


Introduction
Salivary stones have a prevalence of 1.2 per cent.Reference Rauch, Gorlin, Gorlin and Goldmann 1 , Reference Sigismund, Zenk, Koch, Schapher, Rudes and Iro 2 One in 10 000–30 000 patients experience symptomatic swelling and pain in a salivary gland because of stones.Reference Marchal and Dulguerov 3
Today, diagnosis of sialolithiasis is conducted using brightness mode sonography.Reference Marchal and Dulguerov 3 – Reference Zengel, Schrotzlmair, Reichel, Paprottka and Clevert 7 This examination is inexpensive, poses no radiation exposure, is usually easily available and can be performed in a timely fashion. These are the advantages of sonography over other radiological imaging methods such as computed tomography (CT), sialo-magnetic resonance imaging (sialo-MRI) and sialography.Reference Schwarz, Kabbasch, Scheer, Mikolajczak, Beutner and Luers 4 , Reference Katz, Hartl and Guerre 6 , Reference Zengel, Schrotzlmair, Reichel, Paprottka and Clevert 7 Using ultrasound, the stone's current location, the stone's size and the state of function (e.g. gland duct obstruction) can immediately be assessed.Reference Gritzmann, Rettenbacher, Hollerweger, Macheiner and Hubner 8 , Reference Orlandi, Pistorio and Guerra 9 The choice of therapy depends on the location, visualisation and size of the stones. The pursuant success of the therapy can be verified using sonography.
Successful detection of the salivary stones in brightness mode ultrasound depends on pertinent anatomical knowledge concerning the salivary glands on the part of the examiner, and the detection rate increases with examiner experience.Reference Gritzmann, Rettenbacher, Hollerweger, Macheiner and Hubner 8 , Reference Orlandi, Pistorio and Guerra 9 The criteria for the diagnosis of sialolithiasis on a grey-scale image are a typical hyperechogenic structure with an acoustic shadow, occurring in a typical anatomical location in the salivary glands. Obstruction of the salivary system by ductal calculi can cause proximal dilatation of the ducts, swelling and pain.
Visualisation of the stones proves particularly challenging in the efferent ducts, yet can be accomplished with simple means. Diagnostic tools utilised for the visualisation and diagnostic analysis of salivary stones are described below.
Oral finger palpation
This method is suitable, especially in cases of small stones along the submandibular duct.Reference Patel, Hashemi and Joshi 10 Via palpation, a swelling can be felt out at the base of the mouth. In ultrasound, the calculus is seen as a focal area of increased echogenicity anterior to the easily recognisable curve of the finger in the base of the mouth. The stone can be confirmed by palpation as well as ultrasound.
Salivary gland probe insertion
By inserting a salivary gland probe (Bowman probe), the course of a salivary efferent duct can be visualised by following the slowly advancing probe, which can easily be displayed with ultrasound. If a resistance is found in the duct, the stone can be palpated with the probe, which facilitates a reliable representation of even tiny stones. If the probe finds a resistance in the salivary duct without a characteristic hyperechogenic focus with acoustic shadowing, duct stenosis has to be considered as a differential diagnosis.
Sialagogue use
In cases of a duct obstruction, a sialagogue taken immediately preceding ultrasound examination will cause the duct to fill with saliva proximal to the obstruction. The obstructed ducts can usually be followed from the gland all the way to the stone or duct stenosis.
Sono-palpation
Sono-palpation can be utilised, especially for an obstructed parotid duct. By modifying the contact pressure of the ultrasound probe, the duct can be identified because it collapses under compression. Sono-palpation of the submandibular duct is performed as described above, by utilising the palpating finger.Reference Patel, Hashemi and Joshi 10
Twinkling artefact
To our knowledge, this is the first study to investigate the ‘twinkling artefact’ in the diagnosis of salivary stones. This phenomenon was first described by Rahmouni et al., in diagnosing kidney stones, in 1996.Reference Rahmouni, Bargoin, Herment, Bargoin and Vasile 11 It is possible to identify even small stones (in the kidney) based on an artefact in the colour Doppler mode. The twinkling artefact is a colour Doppler reverberation artefact that may occur on surfaces with rigid impact echoes (e.g. at calcifications of the liver and aorta, and in the case of kidney stones and ureteral calculi).
Materials and methods
Using a model, 20 salivary stones of varying size, which had previously been removed through sialendoscopy, were put into a glass bowl filled with ultrasound gel at varying depths. The stones were investigated using a GE Logiq S8 ultrasound unit (General Electric Healthcare, Glattbrugg, Switzerland) with a 6–15 MHz matrix linear array transducer. The twinkling artefact was triggered by selecting suitable parameters on the ultrasound unit. The colour Doppler box was centred narrowly, directly on and behind the calculus. The threshold level was gradually increased until twinkling on the sialolith became visible. This investigation involved both the colour and power Doppler modes. All ultrasound investigations were performed by one experienced examiner and retrospectively graded by two experienced sonographers.
Following this pre-test, patients with symptomatic salivary stones were diagnosed using brightness mode sonography, and then examined using the power and colour Doppler modes. These patients were presenting at our clinic for extracorporeal shock wave lithotripsy, for scheduled salivary stone therapy. After obtaining the approval of the Research Ethical Board of Switzerland, 28 patients (13 females and 15 males), with a mean age of 47.7 years (range, 15–74 years), who had previously been confirmed to have sialolithiasis on brightness mode ultrasound, were examined. Salivary stones that were difficult to locate because of their anatomical location were visualised using above-mentioned resources.
The distribution of the 28 stones in these 28 patients (with 1 stone each) is depicted in Figure 1. We found two stones in the parenchyma, four stones in the proximal hilum and three stones in the distal efferent duct of the parotid gland. In addition, we found six stones in the parenchyma, nine stones in the proximal hilum and six stones in the distal efferent duct of the submandibular gland. The average calculus size was 6.48 mm (range, 2.4–16 mm).
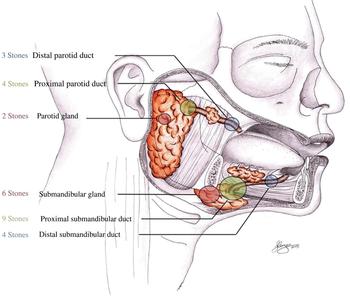
Fig. 1 Location and number of salivary stones in 28 patients.
The calculi of the 28 patients thus verified in vivo were investigated in regard to the stones’ twinkling behaviour, using the same settings on the above-mentioned ultrasound unit as determined in the model pre-test. The twinkling artefact was differentiated into four intensity levels ranging from 0 to 3, where 0 meant ‘no twinkling’, 1 represented ‘weak twinkling’ (twinkling on up to one-third of the stone), 2 reflected ‘medium twinkling’ (twinkling on up to one-half of the stone) and 3 meant ‘intense twinkling’ (twinkling on the entire stone). Patient age and gender, the location and size of the stones, and the Doppler settings, were also recorded and evaluated.
The twinkling artefact was utilised to show examination outcomes and to identify salivary stones. Figure 2a and 2b show the twinkling behaviour of a sialolith in the model test with colour Doppler and power Doppler.

Fig. 2 Stone in vitro in (a) colour Doppler mode and (b) power Doppler mode immediately following extraction.
Results
In vitro pre-test
Switching the cross beam mode on and off, and varying the depth of the salivary stones in the ultrasound gel, demonstrated no influence on the twinkling behaviour of the stones.
The following settings of the Doppler mode proved suitable: the pulse repetition frequency was set at 1 KHz, and the frequency in the Doppler mode was set at 5 MHz.
The twinkling artefact could be observed on all 20 stones in the model test. Even small stones (1–2 mm) would flash (Figure 3), particularly in the power Doppler mode in the ultrasound gel. Hence, this method proved suitable even as a screening method for the detection of salivary stones in the model.

Fig. 3 Salivary stone sized 0.13 cm in vitro (power Doppler mode).
In vivo investigation
Using the Wilcoxon matched-pairs rank sum test, we compared the intensity levels of twinkling (ranging from 0 to 3) between power and colour Doppler modes, in patients. The power Doppler mode showed a significantly higher level of intensity than the colour Doppler mode (p < 0.0001; Figure 4).

Fig. 4 Twinkling intensity of the stones using colour versus power Doppler modes.
Twenty-six of the 28 stones (93 per cent) could be detected using the power Doppler mode and 12 of the 28 stones (43 per cent) could be visualised using the colour Doppler mode. Twenty-seven of the 28 stones (96 per cent) could be represented using the colour and power Doppler modes in combination (Figure 5). One stone could only be represented using the colour Doppler mode. Another stone was not visible in either the colour Doppler mode or the power Doppler mode.

Fig. 5 Number of stones that exhibited twinkling using colour Doppler, power Doppler and both modes in combination, in 28 patients.
Identification of twinkling artefacts was more challenging in patients than in the model test because the pulse repetition frequency had to be set very high in patients in order to eliminate vascular signals. The ease or difficulty of visualising the stones depended on the surrounding tissue structure. By modifying the power Doppler angle, different parts of the stone, particularly the part with the largest reflection area, could be visualised more easily. For testing the detectability of the stone, the Doppler box was steered in a ventral and dorsal fashion over the stone, which showed the twinkling artefact only above the stone (Figure 6a–6c). With increased investigator experience, the twinkling artefact could be triggered more easily, by modifying the parameters during the Doppler investigation.

Fig. 6 Doppler box, with identical power Doppler settings, was steered in a dorsal fashion over a stone (a), was aligned on a stone with twinkling (b), and was steered in a ventral fashion over a stone (c) in the gland's hilum of the same submandibular gland on the right side.
Discussion
We found that salivary stones can be visualised using colour and power Doppler modes, both in vivo and in vitro. In our initial model test, a twinkling artefact could be triggered on all stones. Particularly in the power Doppler mode, even small salivary gland calculi, 1–2 mm in size (Figure 3), could be detected using default settings. The in vivo investigation showed that triggering the twinkling artefact in the patient is more challenging. It was necessary to modify ultrasound Doppler parameters such as the pulse repetition frequency threshold individually for each patient, with the unit's lowest possible Doppler frequency of 5 MHz as a constant factor proving most suitable for imaging.Reference Gao, Hentel and Rubin 12
The decreased visualisation of the stones in vivo compared to those in vitro could be explained by the following theories. The propagation of ultrasound waves in ultrasound gel proves optimal in vitro. By contrast, different tissue properties are found in vivo, such as an increased degree of tissue fibrosis as a result of recurring inflammation around the stone. In addition, according to the trapped bubble theory, the twinkling artefact is triggered by micron-sized bubbles that are trapped in the stone;Reference Jamzad and Setarehdan 13 a stone embedded in ultrasound gel is likely to exhibit more surroundings-related bubbles because it was in free air before being brought into the gel.
The power Doppler mode proved superior to the colour Doppler mode for visualising the stones (Figure 4). The question of why the power Doppler mode showed the stones more frequently and intensely in our investigation is beyond the scope of this study. The emergence of the twinkling phenomenon has been controversial in the literature and has not been clarified conclusively.Reference Rahmouni, Bargoin, Herment, Bargoin and Vasile 11 , Reference Jamzad and Setarehdan 13 , Reference Hassani, Raynal, Spie, Daudon and Vallee 14 By modifying the power Doppler's impact angle on the stone, the impact surface of the ultrasound waves on the stone was observed to play a role in the visualisation of the stone. One stone could not be visualised. A possible explanation is that the stone might have had a different morphological composition.Reference Jamzad and Setarehdan 13 , Reference Chelfouh, Grenier, Higueret, Trillaud, Levantal and Pariente 15
Although our study only comprised 28 patients, the results in regard to gender distribution, stone size and the distribution of the stones in the glands, matched those of a study by Sigismund et al.Reference Sigismund, Zenk, Koch, Schapher, Rudes and Iro 2 Salivary glands have been investigated using colour Doppler before; however, the focus has never been on the twinkling artefact.Reference Mansour, Stock, Chaker, Bas and Knopf 16 Similar to our investigations, the twinkling phenomenon has been successfully applied in the field of nephrology, for diagnosing kidney stones and ureteral calculi, both in vivo and in vitro.Reference Hassani, Raynal, Spie, Daudon and Vallee 14 , Reference Chelfouh, Grenier, Higueret, Trillaud, Levantal and Pariente 15 , Reference Andrulli, Turrin, Bigi, Ravani, Trinchieri and Locatelli 17 –Reference Tsao, Tyan, Kang, Kueng, Lan and Su 23
To our knowledge, no comparable investigations concerning salivary stone detection by means of colour and power Doppler modes exist in the literature. The investigation and verification of the concrements in former studies was performed by sonographers using brightness mode ultrasound only. This study aimed to delineate the twinkling phenomenon on salivary stones; hence, we paid attention to the fact that the stones could be clearly identified, even in the sonographic brightness mode, based on their typical ultrasound criteria. The 28 patients were recruited prior to extracorporeal shockwave lithotripsy in our clinic and, thus, we had a pre-selected group of patients with stones confirmed via brightness mode ultrasound. This is why we did not consider performing further imaging (CT or sialo-MRI) or invasive tests (sialendoscopy).
-
• Imaging of salivary stones poses a challenge, even to experienced examiners
-
• Sonography is suitable for diagnosing sialolithiasis and determining treatment
-
• Treatment options for salivary gland stones include extracorporeal shockwave lithotripsy and sialendoscopy
-
• This paper describes the role of the ‘twinkling artefact’ for detecting salivary stones
-
• Doppler mode sonography is a novel option for visualising salivary gland stones
-
• The twinkling artefact is a very reliable sign for diagnosing sialolithiasis
All ultrasound examinations (brightness mode, power Doppler mode and colour Doppler mode) were performed by one experienced examiner only. This had the advantage that consistent results could be achieved; however, there is the disadvantage that results might be worse for other, more inexperienced examiners.
Another limitation of the study was the fact that the examinations were performed with only one ultrasound unit. Aytac and Ozcan stated that the twinkling phenomenon heavily depends on the settings and type of Doppler system,Reference Aytac and Ozcan 24 and, thus, on the type of device.Reference Jamzad and Setarehdan 13 , Reference Aytac and Ozcan 24 , Reference Wang, Li, Xiao, Shi and Zhang 25 It is therefore likely that the exact settings of the device used in our tests cannot be transferred to other devices. However, the ultrasound unit used in this study is the latest generation of its type. Furthermore, based on various examinations of kidney stones with different devices, by different examiners, it can be inferred that the twinkling phenomenon will be repeatable in the case of salivary stones as well.Reference Ripolles, Martinez-Perez, Vizuete, Miralles, Delgado and Pastor-Navarro 20
Further studies involving greater numbers of cases, performed by different examiners, using different ultrasound units, are necessary to confirm the value of the twinkling artefact for the investigation of salivary stones. Future studies should also focus on the application of colour and power Doppler mode examinations for screening salivary stones, comparable to their application in kidney stones.Reference Turrin, Minola, Costa, Cerati, Andrulli and Trinchieri 26 This will increase sensitivity and improve confirmation of small salivary stones in particular.
Conclusion
Sonography is a suitable method for the diagnosis of sialolithiasis. We demonstrated that even small stones or stones located in the distal salivary ducts can be diagnosed easily using systematic verification via the twinkling artefact. The twinkling artefact is thus an interesting and promising approach for the detection and confirmation of salivary stones.
Acknowledgement
We would like to express our gratitude to Dr H Friedrich at the University Hospital Berne, Switzerland, who kindly produced and provided the schematic drawing of the salivary glands (Figure 1) specifically for this publication.






