


INTRODUCTION
Carbon fibre is widely used in radiotherapy due to the material’s high mechanical strength, low density, and radiotranslucence. These properties make carbon fibre an ideal material for providing rigid and lightweight patient support that does not interfere with the radiation beam. As a result the presence of the treatment couch is often ignored in treatment plan design and calculation.
A study by De Ost et al.Reference De Ost, Vanregemorter, Schaeken and Van den Weyngaert1 compared the transmission properties of three commercially available carbon fibre inserts over a range of photon energies. They found that attenuation of all three inserts was no greater than 1%, but noted a significant increase in surface dose for Co-60 and 6 MV beams. Higgins et al.Reference Higgins, Whitehurst and Morgan2 confirmed these findings and concluded that the carbon fibre inserts provided minimal attenuation of the radiation beam, but significantly decreased the skin sparing effect. McCormack et al.Reference McCormack, Diffey and Morgan3 studied the effect of gantry angle on the attenuation of a 6 MV photon beam by a carbon fibre insert. It was found that the attenuation ranged from 2% at normal incidence to almost 9% at an angle of incidence of 70°. They concluded that this could have serious implications for treatments requiring posterior oblique beams. Myint et al.Reference Myint, Niedbala, Wilkins and Gerig4 investigated the attenuation of 6 MV and 18 MV photon beams by a commercial carbon fibre couch and concluded that neglecting the attenuation of oblique beams could result in localised dose reductions up to 16%. Furthermore, the dose error could be significantly reduced if the carbon fibre couch was modelled in the treatment planning system (Theraplan Plus v3.8) by incorporating it in the planning computed tomography (CT) dataset.
In this study, the effect of the carbon fibre insert for the Varian ExactTM couch on the attenuation and build-up of 6 and 15 MV photon beams were examined. The attenuation over a range of posterior oblique gantry angles has been determined and the ability of a commercial treatment planning system (XiO, Elekta CMS Software, St. Louis, MO) to correctly model the couch attenuation investigated.
MATERIALS AND METHODS
Beam attenuation
The measurements to determine the beam attenuation produced by the carbon fibre insert were performed on a Varian Clinac iX linear accelerator using the arrangement shown in Figure 1. The carbon fibre insert consisted of a carbon fibre shell (approximately 2 mm thick) with a foam core. The accelerator treatment couch had carbon fibre side arms which could be moved to avoid beam interference.
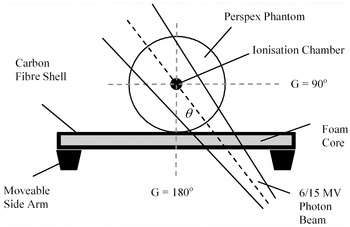
Figure 1. Schematic representation of experimental arrangement used to measure beam attenuation.
A digital electrometer (DOSE1, IBA Dosimetry, Germany) and a 0.6 cmReference McCormack, Diffey and Morgan3 Farmer ionisation chamber (NE 2571, Thermo, Berkshire) were used to obtain charge measurements. The chamber was placed in the centre holder of a 15 cm diameter cylindrical Perspex phantom, which was positioned on the couch such that the centre of the chamber was at the isocentre. Measurements were taken using a 10 × 10 cm field size and 200 MU exposures from both 6 and 15 MV photon beams.
The gantry angle was initially set to 180° so that the radiation field was normally incident to the carbon fibre insert, i.e., the angle of incidence, θ, was 0°. The gantry was rotated in 10° increments towards the plane of the couch with three charge readings taken at each position. At θ = 50° the side arms of the couch were repositioned to avoid interference with the radiation field. At θ = 60° a portion of the field passed through the edge of the carbon fibre insert, and at θ = 70° the field no longer fully intersected the insert so that a portion of the field was not attenuated. The procedure was repeated with the carbon fibre insert removed. The phantom was supported by two wooden bars positioned at either end so that they did not intercept the radiation beam. The attenuation factor was calculated as the ratio of the ionisation charge readings taken without and with carbon fibre in the beam.
Couch modelling on the treatment planning system
The experiment described above was simulated in CMS XiO, version 4.50. A CT dataset of the cylindrical Perspex phantom positioned centrally on the carbon fibre couch insert was acquired using on the Philips Brilliance wide bore CT scanner (Philips Healthcare, the Netherlands). The DICOM RT data was imported into the treatment planning system, where dose calculations were performed using both the Fast Fourier Transform Convolution (FFTC) and Multi-Grid Superposition (MGS) algorithms.Reference Miften, Wiesmeyer, Monthofer and Krippner5 Both algorithms compute the dose by convolving the total energy released per unit mass (TERMA) calculated at each point in the patient with Monte Carlo generated energy deposition kernels. FFTC is the faster of the two algorithms, but is less accurate because the FFT technique assumes kernel invariance in the convolution calculations. In the MGS model, the energy deposition kernels are modified according to the surrounding voxel density, making MGS calculations more accurate in the presence of heterogeneities. The treatment planning system calculations were initially performed with the couch insert excluded from the calculation region, and then repeated with it included.
Skin dose enhancement
The measurements to determine the skin dose enhancement produced by the carbon fibre insert were performed on a Varian Clinac iX linear accelerator using the arrangement shown in Figure 2. A digital electrometer and a parallel-plate ionisation chamber (Markus, PTW, Frieburg) were used to obtain charge measurements in a 10 × 10 cm field. The chamber was placed in a solid water phantom (Plastic Water, CIRS, Virginia) without any additional build-up. The depth dose was recorded from the surface to past the depth of maximum dose by adding additional sheets of solid water while maintaining a constant SSD of 100 cm. Five measurements were taken at each depth using 100 MU exposures for both 6 and 15 MV photons. The process was repeated with the carbon fibre couch insert placed in direct contact with the surface of the phantom.

Figure 2. Schematic representation of experimental arrangement used to measure dose in build-up region.
RESULTS AND DISCUSSION
Beam attenuation
The graphs in Figure 3 show the attenuation factors as a function of angle of incidence. There is a significant increase in beam attenuation as the angle of incidence increases, ranging from approximately 2% at 0° to 6% at 70° for 6 MV photons, and approximately 1.5% at 0° to 4% at 70° for 15 MV photons. This increase in attenuation occurs due to the increasing path length of carbon fibre that the beam traverses as the angle of incidence becomes more oblique. Posterior oblique treatment beams are commonly used in order to conform high radiation doses to target tissues and spare the surrounding normal tissues. Although the beam attenuation at normal incidence is minimal and could likely be ignored without consequence, ignoring the higher attenuation at oblique angles may result in localised dose errors that are clinically significant.

Figure 3. Ratio of measurements with and without carbon fibre in the beam as a function of angle of incidence for values measured experimentally and predicted by the treatment planning system at (a) 6 MV and (b) 15 MV.
Couch modelling on the treatment planning system
A correction strategy is required if the dose errors due to couch attenuation are considered to be unacceptable. One possible solution would be for the treatment planning system to account for the presence of the carbon fibre insert during routine dose calculations. To determine how well the treatment planning system models the couch attenuation, a comparison was made between the predictions of CMS XiO and measurements. The results are shown in Figure 3. The treatment planning system calculations using the FFTC algorithm significantly underestimates the attenuation at all angles for both 6 and 15 MV photon beams. The FFTC attenuation values exhibit a systematic absolute error of approximately –2% at 6 MV and –1.5% at 15 MV. The MGS attenuation values demonstrate better agreement with the experimentally measured values, exhibiting an absolute error of no greater than –0.5% for all angles, with the exception of θ = 70° for the 6 MV photon beam (–0.9%). The errors observed using FFTC are unacceptable and use of MGS is required to adequately model the beam attenuation produced by the couch insert.
Couch modelling on the treatment planning system is a desirable solution because the attenuation of each beam is corrected according to the specific beam geometry and without the requirement to input correction factors manually. The dosimetric effects of the couch insert would also be reflected in the dose distribution, which may be especially useful for beams that only partially intersect the couch. However, there are practical issues which must be considered for this to be a viable solution. First, it would be necessary to devise a method to include the carbon fibre couch insert in the patient CT dataset. This would require the development of software to replace the CT couch with the carbon fibre insert on the original patient CT dataset. Second, it may be necessary to index the patient to the couch in order to ensure that their lateral position at treatment was the same as on the planning CT. An alternative and perhaps more practical solution would be to tabulate attenuation correction factors over a range of gantry angles. The appropriate factor would then be selected from the table, according to the beam energy and gantry angle, and applied as a bulk correction to the monitor units. However, such correction factors should be applied with caution. Highly oblique beams may only be partially attenuated by the couch insert and there is the potential to overdose tissues in the unattenuated portion of the beam. Manual entry of correction factors provides a practical solution to correct for couch attenuation in static beam treatments, but is not a viable correction strategy for the emerging arc based treatments such as volumetric modulated arc therapy (VMAT) and RapidArc. Here, radiation can be delivered over a full 360° rotation of the accelerator gantry and a significant portion of the treatment arc will pass through the couch. Therefore, couch attenuation is likely to be significant effect and treatment planning system based couch modelling appears to be the only sensible solution for these treatment deliveries.
Skin dose enhancement
Parallel-plate ionisation chambers yield inaccurate measurements in the build-up region of high energy photon beams due to perturbations arising from their finite volume.Reference Nilsson and Montelius6,Reference Gerbi and Khan7 The perturbation effects increase the ionisation in the chamber cavity leading to a characteristic “over-response”. Gerbi and KhanReference Gerbi and Khan7 quantified the “over-response” of a Markus chamber by comparison with an extrapolation chamber, considered to be the gold standard for measurements in the build-up region. From this data, they proposed a correction strategy to allow the accurate measurement of dose in the build-up region. All measurements made here have been corrected according to the guidelines proposed by Gerbi and Khan.Reference Gerbi and Khan7
The graphs in Figure 4 show the ionisation measurements, corrected for the “over-response” of the Markus chamber, expressed as percentage depth dose normalised to the depth of maximum dose (d max). The dose in the build-up region was affected in two ways when the carbon fibre insert was present: (i) there was a large increase in surface dose, and (ii) the position of d max moved towards the surface. This is because the carbon fibre acted as bolus, producing a fluence of secondary charged particles, shifting the build-up curve towards the surface of the phantom. This is clearly illustrated by the data in Table 1.

Figure 4. Percentage depth dose curves with and without carbon fibre in the field for (a) 6 MV and (b) 15 MV photon beam.
Table 1. Effect of carbon fibre insert on skin dose and dmax for 6 and 15 MV photon beams

The term “skin dose” is defined by the ICRU8 as the ratio of dose at 0.5 mm to the dose at d max.
It should be noted that use of the carbon fibre couch insert will significantly decrease the skin sparing effect attributed to high energy photon beams. However, the clinical significance of this effect is uncertain. The tolerance dose for skin is considered to be around 55 to 60 Gy for conventional 2 Gy daily fractions.Reference Emami, Lyman, Brown, Coia, Goitein, Munzenrider, Shank, Solin and Wesson9,Reference Van der Kogel and Steel10 It is considered highly unlikely that the use of the carbon fibre insert will elevate skin doses to such dose levels for typical treatment techniques.
CONCLUSION
This study investigated the influence of the carbon fibre insert for the Varian ExactTM couch on the attenuation and build-up of 6 and 15 MV photon beams. Attenuation increased significantly with increasing angle of incidence, reaching values of 6% and 4% at 70° for 6 and 15 MV beams, respectively. It is concluded that it may not be appropriate to neglect couch attenuation for all beam geometries and a correction strategy may be needed. Further work is required to study the effect of ignoring couch attenuation on clinical treatment plans. In addition, it has been shown that it is possible to model the couch attenuation on the treatment planning system by including the carbon fibre couch insert in the planning CT dataset. The success of this approach will depend on the calculation algorithm employed. Practical issues regarding the insertion of the treatment couch in planning CT datasets and patient-couch indexing would need to be resolved to permit routine use of such a correction strategy. Finally, the carbon fibre couch insert significantly decreased the skin sparing effect. Skin dose was approximately three times as large when the couch insert was added to 6 and 15 MV photon beams. The clinical significance of this effect is unclear.
Acknowledgements
The authors thank Mr. Robert Brackenridge for his assistance with data collection and analysis for this study. The authors also thank Mr. Alan Rogers for manufacturing the Perspex phantom.





