


Introduction
Granular myringitis is a disorder characterised by focal or diffuse replacement of the dermis of the tympanic membrane and adjacent canal wall by granulation tissue, while the underlying lamina propria remains intact.Reference Schuknecht1, Reference Levinson2 The relative lack of attention given to granular myringitis in the literature can cause this condition to be overlooked in the care of patients with chronic ear complaints. Such inattention can delay the initiation of appropriate treatment, and can further complicate management.Reference Blevins and Karmody3
Symptoms are usually mild, and mainly comprise discharge and a sense of aural fullness.Reference Wolf, Primov-Fever, Barshack, Polack-Charcon and Kronenberg4 Granular myringitis may appear as a discrete, shallow, ulcerated lesion, or as a polypoidal mass arising from the tympanic membrane. It is assumed that, left untreated for a long period, recovery involves scarring of the tympanic membrane and external auditory canal wall, and can lead to stenosis of the ear canal, thickening of the tympanic membrane and hearing impairment.Reference Khalifa, El-Fouly, Basssiouny and Kamel5–Reference Stoney, Kwok and Hawke7
The condition responds readily to topical antibiotic steroid drops. Occasionally, cauterisation with 50 per cent trichloroacetic acid may be needed for exuberant granulation tissue. Any fungal overgrowth must be treated first. However, the condition tends to recur, or to give rise to further, irreversible pathological changes.
If the response to topical treatment is inadequate, an oral quinolone antibiotic is prescribed. If the condition recurs, the prognosis is discussed with the patient and the option of surgery suggested. Surgical excision of the entire granular area and underlay grafting has been recommended in refractory cases.Reference El-Seifi and Fouad8
Five-fluorouracil (5-FU) is one of the oldest chemotherapy drugs, and has been in use for decades. It is active against many cancers. Five-fluorouracil is a clear, colourless liquid which is given intravenously. It is also available as a cream for treatment of skin cancer. Five-fluorouracil has become accepted because of its efficacy, economical price and relative absence of side effects.Reference Smith9
Five-fluorouracil is a DNA synthesis inhibiting agent. It remains stable in solution at room temperature for several months, and precipitates under refrigeration.Reference Miller10, Reference Heidelberger, Ghobar and Baker11
Five-fluorouracil induced inhibition of DNA synthesis and lack of normal RNA result in unbalanced cell growth and subsequent cell death. Rapidly multiplying tumour cells have a higher DNA and RNA turnover than normal cells, and therefore accumulate larger amounts of lethal fluorouracil.Reference Goette12
In the field of ENT, applications for 5-FU include the (very well known) anticancer role of parenteral 5-FU in head and neck tumours, and its topical use in skin lesions such as solar keratoses and (in situ) squamous cell carcinoma.Reference Perrett, McGregor, Warwick, Karran, Leigh and Proby13 Five-fluorouracil has also been trialled in the treatment of recurrent respiratory papillomatosis.Reference Smith, Healy, Vaughan and Strong14
In otology, topical 5-FU has been trialled in the treatment of external auditory canal cholesteatoma, attic cholesteatoma with aerated mastoid, and localised recurrent cholesteatoma.Reference Takahashi, Funabiki, Hasebe, Fukuda-Yamamoto, Kaieda and Iwanaga15 The safety of topical use of 5-FU on auditory and vestibular structures has recently been evaluated in a guinea pig model.Reference Smith9
Materials and methods
Between November 2004 and September 2007, 60 patients with granular myringitis were enrolled in this preliminary controlled, double-blinded study performed at Cairo University Hospital.
The study was approved by the local ethics committee, and informed consent was obtained from all patients.
Granular myringitis was defined as the presence of granulation over an intact tympanic membrane, with normal audiography and a type A tympanogram.
We excluded from the study patients with hypersensitivity to 5-FU, marked external auditory canal stenosis, multiple exostoses or eustachian tube dysfunction.
Patient diagnosis was based on history-taking, otoscopic examination, and endoscopic examination of the external auditory canal and tympanic membrane.
Patients were divided randomly (using sealed, opaque, sequentially numbered envelopes) into two groups: group A, the study group (30 patients), and group B, the control group (30 patients). Group A patients received three successive local applications of 5-FU 5 per cent cream, with two-week intervals between treatments, while group B patients received local petroleum jelly cream packing at the same intervals.
In group A, after cleaning as much debris as possible from the external auditory canal and tympanic membrane surface, a 5-cm piece of gauze impregnated with 3 cm of 5 per cent 5-FU topical cream was applied on the outer side of the drum transmeatally, using an operating microscope. Group B patients received petroleum jelly cream applied in the same way. After two days, the pack was removed and the external auditory canal cleaned.
Follow-up visits were scheduled every two weeks for the first three months, and then every three months for two years. At the end of the first three months' follow up, patients answered a questionnaire about their response to treatment, with particular emphasis on the quantity of discharge. In addition, at the end of the first three months, thorough cleaning of the external auditory canal was followed by endoscopic examination of the canal and tympanic membrane using a 0°, 2.7 mm Storz rigid endoscope (Storz, Tuttlingen, Germany).
In this study, both the patient and the doctor (who documented the symptoms and endoscopic findings) were unaware of the treatment used.
A four-point scale was used to grade the degree of response to treatment, with zero denoting complete resolution, one moderate improvement, two no improvement and three deterioration. This scale was used to grade both the granulations (assessed by endoscopic examination) and the amount of discharge (reported by the patient).
After two years, patients were recalled for evaluation of any persistent disease, which was defined as granulations or discharge of the same degree of severity as before treatment, or worse.
The chi-square test was used to compare categorical data. A probability (p) value of less than 0.05 was considered statistically significant, and a value of 0.01 or less was considered highly statistically significant. All statistical calculations were performed using the Microsoft Excel version 7 (Microsoft Corporation; New York, New York, USA) and the Statistical Package for the Social Sciences (SPSS Inc; Chicago, Illinois, USA) version 15 for Microsoft Windows computer software programs.
Results
This study included 60 patients, 36 men (60 per cent) and 24 women (40 per cent), with ages ranging from 18 to 53 years (mean, 35.5). The right ear was affected in 33 patients (55 per cent), the left in 22 (36.7 per cent) and both in five (8.3 per cent). According to the classification of Wolf et al. (Table I), this study included nine patients with grade I granular myringitis (15 per cent), 28 with grade II (46.7 per cent), 18 with grade III (30 per cent) and five with grade IV (8.3 per cent).Reference Wolf, Primov-Fever, Barshack, Polack-Charcon and Kronenberg4 Five patients were lost to follow up (two from group A and three from group B) and so were excluded from the study.
Table I Classification of granular myringitisReference Wolf, Primov-Fever, Barshack, Polack-Charcon and Kronenberg4
TM = tympanic membrane; EAC = external auditory canal
Group A included 19 men (63 per cent) and 11 women (37 per cent), with ages ranging from 18 to 50 years (mean, 33.5). The right ear was affected in 16 patients (53 per cent), the left in 11 (37 per cent) and both in three (10 per cent). Three patients had a mild local allergic reaction to the first treatment application, in the form of itching, redness and mild canal oedema; this disappeared on subsequent applications. Two patients were excluded after being lost to follow up. After three months, 17 patients (60.7 per cent) reported no discharge, six (21.4 per cent) less discharge, three (10.7 per cent) no change (compared with before treatment), and two (7.1 per cent) more discharge (Figure 1). Endoscopic evaluation after three months revealed no granulation tissue in 15 patients (53.6 per cent), less granulation tissue in 10 (35.7 per cent), no change in two (7.1 per cent) and more granulation tissue in one (3.6 per cent). After two years, persistent disease was seen in three patients (10.7 per cent). Data and outcomes for group A patients are shown in Table II.
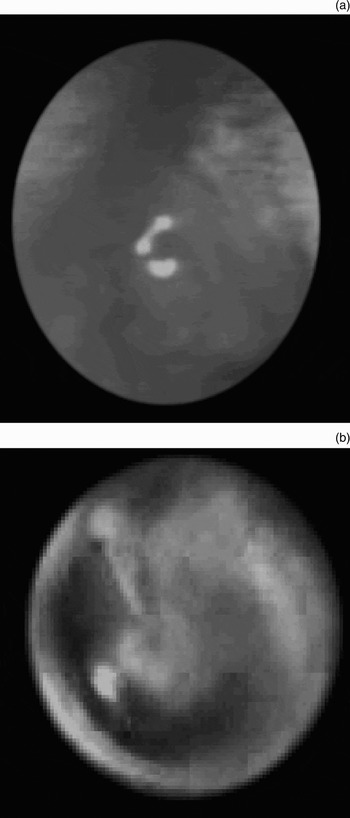
Fig. 1 Otoscopic views of granular myringitis (a) before treatment and (b) after treatment
Table II Lesion data and outcomes: group A patients

*See text for details. †Amount of 5-fluorouracil (5-FU) 5 per cent cream. ‡Two years post-treatment; 0 = complete resolution, 1 = moderate improvement, 2 = no improvement, 3 = deterioration. Pt no = patient number; y = years; M = male; F = female; R = right; L = left; − = absent; + = present
Group B included 17 men (56.7 per cent) and 13 women (43.3 per cent), with ages ranging from 23 to 53 years (mean, 37.5). The right ear was affected in 17 patients (56.7 per cent), the left in 12 (40 per cent) and both in one (3.3 per cent). Three patients were excluded after being lost to follow up. After three months, two patients (7.4 per cent) reported no discharge, four (14.8 per cent) less discharge, 16 (59.3 per cent) no change (compared with before treatment) and five (18.5 per cent) more discharge. Endoscopic evaluation after three months revealed no granulation tissue in two patients (7.4 per cent), less granulation tissue in five (18.5 per cent), no change in 17 (63 per cent) and more granulation tissue in three (11.1 per cent). After two years, persistent disease was seen in 20 patients (74 per cent). Data and outcomes for group B patients are shown in Table III.
Table III Lesion data and outcomes: group B patients

*See text for details. †Amount of 5-fluorouracil (5-FU) 5 per cent cream. ‡Two years post-treatment; 0 = complete resolution, 1 = moderate improvement, 2 = no improvement, 3 = deterioration. Pt no = patient number; y = years; F = female; M = male; L = left; R = right; −= absent; += present
Comparing the study and control groups, there were no statistically significant differences as regards sex distribution (p = 0.701), age distribution (p = 0.137), side of complaint (p = 0.73) or disease grading (p = 0.922). However, there were highly statistically significant differences as regards three-month post-treatment outcomes (i.e. reported discharge and observed granulation tissue) and persistent disease at 24 months (p < 0.001). The difference in outcomes between the two groups is shown in Figures 2–4 and Table IV.

Fig. 2 Comparison of discharge quantity in the two groups. 3 = Deterioration; 2 = no improvement; 1 = moderate improvement; 0 = complete resolution.

Fig. 3 Comparison of granulation outcomes in the two groups. 3 = Deterioration; 2 = no improvement; 1 = moderate improvement; 0 = complete resolution.

Fig. 4 Comparison of persistent disease at two years in the two groups.
Table IV Comparison of patients' demographic characteristics and treatment outcomes

*Study group, n=30; †placebo group, n = 30. ‡Evaluated endoscopically. Y = years; mod = moderate
Discussion
Granular myringitis is usually described as an obscure, poorly understood, uncommon disease.Reference El-Seifi and Fouad8 Stoney et al. considered the condition to represent an infection of the tympanic membrane, with possible involvement of the external auditory canal.Reference Stoney, Kwok and Hawke7 Granular myringitis is defined as de-epithelialisation of the tympanic membrane, with formation of granulation tissue without involvement of the middle-ear cleft.Reference Stoney, Kwok and Hawke7
Several aetiological factors have been suggested: local trauma, poor hygiene and impacted cerumen.Reference Wolf, Primov-Fever, Barshack, Polack-Charcon and Kronenberg4 Any dermatological condition that can lead to desquamation and disruption of squamous epithelium can cause the disease, and it is commonly found in cases of psoriatic and eczematous skin disease. Precipitating factors include infection (e.g. otitis media and externa) and allergic reactions. Heat, moisture and pyrexia are known to have an adverse effect on external auditory canal skin which is maximal in the deepest, least aerated part of the canal.Reference El-Seifi and Fouad8
The main treatment for granular myringitis is topical antibiotic steroid drops, local cleaning and superficial curettage. Cauterisation with 50 per cent trichloroacetic acid has been trialled for exuberant granulation tissue. Jung et al. found that 15 patients treated with dilute vinegar solution all recovered from their original otorrhoea within three weeks, whereas two-thirds of 15 patients treated with antibiotic ear drops recovered within three weeks.Reference Jung, Cho, Yoo, Lim and Chea16 (The disadvantages of dilute vinegar therapy were canal irritation, pain and dizziness.)
Studies indicate that approximately 6 per cent of topically applied 5-FU is systemically absorbed, an amount generally considered too small to produce systemic side effects. There is no evidence that 5-FU is ototoxic, and the biopharmacological bases for its action do not suggest any such ototoxicity. The cochlear and vestibular end-organ is not a rapidly multiplying tissue, and patients who have received large amounts of 5-FU systemically have not demonstrated any evidence of either vestibular or cochlear damage. The most frequently encountered local reactions to the topical use of 5-FU on the skin are pain, hyperpigmentation and a burning sensation at the site of application. Other local reactions of 5-FU on the skin include dermatitis, scarring, pain, suppuration, scaling and swelling.Reference Smith9 The major complication of topical 5-FU is chronic ulceration.Reference Takahashi, Funabiki, Hasebe, Fukuda-Yamamoto, Kaieda and Iwanaga15
Smith et al. observed that the use of 5-FU was associated with inhibition of recurrent respiratory papillomatosis regrowth in six of eight patients.Reference Smith, Healy, Vaughan and Strong14
In the field of otology, Smith in 1985 assessed the use of topical 5-FU in the management of cholesteatoma and unwanted mucus-secreting cells. The results of this retrospective study suggested a very impressive efficacy of topical 5-FU in the management of cholesteatoma and, to a lesser degree, in the control of mucus-hypersecreting cells at locations in the middle ear and mastoid.Reference Smith9 Iwanaga et al. reported that the application of 5-FU ointment to the external ear in guinea pigs appeared safe, but that its application in the middle ear may pose some risk of ototoxicity.Reference Iwanaga, Tanaka, Tsukasaki, Terakado, Kaieda and Takasaki17 Yamamoto-Fukuda et al. suggested that the effect of 5-FU on cholesteatoma appeared to be mediated, at least in part, by down-regulation of keratinocyte growth factor in stromal cells and reduction of the proliferative activity of epithelial cells.Reference Yamamoto-Fukada, Terakado, Hishikawa, Koji and Takahashi18
Takahashi et al. applied topical 5-FU cream two to five times, with intervals of two weeks, in patients with cholesteatoma.Reference Takahashi, Funabiki, Hasebe, Fukuda-Yamamoto, Kaieda and Iwanaga15 This was comparable to our topical use of 5-FU cream three times with two-week intervals in granular myringitis patients. In Takahashi and colleagues' study, 59 per cent of cases showed a good effect, 29 per cent a fair effect and 12 per cent a poor effect. Five-fluorouracil was particularly effective in external auditory canal cholesteatomas, attic cholesteatomas with an aerated mastoid, and recurrent-type cholesteatomas.Reference Takahashi, Funabiki, Hasebe, Fukuda-Yamamoto, Kaieda and Iwanaga15 Based on previous, favourable results for the use of 5-FU in treating cholesteatoma, and lack of obvious side effects, we are the first authors in the literature to evaluate 5-FU in the management of cases of granular myringitis, using a blinded, controlled study design.
We found a highly statistically significant difference between our study and control groups for the outcomes measured (i.e. reported discharge, observed granulation tissue and persistent disease at 24 months) (p < 0.001). Thus, topical use of 5-FU in cases of granular myringitis appears to be effective. No major complications were detected, apart from mild allergic reactions.
Future studies are recommended, incorporating: (1) larger patient numbers, (2) longer follow-up periods, (3) other topical agents in the control group (other than petroleum jelly cream, as it could be argued that this may exacerbate myringitis by preventing drying); and (4) comparison of 5-FU with standard granular myringitis treatments (i.e. topical antibiotics plus steroid eardrops, or dressings or acetic acid).
• Granular myringitis is a poorly understood disease causing considerable discomfort and concern in affected individuals
• This study investigated the efficacy and safety of topical 5-fluorouracil (5-FU) in cases of granular myringitis
• There was a statistically significant positive effect of topical 5-FU in granular myringitis
• Further study is needed to confirm this finding
Such studies are needed in order to confirm the results of this preliminary work, to assess the optimal number of local 5-FU applications and best inter-treatment interval, and to further investigate local reactions and systemic side effects.
Conclusion
Topical application of 5-FU is a new method for the treatment of granular myringitis. It is a simple, well tolerated, clinic-based procedure, and in this study it proved effective and safe, with no serious local reactions or complications.








