


Introduction
A new classification system of attic retraction pockets uses: otoscopic and endoscopic visualisation of the fundus of the attic retraction pocket, the ossicular status in the attic, the degree of scutal erosion, and the presence of cholesteatoma.Reference Vijayendra, Mahajan, Vijayendra and Ramdass1 This new system classifies attic retraction pockets precisely, and incorporates all visible pathology while documenting the extent of destruction. In the lowest grade, grade I, the pars flaccida is only dimpled, but not retracted towards the malleus. In the highest grade, grade V, there is extensive retraction, with complete erosion of the lateral wall of the epitympanum, ossicular necrosis, erosion of the lateral semicircular canal, and possible middle cranial fossa dura exposure.
During decades of treating patients with tympanic membrane retractions, we began to suspect that negative pressure in the middle ear was contributing to retraction formation. Other authors had noted tympanic membrane retractions after sniffing – a manoeuvre that creates negative nasopharyngeal pressure.Reference Kobayashi, Yaginuma, Takahashi and Takasaka2,Reference Falk and Magnuson3 We therefore hypothesised that the middle-ear pressure changes after negative nasopharyngeal pressure (sniffing) would be more marked in ears with attic retraction pockets than in normal ears.
Additionally, it is well recognised that the pars flaccida is the weakest portion of the tympanic membrane.Reference Mansour, Mansour, Magnan, Haidar, Nicolas and Louryan4 Moreover, the dynamics described by LaPlace's law contribute to this differential retraction, which ultimately forms an attic retraction pocket: LaPlace's law states that the pressure within a sphere varies with the inverse of the radius.Reference Thiriet and Thiriet5 Therefore, in the tympanic cavity, air within the smaller epitympanic region should evacuate more readily than air in the larger middle-ear space.6 Our discussion will go into further depth, relating negative nasopharyngeal pressure, tympanic membrane composition and LaPlace's law to attic retraction pocket formation.
This study aimed to demonstrate that the effect of negative nasopharyngeal pressure (post-sniffing) on middle-ear pressures is greater in ears with attic retraction pockets than in normal ears.
Materials and methods
This study was reviewed by Vijaya ENT Care Super Speciality Otology Centre's Ethics Committee and received approval (protocol number 2019–17).
The study consisted of 154 selected patients with different grades of attic retraction pockets (46 patients with bilateral attic retraction pockets and 108 with unilateral attic retraction pockets) who presented to a tertiary referral otology centre during the period from August 2015 through July 2018. Only patients who agreed to participate were included in this study. Excluded were patients whose ears showed pathology involving both the pars tensa and flaccida, middle-ear effusion, or tympanic membrane perforation, or who had undergone prior ear surgery.
The following grading system was used to classify attic retraction pockets.Reference Vijayendra, Mahajan, Vijayendra and Ramdass1 Grade I: the pars flaccida is dimpled; it is retracted towards the neck of the malleus but not adherent to it. Grades IIa and IIb: the fundus of the attic retraction pocket is completely seen on otoscopic examination without the need for an endoscope. The pars flaccida is adherent (grade IIa) to the neck of the malleus or (grade IIb) to the head of the malleus, causing the neck to be completely visible and the head of the malleus to be partly visible, with mild erosion of scutum. Grades IIIa, IIIb and IIIc: the fundus of the attic retraction pocket is out of view on mere otoscopic examination but becomes completely visible on endoscopic examination, with moderate scutal erosion. Grade IIIa is without ossicular erosion, and the pars flaccida drapes over the neck and head of the malleus and onto the incus. Grade IIIb shows ossicular erosion. Grade IIIc has cholesteatoma in the attic retraction pocket. Grades IVa, IVb and IVc: the attic retraction pocket is completely or only partly visible on endoscopic examination alone, with severe scutal erosion. Grade IVa shows the pars flaccida draped over the neck and head of the malleus, and the entire incus, without erosion. Grade IVb shows an attic retraction pocket with ossicular erosion in any combination. Grade IVc has cholesteatoma in the attic retraction pocket. Grade V: extensive attic retraction pocket with complete outer attic (scutal) erosion and ossicular necrosis, with lateral semicircular canal erosion, with or without tegmen plate erosion.
Patients underwent otoendoscopy, nasal endoscopy, pure tone audiometry and impedance audiometry. Patients were instructed how to sniff and perform the Valsalva manoeuvre (Figure 1). Impedance audiometry pressure measurements were obtained in the normal resting state, and after sniffing, swallowing and the Valsalva manoeuvre. All middle-ear pressure changes were measured in decapascals. Changes in middle-ear pressure were recorded from the baseline resting pressure for each ear, in decapascals. Sniffing creates negative nasopharyngeal pressure, while swallowing and the Valsalva manoeuvre create positive pressure.

Fig. 1. Impedance audiometry with (a) forced negative nasopharyngeal pressure (sniffing) and (b) forced positive nasopharyngeal pressure (Valsalva manoeuvre).
Results
Table 1 outlines the changes in decapascals with sniffing, swallowing and the Valsalva manoeuvre for normal ears without attic retraction pockets and ears stratified by grade of attic retraction pocket. Sniffing created negative nasopharyngeal pressure, while swallowing and Valsalva created positive nasopharyngeal pressure. Baseline measurements of resting middle-ear pressure varied for each ear, and the subsequent drop in pressure with sniffing was recorded in negative decapascals. All tympanograms were type A for baseline, sniffing, swallowing and the Valsalva manoeuvre, in normal ears and in ears with attic retraction pockets.
Table 1. Pressure changes, middle-ear collapse and pressure normalisation with sniffing, swallowing and Valsalva manoeuvre in control ears and ears with attic retraction pockets

*Mean difference between middle-ear pressure in attic retraction pockets and baseline = −31 daPa (standard deviation = 6.37 daPa). Comparison of control versus attic retraction pocket ears: †p < 0.0001; ‡p < 0.08; **p < 0.16. ARP = attic retraction pocket; NA = not applicable
Sniffing
The 108 normal ears showed much less diminution of pressure in decapascals than the 200 ears with attic retraction pockets when the negative nasopharyngeal pressure of sniffing was applied. The 108 normal ears showed an average of −5 daPa change in middle-ear pressure with sniffing. In contrast, 170 of 200 ears with attic retraction pockets (85 per cent) showed a drop in decapascals with sniffing. The drop in pressure across all 200 ears with attic retraction pockets varied from −24 daPa to −45 daPa according to the grade of attic retraction pocket. Average variation in middle-ear pressure after sniffing was: −26 daPa in grade I attic retraction pockets, −26 daPa in grade IIa, −28 daPa in grade IIb, −37 daPa in grade IIIa, −24 daPa in grade IIIb, −30 daPa in grade IIIc, −27 daPa in grade IVa, −34 daPa in grade IVb, −31 daPa in grade IVc and −45 daPa in grade V. The mean difference between middle-ear pressure in attic retraction pockets and baseline was −31 daPa, with a standard deviation (SD) of 6.37 daPa. A student's paired t-test found that the difference in pressure measurement changes after sniffing in the normal ears compared with the ears with attic retraction pockets was statistically significant (p < 0.0001).
Swallowing restored 61 per cent of the attic retraction pocket ears that had collapsed on sniffing to baseline, and the Valsalva manoeuvre returned 88 per cent of those ears to baseline. Therefore, the Valsalva manoeuvre was more effective than swallowing in returning negative pressure in the attic retraction pocket ears to baseline.
Swallowing and Valsalva manoeuvre
Positive nasopharyngeal pressure changes were consistently greater after the Valsalva manoeuvre than after swallowing in both normal and attic retraction pocket ears. In contrast to the negative nasopharyngeal pressure changes post-sniffing, however, positive nasopharyngeal pressure changes from baseline in the middle ear after swallowing and after the Valsalva manoeuvre were similar in the normal and the attic retraction pocket ears: p-values for the differences between positive pressure changes in normal and attic retraction pocket ears were p < 0.08 after swallowing and p < 0.08 after the Valsalva manoeuvre (Table 1).
A comparison of the differences between normal ears and attic retraction pocket ears in pressure changes post-sniffing versus post-swallowing revealed significantly different effects (p < 0.0001). Similarly, the differences between normal ears and attic retraction pocket ears in pressure changes after sniffing compared with after the Valsalva manoeuvre showed significantly different effects (p < 0.0001).
Discussion
This study revealed that nasopharyngeal pressure changes are co-incident with the same pressure changes in the middle ear in those with attic retraction pockets. Our study does not definitively prove that the unmitigated transmission of nasopharyngeal pressure change to the attic is the actual cause of the attic retraction pocket. However, the data in this study show that all control ears (with normal-appearing pars flaccida) showed only slight reductions in middle-ear pressure with sniffing: pressure in the normal ears after sniffing decreased on average by only −5 daPa. In contrast, the ears with attic retraction pockets showed a significant reduction after sniffing (mean = −31 daPa, SD = 6.37), indicating that these middle ears were experiencing the nasopharyngeal pressure changes.
Positive nasopharyngeal pressure changes after swallowing and after the Valsalva manoeuvre did not cause significantly different changes in the middle-ear pressure in normal versus attic retraction pocket ears. In other words, positive nasopharyngeal pressure caused similar increases in middle-ear pressures in normal and attic retraction pocket ears, while negative nasopharyngeal pressure caused a much greater drop in pressure in the attic retraction pocket ears. We conclude from these measurements that the negative nasopharyngeal pressure post-sniffing is transmitted via a more open Eustachian tube in the attic retraction pocket ears, but that the Eustachian tube is more closed in the normal ears, and transmission of negative nasopharyngeal pressure to the middle ear is mitigated. Positive nasopharyngeal pressure after swallowing and after the Valsalva manoeuvre, on the other hand, is transmitted via the Eustachian tube to normal and attic retraction pocket ears equally. An easy way to conceptualise this is as follows: the Eustachian tube is chronically open in ears that form attic retraction pockets, while the Eustachian tube is basically closed in normal ears, opening when positive nasopharyngeal pressure pops it open.
LaPlace's law demonstrates a possible reason for the preferential evacuation, collapse and retraction of the attic space, and is further explored here for the reader's consideration. Intuitively, it seems that when two disparate volumes are in communication, the larger volume would empty into the smaller volume; however, the exact opposite is the case. LaPlace's law states that the pressure within a sphere varies with the inverse of the radius.Reference Thiriet and Thiriet5 Therefore, air within the smaller epitympanic region will evacuate more readily than air in the larger middle-ear space.6 This principle explains why smaller volumes evacuate first; the surfactant's role in alveoli, for example, is to counteract LaPlace's law and keep the small air spaces open.Reference Thiriet and Thiriet5
For this discussion, the corresponding author replicated LaPlace's law as it applies to two unequal air-containing spaces: the attic (epitympanic space) and the middle ear (mesotympanum). Figure 2 demonstrates that when the Eustachian tube is opened, air from the smaller volume evacuates preferentially. Figure 3 demonstrates that while forced positive nasopharyngeal pressure (post-Valsalva manoeuvre) inflates both attic and middle ear, forced negative nasopharyngeal pressure (post-sniffing) preferentially evacuates the smaller attic space. Similarly, LaPlace's law explains the tendency for the attic to form an attic retraction pocket.
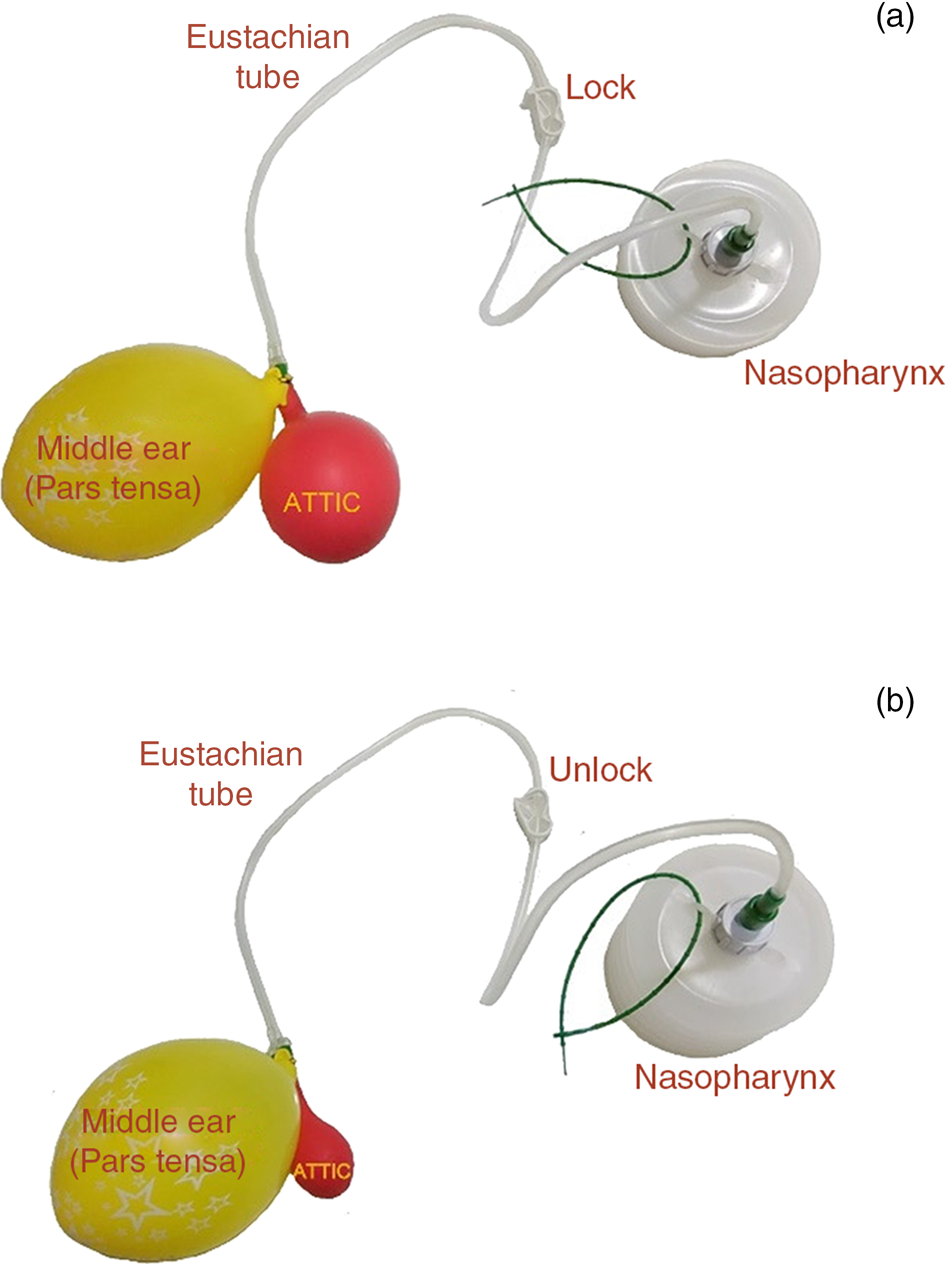
Fig. 2. Model of middle ear (yellow balloon), attic area (red balloon), Eustachian tube (tubing) and nasopharynx (canister). (a) Both the middle ear and attic are aerated, and the Eustachian tube is closed. (b) When the Eustachian tube is open, the smaller attic area evacuates preferentially into the canister.

Fig. 3. Nasopharyngeal pressure changes in the model of the middle ear (yellow balloon), attic area (red balloon), Eustachian tube (tubing) and nasopharynx (canister). (a) Valsalva manoeuvre (forced positive pressure up the Eustachian tube) re-inflates both the middle-ear space and the attic. (b) Sniffing (forced negative pressure in the nasopharynx and the Eustachian tube) causes evacuation of the smaller air space (attic) first, (c) then the larger air space (middle ear) second.
To restate this application of LaPlace's law: the epitympanum, middle-ear space, and Eustachian tube are a continuous system. Because the Eustachian tube in ears that form attic retraction pockets is too open and transmits the negative nasopharyngeal pressure too readily, the epitympanum preferentially empties into the nasopharynx. Just as the balloon illustration demonstrates, the two ear air spaces are under higher pressure relative to the release route into the nasopharynx when the patients sniff. Sniffing causes negative nasopharyngeal pressure, and that negative nasopharyngeal pressure too readily pulls on the middle-ear and epitympanic spaces, causing them to evacuate into the nasopharynx, the smaller air space first.
Earlier literature supports this observation of LaPlace's law in action. Sade et al.Reference Sade, Fuchs and Luntz7 noted that the pars flaccida tends to retract when the attic is continuous with a contracted mastoid air space and tends not to retract when it is continuous with a larger mastoid air space. They attributed this to ‘buffering’, but the phenomenon is consistent with LaPlace's law – the smaller air cell spaces are under more pressure to evacuate. Marchioni et al.Reference Marchioni, Mattioli, Alicandri-Ciufelli and Presutti8 noted that the attic (epitympanic region) and the middle-ear space (mesotympanum) are separate spaces, connected by a variable isthmus, and that the smaller attic spaces tended to retract more than the larger attic spaces. Others note that in ears with attic retraction pockets, sniffing causes a more marked drop in middle-ear pressure compared with normal ears.Reference Kobayashi, Yaginuma, Takahashi and Takasaka2,Reference Falk and Magnuson3,Reference Magnuson9 They also state that non-closure of the Eustachian tube,Reference Kobayashi, Yaginuma, Takahashi and Takasaka2,Reference Falk and Magnuson3 which is a failure of the Eustachian tube to protect the middle ear and attic from the extreme pressure changes of the nasopharynx, is responsible for the attic retraction pocket formation.
Hence, this study demonstrates that, in ears with attic retraction pockets, the negative nasopharyngeal pressure is communicated more than in normal ears. It has long been known that the thinner pars flaccida has only sparse fibres in its lamina propria and lacks a stabilising annulus.Reference Mansour, Mansour, Magnan, Haidar, Nicolas and Louryan4 We have observed the diminution in pressure in these ears, and speculate that the pars flaccida composition and the smaller attic radius both contribute to the attic retraction pocket formation.
• The normal tympanic membranes of 108 patients were compared to the contralateral 108 tympanic membranes with attic retraction pockets and 92 bilateral attic retraction pockets
• Pressure changes with sniffing (negative nasopharyngeal pressure), and swallowing and Valsalva manoeuvre (positive pressure), were measured
• All 308 ears showed transmission of positive nasopharyngeal pressure changes to the tympanic membrane
• However, negative nasopharyngeal pressure changes were transmitted only to the 200 attic retraction pocket ears, not to the 108 normal ears
• In attic retraction pocket ears, Eustachian tube was unable to mitigate nasopharyngeal negative pressure changes and protect the middle ear from these negative pressures
The strengths of this study are that the measurements and data are straightforward. Furthermore, LaPlace's law is quite clear and seems to support our model of attic retraction pocket formation well. Another strength is that our controls are paired with affected ears in the same patients. Therefore, we are not comparing the physiology of affected individuals with the physiology of unaffected controls: The control ears are in the same individuals as the affected ears. A weakness of this study is that we do not know why some ears cannot mitigate the nasopharyngeal pressure changes and some can.
Conclusion
We believe that this study, with a level of evidence of 5, demonstrates that attic retraction pockets are associated with greater collapse of middle-ear volume when negative nasopharyngeal pressure is created, while normal ears do not show the same degree of negative nasopharyngeal pressure changes.
Competing interests
None declared




