neglect make errors (that is, they fail to show the normal illusory effect) when the illusion arises in the left halves of the fans, while their performance is normal (that is, they show the illusory effect) when the illusion is produced by the right halves of the fans.
**** In this test, a sentence (article-noun-verb-adjective/adverb-noun) printed horizontally in the middle of an A4 sheet is centrally presented to the subject. Subject is asked to read aloud six different sentences; number of correctly read sentences is reported (hits). One error (or more), specifically omissions, in the left side or in the left of each word is considered as indicative of a pathological performance (Pizzamiglio et al., Reference Pizzamiglio, Judica, Razzano and Zoccolotti1989).
***** This test requires to judge differences and analogies, to interpret proverbs and to find logical errors in short novels.
On the other hand, the patient described two familiar city squares from two opposite points of view in similar fashion (Familiar Squares Description Test; Bisiach & Luzzatti, Reference Bisiach and Luzzatti1978). When the patient was required to describe two squares in Rome (Piazza del Popolo and Piazza Venezia), he reported overall 16 elements on the right side and 17 elements on the left side. The elements reported on the left and right sides of the squares were transformed into a laterality quotient. The patient’s LQ was 3, which was within the norm (cutoff = −16; Piccardi et al., Reference Piccardi, Bianchini, Zompanti and Guariglia2008).
Patient 2 is a 40-year-old, right-handed man with 13 years of education. He underwent surgical treatment for angioma. MRI revealed brain damage corresponding with frontal areas (Figure 2).

Fig. 2. Patient 2’s magnetic resonance imaging scan; left and right refer to the side of brain.
He came under our observation 11 years after the surgery (see Table 1 for neuropsychological assessment). His naming and comprehension abilities were good. The patient had no difficulty on verbal and visuo-spatial memory tests. He had no deficit in abstract reasoning or in visual integration ability. However, some difficulties were detected in divided attention (TEA, Test per l’Esame dell’Attenzione; Zimmerman & Fimm, Reference Zimmermann and Fimm1992: patients have to respond to acoustic signals or/and visual square configurations appearing at random intervals), and he spontaneously reported a severe deficit in orienting himself in the environment. For instance, he reported some difficulties in finding the exit in a shopping center. On the Standardized battery for the evaluation of visuo-spatial neglect (Pizzamiglio et al., Reference Pizzamiglio, Judica, Razzano and Zoccolotti1989), the patient showed no disorders. On the other hand, the patient reported a deficient performance in the assessment of imagery neglect. In particular, his performance was asymmetric when he had to describe two familiar city squares from two opposite vantage points (Familiar Squares Description Test; Bisiach & Luzzatti, Reference Bisiach and Luzzatti1978). The patient was required to describe two squares in Rome (Piazza del Popolo and Piazza Venezia) and overall reported 11 elements on the right and 2 elements on the left of both squares. The elements described on the left and on the right sides of the squares were transformed into a LQ (Bartolomeo et al., Reference Bartolomeo, D’Erme and Gainotti1994). The patient’s LQ was −69.23, which corresponded to a defective performance (cutoff = −16; Piccardi et al., Reference Piccardi, Bianchini, Zompanti and Guariglia2008). On the other hand, the patient did not perform asymmetrically when he had to imagine two different times on two analog clocks and to decide on which one the clock hands formed the widest angle (a modified version of the O’Clock Test; Grossi et al., Reference Grossi, Modaferri, Pelosi and Trojano1989). The patient correctly solved 15/16 right-items and 15/16 left-items. The correct answers on the left and on the right clock hemiface were transformed into a LQ (Bartolomeo et al., Reference Bartolomeo, D’Erme and Gainotti1994). The patient’s LQ was 0, which corresponded to a normal performance (cutoff = −16; Piccardi et al., Reference Piccardi, Bianchini, Zompanti and Guariglia2008).
Both patients were submitted to a complex visuo-spatial imagery battery (Palermo, Piccardi, Nori, Giusberti, & Guariglia, submitted), which included tasks requiring the generation, inspection and manipulation of objects (including common objects, architectonic objects, and abstract figures) and tasks involving the generation, inspection and manipulation of real environments.
The study was approved by the local Ethics Committee. All participants gave written informed consent.
Before performing the battery, both patients were submitted to a Vividness Task (Vincenzi, Reference Vincenzi2000) to see whether they would spontaneously report a total lack of image generation. In particular, we asked the patients to imagine a common object (e.g., a bottle) and then to choose among five pictures (a perfect 3-D object figure, a black and white figure, a 2-D figure, a blurred figure, and no figure; Figure 3) the one that was most similar to their mental image. The task included 20 trials. Similarly to the controls, neither patient ever chose the “no figure cards” or the blurred ones nor reported a mental imagery deficit spontaneously.

Fig. 3. Example of Vividness task items. Subjects had to select, from among five pictures (A: a perfect 3-D object figure; B: a blurred figure; C: a black and white figure; D: a 2-D figure, and E: no figure). Four points were assigned to A, 3 points to D, 2 points to C, 1 point to B, and 0 points to E.
Object Image Tasks
Generation task
Building task (a modified version of the “Photo task,” Nori & Giusberti, Reference Nori and Giusberti2006). This task involves the ability to generate a mental image of an architectonic object (i.e., a building) from short-term memory and to hold it in the visual buffer. The patients were required to look at a photograph of a building for 10 s and then to recognize it among three distracters. Distracters were obtained by manipulating the target item using Adobe Photoshop. Manipulations consisted of alterations of basic visual characteristics (i.e., color) or of addition or subtraction of specific elements (Figure 4). The task included 20 trials (maximum score 20).

Fig. 4. Example of Building Task items. Subjects had to recognize the photo target (top) seen a few seconds before among distracters depicted on a sheet of paper [i.e., one target (C), three distracters]. Distracters consisted of similar buildings distinguished by some basic visual characteristics (D) or presence/absence of elements (B) and a mirror image of the target (A).
Inspection task
Overlapping task (Sassi, Reference Sassi1986). In this task, the patients were asked to imagine that some figures were dropped on a sheet of paper and to number them starting from the first one dropped (Figure 5). The task included four trials (maximum score: 28).

Fig. 5. Example of Overlapping Task item.
Transformation tasks
In accordance with Kosslyn’s model, we used several tasks to analyze different transformation processes such as mental assembly, reconstruction, folding and rotation.Footnote 1
Mental assembly task. In this task, the patients were asked to mentally assemble three segments of an object (i.e., a streetlamp) and then to judge whether a successively presented whole figure corresponded to the assembly created. Stimuli were presented sequentially (on a vertical or horizontal axis, Figure 6a) on a computer screen with SuperLab (Cedrus, Wheaton, MD; Haxby, Parasuraman, Lalonde, & Abboud, Reference Haxby, Parasuraman, Lalonde and Abboud1993). Each segment of the object was presented for 2500 ms (ISI 500 ms); then the whole picture was presented until the subject pressed one of two response keys (“yes” or “no”). The task included 60 trials (maximum score: 60).

Fig. 6. a: Example (left) of the procedure followed in the Mental Assembly Task and examples (right) of vertical axis stimuli with two different types of response (“yes” or “no”). b: Example of Sequence Task item. Subjects had to observe the picture of a landscape in frontal view (left); 20 s later, they had to mentally arrange panels (right). c: Example of Mental Folding Task item. d: Example of Mental Rotation Task item.
Sequence task (Nori & Giusberti, Reference Nori and Giusberti2006). Patients observed the picture of a landscape they had never seen before in frontal view (Figure 6b). Twenty seconds later the same picture was shown divided into three, four or five panels. The participant’s task was to mentally reconstruct the original picture, indicating by pointing in which order the pieces should be arranged to correctly reconstruct the scene. The patients performed 20 trials (maximum score: 20).
Mental folding task (based on French, Ekstrom, & Price, Reference French, Ekstrom and Price1963). The patients had to mentally fold an unfolded cube and to indicate whether the arrows marked on the two sides of the cube would touch each other (Figure 6c). The patients performed 20 trials (maximum score: 20).
Mental rotation task (based on Thurstone, Reference Thurstone1937). In this task, we asked the patients to choose among five figures those that would correspond to the target when mentally rotated (Figure 6d.). The task included 21 trials (maximum score: 21).
Environment Image Tasks
This task involved the processing of images acquired moving through a real environment. The two patients had to learn a pathway in an area of the hospital they had never explored before. There were 13 landmarks and five turning points (three on the right and two on the left) along the route (Figure 7a). In the learning phase, the experimenter went with the patients to the starting point of the pathway and said: “This is the starting point. We will follow the same path three times. Along the way I will point out some landmarks that you should look at carefully. Then I will ask you some questions about those landmarks and some details about the pathway”.

Fig. 7. a: Pathway (red line) in the hospital with landmarks and turning points never explored before by the participants. b: Example of Landmark Recognition Task item. Target (left) seen on the pathway and its distractor (right).
At the end of the learning phase, the patients had to perform six different tasks.
Generation task
Landmark Task. This task involved the ability to generate a mental image of the previously seen landmarks from long-term memory (Figure 7b). Pictures of the 13 landmarks interspersed with 13 pictures of distracters (an object similar to one of the landmarks for function and size) were presented one by one. The patients’ task was to recognize the landmarks they encountered on the path (maximum score: 26).
Inspection tasks
Egocentric navigational questions. This task included 15 questions. The patients had to imagine themselves with respect to one of the previously seen landmarks and to inspect it to answer questions such as: “Imagine being in front of the snack-machine: is it taller or shorter than you?”(maximum score: 15).
Allocentric navigational questions-inspection. This task was composed of six questions. The patients had to generate the image of two landmarks and inspect them to answer questions such as: “Is the lamppost higher or lower than the electric box?”(maximum score: 6).
Route-direct pathway direction questions. This task was composed of seven questions that investigated the ability to imagine the pathway in the same learning perspective and to inspect it. For example: “Imagine being at the poster and looking at the emergency exit: do you turn right or left to reach the doctor’s office?”(maximum score: 7).
Transformation tasks
Route-inverse pathway direction questions. This task was composed of eight questions in which patients had to imagine the pathway in a different perspective (rotated by 180°) from the learned one. For example: “Imagine turning your back to the electric box. To go toward the plant, do you turn right or left?”(maximum score: 8).
Allocentric navigational questions-transformation. This task was composed of six questions. The patients had to generate the image of two landmarks and manipulate them to answer questions such as: “If the coffee-machine fell toward the snack-machine, would the door between them be blocked?”(maximum score: 6).
RESULTS
We analyzed the patients’ performances on the imagery tasks with respect to the performances of a group of control subjects who had no signs of neurological or psychiatric impairment (C: several subjects that varied from 17 to 20; mean age = 61.7 years; SD = 12.4; mean education = 10.16, SD = 5.11), by means of Crawford’s analysis (Crawford & Howell, Reference Crawford and Howell1998; Crawford & Garthwaite, Reference Crawford and Garthwaite2002), using the computer program SINGLIMS.EXE (see Table 2). This method allows estimating the abnormality of the individual scores and testing whether it is significantly lower than the scores of the control sample. It is the more suitable analysis when the normative sample is small (that is less than 50 subjects) and each individual is treated as a sample of N = 1; a modified t test described by Sokal and Rohlf (Reference Sokal and Rohlf1995) is used. Crawford analysis uses the t-distribution, rather than the standard normal distribution, to estimate the abnormality of the patient’s scores and to test whether it is significantly lower than the scores of the control sample. Crawford, Garthwaite, Azzalini, Howell, and Laws (Reference Crawford, Garthwaite, Azzalini, Howell and Laws2006) demonstrated this method is robust and less influenced by skew and leptokurtosis also when the control sample N is small.
Table 2. Individual patients’ results on the Experimental Tasks
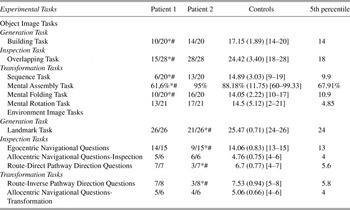
Note
Means, (SD), and [range] are reported for controls.
* Deficit performance according Crawford analysis.
# Deficit performance under the 5th percentile.
Patient 1 showed a deficit only on some tests involving the generation, inspection and manipulation of images of objects. In particular, his performance was significantly worse than that of the control group when he had to recognize an architectonic object among distracters (Building Task: t1,19 = −3.69; one-tailed p < .001), to inspect an image (Overlapping Task: t1,18 = −2.7; one-tailed p = .007), to decide whether a common object was the same one he had mentally assembled (Mental Assembly Task: t1,19 = −2.203; one-tailed p = .009), and when he had to mentally put together pieces of a previously seen picture (Sequence Task: t1,18 = −2.86; one-tailed p = .005). The patient performed similarly to the controls when he had to manipulate the whole image of the object (Mental Folding Task: t1,18 = −1.78, one-tailed p = .046; Mental Rotation Task: t1,19 = −0.27, n.s.).
Patient 1 had no difficulty performing any of the Environment Image Tasks (Landmark Task: t1,16 = 0.73, n.s.; Egocentric Navigational Questions: t1,16 = −0.06, n.s; Allocentric Navigational Questions-Inspection: t1,16 = 0.31, n.s.; Allocentric Navigational Questions-Transformation: t1,16 = −0.08, n.s.; Route-Direct Pathway Direction Questions: t1,16 = 0.38, n.s.; and Route-Inverse Pathway Direction Questions: t1,16 = −0.54, n.s.).
On the contrary, Patient 2 performed like the controls on the Object image tasks (Building Task: t1,19 = −1.63, n.s.; Overlapping Task: t1,18 = 1.026, n.s.; Mental Assembly Task: t1,19 = 0.56, n.s.; Sequence Task: t1,18 = −0.61, n.s.; Mental Folding Task: t1,18 = 0.85, n.s.; Mental Rotation Task: t1,19 = 0.49, n.s.) but performed deficiently on many Environment Image Tasks. In particular, he was unable to generate landmarks mentally (Landmark Task: t1,16 = −6.12, one-tailed p < .001), to inspect (Egocentric Navigational Questions: t1,16 = −5.98, p < .001; Route-Direct Pathway Direction Questions t1,16 = −4.67, one-tailed p < .001), or to manipulate the mental representation of a pathway (Route-Inverse Pathway Direction Questions: t1,16 = −4.67, one-tailed p < .001). Instead, Patient 2’s performance was comparable to that of the controls in both the Allocentric Navigational Questions-Inspection (t1,16 = 1.61, n.s.) and Allocentric Navigational Questions-Transformation (t1,16 = −1.56, n.s.).
DISCUSSION
The aim of this study was to shed light on the nature of the deficit in patients with representational neglect and to investigate whether representational neglect was affected by the content of the mental image the patients had to generate, inspect, and manipulate.
In particular, we submitted two patients with different types of representational neglect to a complex battery that assessed the different kinds of imagery processes. We found that Patient 1, whose performance on the O’Clock Test was asymmetric, performed poorly on some tasks involving the mental generation, inspection, and manipulation of objects (Building Task, Overlapping Task, Mental Assembling Task, Mental Folding Task, and Sequence Task) but not on other tasks involving the mental imagery of environments. On the other hand, Patient 2, whose performance was asymmetric on the Familiar Squares Description Test, performed poorly on tasks involving the mental generation, inspection, and manipulation of environments (Landmark Task, Egocentric Navigational Questions, Route-Direct Pathway Direction Questions, and Route-Inverse Pathway Direction Questions) but not on tasks involving the mental imagery of objects.
It could be that Patient 1’s poor performance on object image tasks was due to his perceptual neglect more than to his representational neglect. In fact, it can be hypothesized that the presence of perceptual neglect impeded him from perceiving the left side of stimuli, therefore, making it impossible for him to generate, inspect, or manipulate correctly the left side of mental images of the same stimuli. But why should perceptual neglect affect only some tasks? If the observed deficits were due to the patient’s inability to perceive the stimuli correctly, he would have shown a similar deficit in all imagery tasks. This was not the case, however, because Patient 1 performed all of the Environment Image tasks without any deficit. Furthermore, it should be noted that when we tested this patient he was enrolled in a rehabilitation program for perceptual neglect and was able to explore each stimulus correctly. A further demonstration that his defective performances depended on the presence of a specific imagery disorder and were not due to the presence of perceptual neglect was the absence of horizontal asymmetries in his defective performances. In the Mental Assembly Task he failed on both the horizontal and the vertical trials, and in the Sequence Task, when we analyzed the individual pieces arranged mentally in the right way, we found that the patient correctly placed the same number of pieces on the right and on the left (respectively, 15/31 pieces on the right, 15/31 on the left and 5/13 in the middle).
Patient 1 shows that representational neglect can affect only the mental representation of objects and spare the mental representation of environments and that the mental imagery process is not a single and undifferentiated ability. In fact, his performance was strongly related to the image content (objects vs. environments) as well as to the kind of mental imagery transformation required by the test. Patient 1 was able to mentally rotate, but was unable to fold stimuli and mentally assemble them. This pattern of performance was opposite to that of Riddoch’s patient (1990), who was unable to rotate images but was able to assemble them.
Patient 2 shows that in some cases representational neglect can affect the mental representation of environments and can spare the mental representation of objects. This patient was unable to generate an image to recognize previously seen landmarks and to inspect and transform the pathway images. The only Environment Images tasks that Patient 2 performed well were the Allocentric Navigational Questions-Inspection and the Allocentric Navigational Questions-Transformation, in which he had to generate the image of two landmarks, to inspect and then to manipulate them respectively. A possible explanation is that in both of these allocentric tasks landmarks were imaged as objects and not as pieces of an environment, because the tasks require making judgments and transforming objects that are not directly related to their environmental location or to their value as reference points in the environment. Moreover, it is possible to use previous semantic knowledge to solve this task correctly. In fact, when the subject has to decide whether the hat-stand is taller than the door he can use one of two strategies: image a mental comparison between objects encountered on the pathway (correct mental imagery task procedure) or refer to common sense and semantic knowledge. However, these latter interpretations may justify the correct performances on the inspection task, but not those on the transformation task, which fits better with the first one.
Patient 2’s deficit in generating an environment image (i.e., a cognitive map) can partially explain the difficulty in orienting in the environment that he spontaneously reported during the clinical evaluation.
It is interesting to observe the opposite performance of Patient 1, who failed to solve the Building task in which he had to recognize the picture of a previously seen building among three distracters, and of Patient 2, who failed to solve the Landmark task, which required recognizing previously seen real objects that functioned as landmarks. These data confirm the idea that landmarks acquired along a pathway have a specific and peculiar identity. The recognition of the picture of a building among very similar distracters (i.e., architectonic objects) is very different from the recognition of an object shown along a pathway (i.e., a landmark). These results are on line with Epstein and Kanwisher’s second experiment (1998), which demonstrated that the parahippocampal place area was significantly more active during the perception of familiar landmarks than during the perception of common objects. It could be, however, that this area was also active for the perception of buildings (Aguirre, Zarahn, & D’Esposito, Reference Aguirre, Zarahn and D’Esposito1998) and houses (Epstein & Kanwisher’s first experiment; 1998) that are not landmarks (i.e., never seen in the real environment), and, therefore, the recognition of architectonic objects and of landmarks could be supported by the same neuronal substrate. However, other regions not analyzed in these studies might show different patterns of activation with respect to landmarks and architectonic objects. One of these regions could be the retrosplenial cortex in which Epstein, Parker, and Feiler (Reference Epstein, Parker and Feiler2007) found a stronger response when subjects viewed familiar scenes (seen in the real environment) than when they viewed unfamiliar scenes.
Moreover, Janzen and van Turennout (Reference Janzen and van Turennout2004) showed that the peculiarity of a landmark is not its physical features but its spatial collocation in the environment. In particular, in subjects who viewed a route through a virtual environment with objects placed at decision or nondecision points, parahippocampal responses were stronger when the object was located at a decision point, demonstrating that only objects with a navigational-direction value become landmarks.
Taken together these data, in line with Piccardi and co-workers’s study (2008) describing a patient with imagery neglect but normal spatial working memory, indicate that representational neglect is not due to a working memory deficit (Beschin et al., Reference Beschin, Cocchini, Della Sala and Logie1997; Della Sala et al., Reference Della Sala, Logie, Beschin and Denis2004; Denis, Beschin, Logie, & Della Sala, Reference Denis, Beschin, Logie and Della Sala2002), because our patients would have failed on both the object and the environment images tasks, which involve the working memory system in the same way.
Our data agree with some studies interpreting specific navigational disorders in patients with representational neglect (Guariglia et al., Reference Guariglia, Piccardi, Iaria, Nico and Pizzamiglio2005; Nico et al., Reference Nico, Piccardi, Iaria, Bianchini, Zompanti and Guariglia2008; Piccardi et al., Reference Piccardi, Bianchini, Zompanti and Guariglia2008) as due to a deficit in specific systems for the mental representation of environments (i.e., a deficit in the ability to generate and use an internal representation of the environment).
Although it is unwise to draw conclusions from two single cases, our results, in line with functional MRI evidence (Ishai et al., Reference Ishai, Ungerleider and Haxby2000; O’Craven & Kanwisher, Reference O’Craven and Kanwisher2000) and recordings from single neurons (Kreiman et al., Reference Kreiman, Koch and Fried2000), show that, in the imagery domain, environments, and objects can be represented separately and disrupted independently. They also confirm Guariglia and Pizzamiglio’s theoretical interpretation (2006, 2007) that two different mental representation systems exist, one devoted to topographical images and human navigation and the other involved in object representation.
An alternative interpretation of our data is a dissociation between egocentric (Patient 2) versus allocentric (Patient 1) neglect in the imagery domain analogous to the dissociation reported in the perceptual domain by Hillis and co-workers (2005), who stated that parietal areas are involved in egocentric representation, while temporal areas are involved in allocentric representation. The two patients we present suffered from lesions that may, at least in part, correspond to those above reported. In fact, Patient 1 has a lesion involving the temporal lobe while in Patient 2 the lesion seems to spare the areas that Hillis and co-workers (2005) hypothesized to be involved in egocentric representation. However, following this interpretation, we should find that each patient failed in all the tasks requiring adopting one of these frames of reference. Instead, Patient 1 did not fail in both Environment tasks requiring an allocentric frame of reference, and Patient 2 did not fail in all the tasks requiring an egocentric frame of reference (including the cancellation Tests of the battery for neglect).
Present data are better explained by hypothesizing the existence of two separate systems processing the mental representation of the space near the body and the mental representation of the navigational space. Dissociated forms of neglect affect these two systems. In one case (Patient 1) a fronto-parieto-temporal lesion caused visuo-spatial neglect in peri-personal space accompanied by a representational neglect affecting the ability to generate, inspect and transform visual mental images of objects without affecting the processing of mental representation of environments. In the other case (Patient 2), a small frontal lesion caused a representational neglect affecting the ability to generate, inspect and transform visual mental images of environments without affecting the processing of mental representation of objects; this latter patient did not show any sign of visuo-spatial neglect in peri-personal space, but was affected by persistent difficulties in topographical orientation.
This interpretation is coherent with another hypothesis that different types of space exist, processed by different neural systems. The reported dissociation could be interpreted as a dissociation between impairments in spatial abilities at different scales of space (Hegarty, Montello, Richardson, Ishikawa, & Lovelace, Reference Hegarty, Montello, Richardson, Ishikawa and Lovelace2006), or also among different functional spaces (space of the body, space around the body, space of navigation; Tversky, Reference Tversky2003). In this view, present data confirm the existence of different functional spaces, namely the space near the body for which processing is selectively damaged in Patient 1, and the space of navigation for which processing is selectively damaged in Patient 2. The double dissociation between these two types of space suggests also that two independent neural systems exist.
ACKNOWLEDGMENTS
This study was supported by funding from MIUR (Cofin 2003), Ministero della Salute (RC 2004–2005), and the European Community (Eu 6th NEST Pathfinder Project: Wayfinding nr12959). Authors would like to thank Maria Caccetta for her support in collecting the data.









