Introduction
The management of upper airway obstruction due to bilateral vocal fold paralysis presents a challenge to the otolaryngologist. Sufficient airway patency needs to be balanced against quality of voice. A number of surgical techniques have been described which aim to avoid the need for a tracheostomy. In recent years, external techniques have been superseded by endoscopic approaches. These include Thornell's arytenoidectomy by electrocautery,Reference Thornell1 Ossoff and colleagues' CO2 laser arytenoidectomy,Reference Ossoff, Duncavage and Shapshay2 Dennis and Kashima's CO2 laser posterior cordectomy,Reference Dennis and Kashima3 and Kashima's transverse cordotomy.Reference Kashima4
The objective of this study was to describe our experience with a simple modification of the classical endoscopic laser technique. To the best of our knowledge, this is the first series to describe the use of a simultaneous release procedure (bilateral transverse posterior cordotomy) as a primary treatment for bilateral vocal fold paralysis.
Patients and methods
Nine patients with bilateral vocal fold paralysis underwent simultaneous bilateral posterior vocal fold release (transverse cordotomy) using the CO2 laser. All procedures were performed by the two senior authors (APC and ARN).
Each procedure was performed using suspension microlaryngoscopy, under general anaesthesia, and utilising a laser-resistant, cuffed endotracheal tube. The posterior half of the vocal folds and the posterior commissure were exposed by displacing the tube anteriorly with the laryngoscope. The operating microscope was set at a focal length of 400 mm, coupled to a CO2 laser micromanipulator and the AcuBlade linear incision computerised robotic beam (laryngeal protocol at 10 W continuous mode). Laser precautions were taken, which included using moist neurosurgical pledgets in the subglottis to protect the trachea and the endotracheal tube.
A simple incision (performed on both vocal folds in the same sitting) was commenced anterior to the vocal process of the arytenoid, and was then carried laterally in a curvilinear fashion through the entire thickness of the vocal fold (Figure 1), thus skirting the cartilage. The end-point of the procedure was reached when the vocal fold was seen to be completely released from the vocal process of the arytenoid (Figure 2), at which point the augmentation to the airway became apparent at the posterior glottis. All treated areas were cleansed with moistened pledgets to remove laser char, and all patients received intravenous dexamethasone peri-operatively.

Fig. 1 Diagram showing bilateral transverse cordotomy.

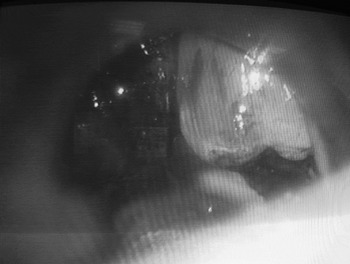
Fig. 2 Intra-operative photograph showing laser cordotomy.
Patients were kept in for overnight observation, but were generally discharged home within 24 hours of their operation (in the absence of any airway or swallowing difficulties), to be reviewed in the out-patient department within four to six weeks. The airway was assessed by pre- and post-operative flexible laryngoscopy or stroboscopy (Figure 3). No granulomas were observed in this series.

Fig. 3 Post-operative stroboscopic view, eight weeks after cordotomy.
Patients' voices and quality of life after the procedure were also assessed. Voices were subjectively analysed using the Voice Symptom Scale, the total score for which ranged from zero (i.e. a perfect voice) to 120 (i.e. a very poor voice).Reference Wilson, Webb, Carding, Steen, MacKenzie and Deary5 Patients' quality of life after the operation was assessed using the revised University of Washington Quality of Life questionnaire,Reference Weymuller, Alsarraf, Yueh, Deleyiannis and Coltrera6 which focuses on physical, social and emotional function; the maximum (best) score is 100 and the minimum is zero.
Results
The nine patients undergoing the procedure were aged from 27 to 85 years, and comprised three men and six women. The duration of their bilateral vocal fold palsy at the time of their operation varied from one to three years (mean two years). The causes of this condition in these patients are summarised in Table I. Three of the patients had presented originally with marked stridor requiring an emergency tracheostomy; the remaining six had mild stridor on exertion. No procedure had been performed on the vocal folds prior to transverse cordotomy in this series. Pre-operatively, the voice was considered to be good in five patients and impaired in four patients. Swallowing was normal in seven of the nine patients pre-operatively. All patients felt their activities were restricted because of breathing difficulties due to their condition.
Table I Causes of bilateral vocal fold palsy in study patients

Bilateral laser cordotomy procedures were carried out between May 2005 and March 2008. The CO2 laser was used in all patients. All patients were admitted for overnight observation, and all were discharged home the next day.
There was a single complication in this study group, in a patient who developed breathing difficulty 48 hours after the procedure and had to be readmitted. He improved with antibiotics and steroids, and was observed for any worsening of dyspnoea for six days in hospital. On admission, the posterior half of the vocal folds (i.e. the operated site) was swollen; this settled with conservative treatment.
None of the patients required post-operative tracheostomy, and all three patients with a previous tracheostomy were successfully decannulated within one month of their operation.
The follow-up period for this study group ranged from three months to four years (mean 28 months). Post-operatively, the airway was found to have improved in all patients, and none needed a second operation to improve their airway further. As regards the voice, seven of the nine patients felt their voice was better than before the operation, one felt it was the same and one felt it was worse. One patient required referral to the speech therapy department. No patients reported any change in swallowing. Peak flow measurements were not performed in this study.
The Voice Symptom Scale and quality of life questionnaires could only be completed for seven of the nine patients in this retrospective series, since unfortunately two had died by the time of this study due to unrelated causes. The total Voice Symptom Scale scores for the seven surviving patients were 28, 30, 32, 37, 45, 83 and 99, out of a total score of 120. The total Voice Symptom Scale score was on the low side in the majority of patients, indicating good voice from the patients' perspective.
The cumulative quality of life scores for the seven surviving patients in this series were 100, 97.5, 88.3, 83.3, 80, 66 and 61.1 per cent. Thus, quality of life was scored high by the majority of patients, indicating a good outcome in most patients in this small series. Patients graded their overall quality of life as outstanding (one patient), very good (two), good (one), fair (two) and poor (one).
Discussion
Bilateral vocal fold paralysis is potentially a life-threatening condition. Surgical intervention is frequently required to prevent acute asphyxiation or chronic airway obstruction. Surgery aims to improve the patient's airway, while at the same time avoiding a breathy voice or an incompetent larynx.
Many techniques have been devised which attempt to avoid the morbidity associated with a permanent tracheostomy by surgically enlarging the glottic aperture. These comprise extralaryngeal as well as endoscopic approaches, and commonly involve some form of laser arytenoidectomy or posterior cordectomy.
Although arytenoidectomy may produce an adequate airway, it is hampered by technical difficulties, such as poor visualisation of the muscularis process and troublesome bleeding, and risks the development of posterior laryngeal webbing and aspiration.
Steiner and Ambrosch reported performing endoscopic posterior cordectomy using the laser as long ago as 1985,Reference Steiner and Ambrosch7 using a technique which involved removing a 5 mm wedge of tissue from the posterior end of the true vocal fold. Dennis and Kashima followed with a report of results for a similar procedure,Reference Dennis and Kashima3 and many modifications have since been described. Kashima was the first to introduce the concept of unilateral transverse cordotomy.Reference Kashima4 This was followed by Wang and colleagues' description of a unilateral procedure using scissors performed in four patients, with good airway results.Reference Wang, Zhou and Xu8 Bosley et al. also described a unilateral approach,Reference Bosley, Rosen, Simpson, McMullin and Gartner-Schmidt9 while another groupReference Laccourreye, Paz Escovar, Gerhardt, Hans, Biacabe and Brasnu10 reported performing cordotomies but had in actual fact performed classical cordectomies (according to their methodology section details).
• Bilateral transverse cordotomy is a reliable treatment option for bilateral vocal fold paralysis, which aims to avoid the morbidity associated with a permanent tracheostomy
• The overall results for airway patency are good; the technique also preserves voice quality and avoids swallowing problems
• This is a simple operation which improves the quality of life for a group of patients with a potentially highly debilitating condition
Most of the patients in our series also achieved a good quality of life after the procedure. This is in complete agreement with many previous studies, which reported that preservation of the anterior vocal fold allowed sufficient airway enlargement while safeguarding voice quality. In addition, our method avoids debilitating problems with aspiration, as do most other cordectomy techniques which respect the integrity of the arytenoids and posterior commissure. Our technique for augmenting the glottic aperture differs from that of others, however, in its simplicity, and in the fact that it maximises the preservation of precious vocal fold mucosa while minimising the risk of complications. The use of a simultaneous ‘bilateral’ procedure ensures an adequate airway, created in a single operation and with a short hospital stay.
Conclusion
Bilateral transverse cordotomy is a reliable treatment option for patients with bilateral vocal fold paralysis, which aims to avoid the morbidity associated with a permanent tracheostomy. The overall results for airway patency are good, while the technique preserves voice quality and avoids swallowing problems. This is a simple operation which improves the quality of life for a group of patients with a potentially highly debilitating condition, and deserves to be made more widely available where appropriate facilities allow.