Introduction
The success of radiotherapy depends on the accuracy, precision and conformity of the desired dose distribution over the tumour volume and organs at risk, that is the accurate delivery of the treatment as planned. The advanced technology medical electron linear accelerators have the capability of treating small and irregular lesions more precisely using megavoltage X-ray beams. These accelerators can be utilised for treating various types of cancer cases by advanced radiotherapy techniques such as beamlet-based intensity-modulated radiation therapy (IMRT), volumetric modulation arc therapy (VMAT), helical IMRT, high-precision stereotactic radiosurgery (SRS) and stereotactic body radiation therapy (SBRT). The use of advanced radiotherapy techniques offers conformal dose distributions and accurate dose delivery options. However, high degree of geometric accuracy is required in the effective implementation of these techniques and hence proper localisation of the target volume is an important component in such clinical practices. However, patients are not just rigid geometries and are not static over time. The main challenge in practicing advanced radiotherapy with tighter margins is the non-rigid geometries and non-static organs of the patients and hence tumour motion is one of the potential sources of error.Reference Keall, Mageras and Balter 1 , Reference Ishihara, Nakamura and Miyabe 2 The source of error may be due to respiratory, cardiac, digestive systems movement during the imaging or delivery.
SBRT is a technique that delivers focussed radiation to target in the body with minimal radiation to the surrounding healthy structures using stereotactic technique/apparatus. It is a highly conformal and precision radiotherapy method that makes it a better alternative than other radiotherapy techniques in a variety of cases. Usually, SBRT requires longer treatment time due to high dose per fraction. Hence, we should consider the intrafraction mobility of mobile targets in SBRT using real-time tumour tracking or gating techniques. However, if the target is not highly mobile, then, there is no need of tracking or gating during the treatment, and SBRT can be delivered continuously without any interruption.
In some of the cases such as lung cancer, where hypofractionated SBRT is thought to have attractive treatment outcomes, target motion is quite complex and prone to hysteresis.Reference Seppenwoolde, Shirato and Kitamura 3 However, the target motion must be accounted for to ensure the successful delivery of hypofractionated SBRT in lung cancer. In situations where target and critical structures cannot be identified in the images acquired for treatment planning because of their internal movement,Reference Benedict, Yenice and Followill 4 SBRT is not considered to be an effective option. The published literature indicates that the clinical outcomes of SBRT are very encouraging especially for stage-I non-small cell lung cancer (NSCLC) cases.Reference Simone and Dorsey 5 , Reference Zheng, Schipper and Kidwell 6 Motion-correlated computed tomography imaging is mainly used for lung cancer cases and it is a most important requirement in SBRT of lung. The use of conventional CT imaging for lung tumour imaging leads to several types of artefacts.Reference van der Geld, Lagerwaard, van Sörnsen de Koste, Cuijpers, Slotman and enan 7 , Reference Chen, Kung and Beaudette 8 The magnitude of these artefacts is influenced by many factors including scan time and the relation between the CT acquisition period and the respiratory cycle of the patient.
Movement due to respiration during volume acquisition results in two types of imaging errors. The first type of artefact occurs within an image slice due to X-ray projections acquired at different respiratory phases. The second type of artefact can be due to the limited axial field of view (AFOV) of a CT scanner. Sometimes, these artefacts may be similar to the disease which may lead to identification of an erroneous position, size, shape and volume of the target and in the identification of other regions.Reference Bettinardi, Picchio, Muzio, Gianolli, Gilardi and Messa 9 According to Shimizu et al.Reference Shimizu, Shirato and Kagei 10 tumour may disappear from axial slice in 21% of the images with this type of CT. The International Commission on Radiation Units and Measurements (ICRU) Report 62 has recommended the use of an internal target volume (ITV) to account for these variations. 11 There is the standard practice of using population-based standard concentric margin of 20–25 mm around the target for lung cancer treatments.Reference Giraud, Morvan and Claude 12 – Reference Giraud, De Rycke and Dubray 14 These concentric margins in all directions in the creation of planning target volumes (PTV) without considering the real mobility vector of the tumour may overestimate or underestimate the target motion and also results in the unnecessary irradiation of normal organ volumes.Reference Van Sornsen de Koste, Lagerwaard and Nijssen Visser 15 – Reference Underberg, Lagerwaard and Slotman 19 This is an important constraint for dose escalation in SBRT planning.
Most of the studies clearly demonstrated that the lung tumour motion is very complex and unpredictable in nature. Hence, patient-specific motion-correlated CT is highly essential for hypofractionated SBRT planning to identify the ITC. Slow rotation CT scanning, breath hold CT and 4D CT are some of the motion-correlated CT techniques. In 4D CT scan, images are acquired in all phases of the breathing cycle of a patient. Different 3D data sets can be derived using this 4D data in which each set represents a particular breathing phase of the patient. The clinician draws the gross tumour volume (GTV) in each phase and then, ITV can be derived by the union of all these volumes. This requires a lot of time and effort, however, the ITV can be accurately estimated using this method in line with target motion and also reduces the irradiation volume due to reduced PTV when compared with population-based concentric margins. Maximum- and minimum-intensity projections (MIP and MinIP) can be created using the 3D data. In MIP set, target volume is formed with maximum voxel content in 4D data, whereas in MinIP set target volume is created by using the lowest voxel content. As per the definition of MIP, the internal volume identified using this data set should coincide with the internal volume generated from the union of the GTVs of all of the breathing phases. If the tumour is highly mobile, then the MinIP target volume is small or zero. These intensity projections are very useful in different steps of planning SBRT treatment.
Accounting for target motion is important not only in imaging and treatment planning but also in dose delivery to the patient.Reference Schwarz, Cattaneo and Marrazzo 20 If the dose to the target volume is not delivered as per the dose distribution generated using treatment planning system, there may be a significant increase in the possibility of a geographic miss, the rate of serious complications/intolerable side effects. There are several real-time tracking methods available to reduce the impact of tumour motion during dose delivery.Reference Caillet, Booth and Keall 21 , Reference Uchida, Tachibana, Kamei and Kashihara 22 In respiratory gating method, radiation is delivered in a predetermined part of the breathing cycle in which target mobility is comparatively less. This is a very useful technique for the targets, which are highly mobile in nature. Reduction in the target volume is the major advantage in being able to escalate the dose to the tumour. However, gating is a time-consuming method and can cause patient discomfort during dose delivery. Patient breath arrest for preset time during the imaging and treatment is the basis for breath-holding techniques. This is done to reduce the target motion. This is a good method that allows imaging of the tumour without artefacts and errors and it also allows for a reduction in the target volume. Given the health status of some patients, it can be difficult to find suitable patients who are able to adapt this method of arrested breathing. Another approach is the use of tracking systems using fiducial markers implanted in the patient to delineate the tumour and allows monitoring of target motion continuously during delivery of the radiation dose. Fiducial implantation is an invasive procedure and motion correlated CT is required for imaging.
Treatment may be delivered without interruption if the target is not highly mobile or by using one of these methods. Identification of a suitable technique is also very important for patient comfort. Breath-holding technique can be used if imaging is with 4DCT and this imaging modality can be useful in selecting an appropriate treatment method for a given patient. If we evaluate and understand that the tumour is not highly mobile, then treatment can be delivered without any gap with proper creation of an ITV, otherwise, gating/tracking technique should be adopted to account for tumor mobility. Many articles describe the use Reference van der Geld, Lagerwaard, van Sörnsen de Koste, Cuijpers, Slotman and enan 7 , Reference Bettinardi, Picchio, Muzio, Gianolli, Gilardi and Messa 9 , Reference Underberg, Lagerwaard and Cuijpers 18 , Reference Underberg, Lagerwaard and Slotman 19 of 4DCT-based treatment planning. However, 4D CT-based intensity projections and their importance in the lung cancer treatment delivery and its use in the patient selection is not extensively discussed in the scientific literature. Our objectives of this study were threefold, namely (i) to evaluate the benefit in reducing the target volume with motion-correlated 4DCT when compared with population margin-based conventional CT, (ii) to estimate the accuracy of ITV created by maximum intensity projection (MIP) image when compared with the ITV based on the union of all the GTVs of respiratory phases and (iii) to find out the suitability of patient for gating technique based on MIPs and MinIPs data generated from 4DCT.
Materials and Methods
Twenty patient plans of stage-I NSCLC were analyzed in this study. All cases were treated by hypofractionated SBRT. Conventional CT and 4DCT scans were taken using a brilliance big bore CT unit (Philips Medical Systems, The Netherlands) as shown in Figure 1. 4DCT scans were carried out using a real-time position management system (Varian Medical Systems, Palo Alto, USA) and brilliance 4D imaging software. Twelve among 20 were lower lobe tumours. Only those cases were selected for this study involved with MIP, where the targets were not near to the thoracic wall and mediastinum as the 4DCT-based MIP data may overestimate the target volume.Reference Underberg, Lagerwaard, Slotman, Cuijpers and Senan 23 A marker block was placed on the patient’s thorax. The markers were focused by an infrared camera. Patient coaching was very important here to ensure breathing patterns were synchronized. The respiratory signals were recorded using infrared reflecting markers on the block during coached breathing. The 4D data sets were sorted out for 10 phase bins (0–90% phases). The entire breathing cycle represents 100% which is divided into 10 bins. Each bin gives voluble information of breathing correlated images of that particular phase.
Figure 1 4DCT facility.
All the CT data sets were then transferred to Eclipse treatment planning system (Varian Medical Systems, Palo Alto, USA). GTVs were contoured in all the data sets manually using lung window. The union of all volumes of GTVs in 10 phases was created and defined as ITVall phases. Three millimetre margin was given around the ITVall phases to account for geometrical uncertainties and the new volume was designated as PTVall phases. Similarly, PTV15mm was created by using conventional CT data set plus 15 mm margin around the ITV. These target volumes were compared in all patients. The MIP and MinIP of all the phases were determined using brilliance software, and ITVMIP was contoured in MIP data set. This indicates the volume of the target present at any point of time during the respiratory cycle. Similarly, ITVmin IP was identified in Min IP data which gives the volume of the target which is present in all the phases of respiratory cycle. The magnitudes of ITVall phases were compared with ITVMIP. The ratio of MinIP and MIP was calculated to decide whether a given patient could be treated with continuous SBRT or real-time position management-based gated SBRT.
Results and Discussion
Table 1 presents the volumes of PTV15mm and PTVall phases along with the ratio of PTV15mm to PTVall phases for the 20 patients included in this study. The ratio of PTV15mm to PTVall phases varies from 1·17 to 3·17 (p ᴝ 0) clearly indicating that large amount of normal tissue volume is covered by population-based PTV, that is PTV15mm. The average value of this ratio is 1·98, which means that PTV determined using population-based criteria is nearly double of the PTV determined using 4DCT method. This is due to the fact that the tumour motion in lung cancer cases is very complex, not isotropic involving mostly superior and inferior displacements.
Table 1 Comparison of planning target volumes (PTVs) created from population-based margin using conventional CT images (PTV15mm) and from all the phases of four-dimensional computed tomography images (PTVall phases). Also included in the table is the ratio of these two PTVs
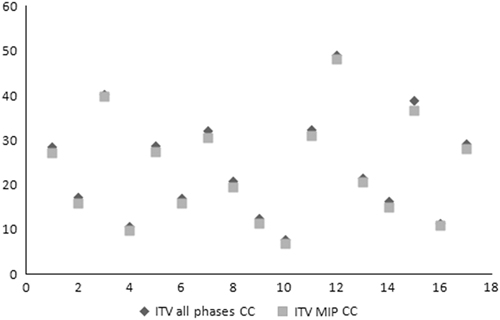
Graph 1 shows the data of ITVMIP and ITVall phases. Data of 17 patients were used to compare the ITV in MIP images because the tumours were very close to mediastinum in the remaining three cases and hence not considered. The average value of the ITVMIP to ITV all phases ratio is 1·06 with standard deviation of 0·028. That means most of the values are very close to the average. Thus, ITVs created from the union of images from all the phases to the ITVs created using MIPs are very close to each other. Finally, the ratio of intensity projections is calculated as shown in Table 2. In three cases, it was found to be zero indicating that there is no common volume of the target which is existing in all phases of 4DCT. This means that the tumours are highly mobile in these cases. We established a limit that, the ratio should be less than or equal to 0·35 (35% or one third) between both projections to estimate the considerable tumor mobility. Further, the ratio of intensity projections in six cases was found to be less than 0·35 indicating that the tumours have considerable intrafraction motion. This evaluation indicated that 9 out of the 17 patients were suitable for gated treatment available in our institute and they may benefit with this treatment approach even though this technique is time-consuming. These results are similar to some of the published data.Reference Underberg, Lagerwaard, Slotman, Cuijpers and Senan 23 , Reference Saito, Matsuyama and Toya 24 Two cases (0·32, 0·33) were very close to our fixed ratio. Still, we took them for gating because of their good cooperation. Continuous treatment (without gating) delivery method was used for the remaining eight patients as there was no extra benefit with motion management in these cases. Some systems like real-time position management (Varian Medical Systems, Palo Alto, USA), adapt gating technique, some systems with fiducial implants follow tracking technology and some other systems are based on breath hold technique like active breath coordinator (Elekta Oncology Systems Ltd, Crawley, UK) at the time of dose delivery. However, 4D CT is a common and important requirement irrespective of these techniques to identify the target without artefacts, to reduce the target volume and to identify the patients who can benefit from motion management during the dose delivery.
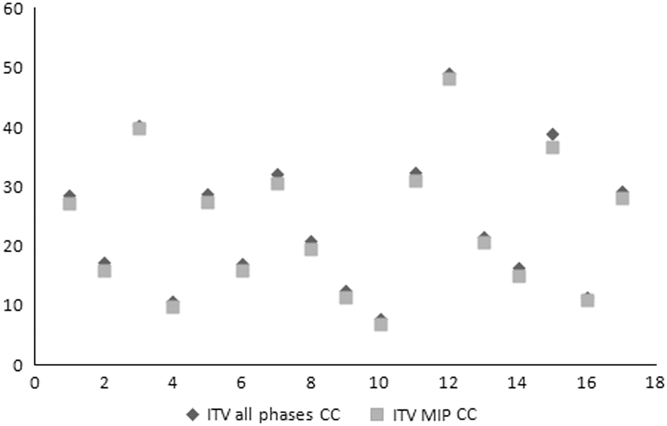
Graph 1 Comparison of ITVMIP and ITVall phases.
Table 2 Internal target volume internal target volume (ITV)MIP and ITVMinIP volumes and their ratio
Conclusions
This study supports that population-based margins should not be used for hypofractionated SBRT in stage-I NSCLC cases and the motion-correlated 4DCT is a definite requirement for the tumour delineation, treatment planning, and dose delivery. MIP is a reliable clinical tool for the quick generation of ITV for the stage-I NSCLC tumours. There are many advantages with 4DCT at different stages of SBRT. Motion-correlated 4DCT is common and important requirement, irrespective of different motion management methods. All SBRT patients who undergo 4DCT need not require motion management during dose delivery. This is proved clearly in this study. Motion management requirements for treatment delivery can be estimated easily and quickly based on the MIP and MinIP data. Patients who may be benefitted with motion management during dose delivery can be identified and preselected with 4DCT.
Acknowledgement
None.
Financial support
Nil.
Conflicts of interest
On behalf of all authors, corresponding author state that there is no conflict of interest.