


Introduction
Airway management is a vital component of care in the in-patient setting. The National Emergency Airway Registry project analysed over 17 500 emergency department intubations, of which 97 per cent of attempts performed by physicians higher than intern level were successfully completed by the primary physician.Reference Brown, Bair and Pallin1 Despite this high success rate, 1.2–3.8 per cent of adult patients experience difficult intubation, whilst 0.05–0.1 per cent experience difficult mask ventilation.Reference Cattano, Panicucci, Paolicchi, Forfori, Giunta and Hagberg2
Risk factors for a difficult intubation include obesity (body mass index of more than 30 kg/m2),Reference Rose and Cohen3 male gender,Reference Rose and Cohen3 age of over 40 yearsReference Moon, Baek, Kim, Koo, Kim and Woo4 and obstructive sleep apnoea (apnoea–hypopnea index of more than 10).Reference Siyam and Benhamou5,Reference Hiremath, Hillman, James, Noffsinger, Platt and Singer6 Additionally, physical aspects of the airway, such as thyromental distance, cervical flexibility, poor dentition and Mallampati score, have been associated with an increased risk of difficult intubation.Reference Rose and Cohen3–Reference Shiga, Wajima, Inoue and Sakamoto8
An awake tracheostomy may be one of the best options to secure the airway for a patient whose trachea cannot be intubated.Reference Rose and Cohen3 The majority of awake tracheostomies are well-tolerated. However, sedatives and analgesics must often be avoided. This may lead to patient movement during the procedure, anxiety or significant pain. Additionally, previous neck trauma or cancer may increase the risks and complications of an awake tracheostomy. These adverse outcomes may be avoided in properly selected patients who are co-operative enough to tolerate awake intubation with an anterior commissure laryngoscope and a bougie.
This study examined the outcomes of patients who underwent rigid anterior commissure laryngoscopic intubation using a bougie, performed by an otolaryngology surgeon. The paper describes the ideal patients who may benefit from this procedure.
Materials and methods
A retrospective study was conducted of a series of intubations performed by a surgeon in the operating theatre at a tertiary medical centre. Adult patients were identified through a search of the medical centre billing database using the Current Procedural Terminology (‘CPT’) code 31500 – ‘intubation by surgeon’. This search identified 49 encounters from 2005 to 2015 in which an otolaryngology surgeon performed intubation using an anterior commissure laryngoscope (Figure 1) in the operating theatre. Patients who were managed only by other methods, such as fibre-optic intubation, were not included in the analysis.

Fig. 1. Anterior commissure laryngoscope used for surgeon-performed intubations.
Age, sex, a history of previous difficult intubation and the reason for the current difficult intubation were reviewed. The number of failed intubation attempts and method of failed intubation were recorded. It was determined whether the patient was awake or paralysed during the attempt, and if the difficult airway was anticipated prior to the initial attempt. Institutional review board approval was obtained through the University of Oklahoma Health Sciences Center; informed consent was not required.
In those patients for whom intubation is expected to be difficult, we follow a protocol at our institution to select candidates for awake anterior commissure laryngoscope intubation. The majority of surgeons performing planned anterior commissure laryngoscope intubations in awake patients follow this protocol, described below.
The ideal candidate for surgeon-performed intubation needs to be able to tolerate a pre-operative transnasal flexible fibre-optic laryngoscopy in the pre-operative holding area, performed to properly visualise the airway anatomy and develop a plan of approach prior to proceeding to the operating theatre. In patients with tenuous airways, the flexible nasolaryngoscopy is performed without local anaesthetic; this avoids the loss of sensation in the glottic airway, an increase in airway flow resistance and the potential for increasing respiratory distress.Reference Beydon, Lorino and Verra9–Reference Sofferman, Johnson and Spencer11 The patient must be able to calmly maintain a supine position for the short duration of the anterior commissure laryngoscope intubation. Finally, in co-ordination with anaesthetists, the patient must be able to demonstrate sufficient pulmonary function to maintain oxygen saturation during the intubation. Ideally, respiratory depression with sedatives and anxiolytics should be avoided to prevent respiratory arrest. Our preference is an infusion of dexmedetomidine, which provides adequate sedation whilst maintaining spontaneous ventilation.
The ideal surgeon-performed intubation in awake patients begins with direct laryngoscopy using the Hollinger or similar anterior commissure laryngoscope (Figure 2). Laryngeal suction can be conducted through the scope to remove secretions. Once the laryngoscope enters the supraglottis, providing a view of the vocal folds, a bougie is passed through the laryngoscope and past the glottis into the trachea under direct vision (Figure 3). Whilst maintaining control of the bougie, the laryngoscope is removed and an appropriately sized endotracheal tube is placed over the bougie by the surgeon (Figure 4). The endotracheal tube is then threaded along the bougie to the correct depth. The bougie is then removed, the cuff is inflated and ventilation is confirmed.

Fig. 2. Visualisation of glottis via direct laryngoscopy performed with an anterior commissure laryngoscope.

Fig. 3. Standard bougie passed through scope and through the glottis.
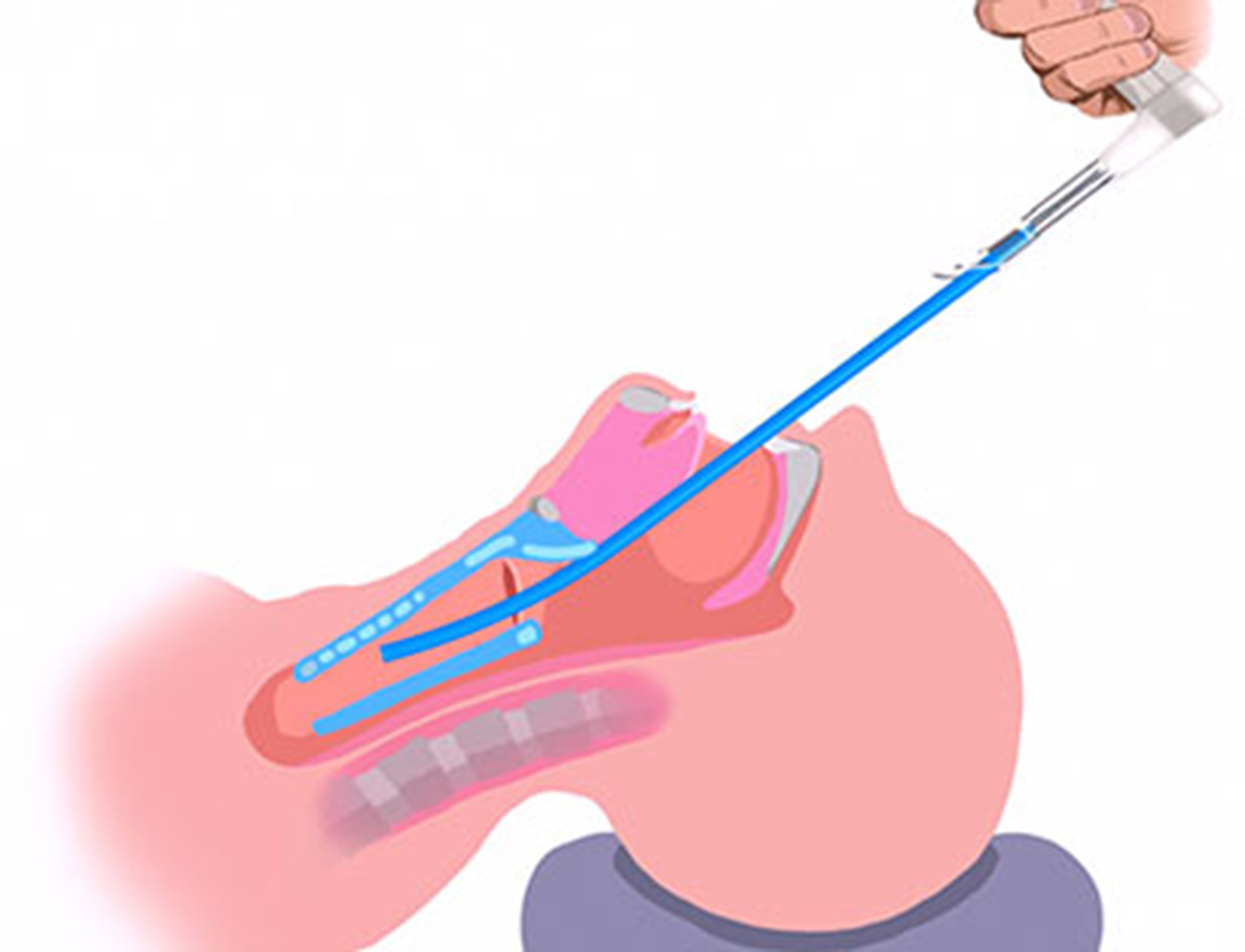
Fig. 4. Removal of laryngoscope, whilst maintaining control of the bougie's position.
Results
Demographics and history of difficult airway
Forty-nine patients (31 males) were included in this study. The average patient age (± standard deviation) was 58.8 ± 4.63 years. Ten patients (20 per cent) had a history of previous difficult intubation during a previous hospitalisation.
Success rates and outcomes
Forty-seven of the 49 patients (96 per cent) were successfully intubated by the surgeon using an anterior commissure laryngoscope. Forty-six patients were intubated on the first attempt, with only one patient requiring a second attempt to secure the airway with an anterior commissure laryngoscope.
Of the two patients for whom anterior commissure laryngoscope intubation attempts were unsuccessful, one subsequently underwent fibre-optic intubation by an anaesthesiologist, whilst the second patient underwent a successful emergent surgeon-performed tracheostomy but ultimately died from cardiac arrest in the operating theatre.
Use of paralysis versus awake intubation
Forty-one per cent of the patients were awake for intubation. Dexmedetomidine was the only medication given by the anaesthesiologist in the majority of these cases and topical anaesthetic was avoided. Twenty-nine patients (59 per cent) were documented as having received a paralytic agent at the time of intubation. Of the two unsuccessful anterior commissure laryngoscope attempts, one patient was awake for the intubation.
Causes of difficult intubation
The two most common causes of difficult airway were an obstructive mass (22 out of 49 patients, 43 per cent) and trismus (11 out of 49 patients, 22 per cent). Other causes included: acute infection, neck immobilisation, obesity, laryngeal oedema and post-operative bleeding (Table 1). The reasons for difficult intubation in the two failed cases were: a lingual thyroid causing airway obstruction (benign mass), and obesity in an intensive care patient with respiratory failure.
Table 1. Documented reasons for difficult airway

Previous attempts
Forty-seven patients were successfully intubated by the surgeon using an anterior commissure laryngoscope. Twenty-nine of these 47 patients (62 per cent) were first encountered by the surgeon following a previous failed intubation attempted by an anaesthesiologist using a different method, most often utilising a Macintosh or Miller blade. Previous failed intubation attempts by anaesthesiologists with other methods had occurred once in 20 patients, twice in 2 patients and at least three times in 7 patients.
The remaining 38 per cent of patients successfully intubated with the anterior commissure laryngoscope (18 out of 47) were intubated by the surgeon on the first attempt. Many of these patients were undergoing a head and neck procedure and, for this reason, a surgeon was available and ready to intubate in the operating theatre. Other patients were identified by the anaesthesiology pre-operative investigation in light of a prior history of difficult intubation. This gave advance notice for the surgeon to be available for pre-operative planning and intubation in the operating theatre.
Expected versus unexpected difficult airway
The majority of patients in this study (36 of 49 patients, 73 per cent) were expected by the anaesthesia team to be difficult to intubate. This included 18 patients who were intubated within one attempt by the surgeon using the anterior commissure laryngoscope. Seventeen patients required attempts by anaesthesiology with other methods prior to successful surgeon-performed intubation with the anterior commissure laryngoscope, including the patient who was unsuccessfully intubated using the anterior commissure laryngoscope method and who subsequently died of respiratory arrest.
Thirteen of 49 patients were unexpectedly difficult to intubate. Fortunately, nine of the unexpected cases occurred with the surgeon present, who was immediately available to assist with the anterior commissure laryngoscope intubation. In the other four unexpected cases, the surgeon was not originally involved with the intubation but was called emergently by the anaesthesiologist for assistance.
Discussion
Surgeon-performed intubation using a bougie and anterior commissure laryngoscope has been described previously. However, the rationale and mechanics of this method have not been clearly communicated to those who manage the airway in other specialties.
The anterior commissure laryngoscope is a rigid metal enclosed tube with a fibre-optic light source at the distal end, which gives the surgeon the ability to view structures through the scope. The anterior commissure laryngoscope was designed for inspection of the larynx and hypopharynx, and to perform procedures such as biopsy and foreign body removal, for example. The lumen of the tube is relatively narrow, allowing the user to negotiate patient anatomy to reach the glottic larynx, unlike a Macintosh or Miller blade. Additionally, the enclosed tube avoids the prolapse of tissue from the tongue or lateral wall of the pharynx that can occlude the user's view. The surgeon uses the scope to pass a bougie through to the trachea under direct vision. This method is similar to the Seldinger technique for vascular access or percutaneous tracheostomy. With an anterior commissure laryngoscope, either of the surgeon's hands can be used, and either side of the mouth can be accessed, depending on patient anatomy.
Figures 5 and 6 show the side and proximal profiles of a Macintosh blade, respectively. The anterior commissure laryngoscope's profile is low and short, which allows this laryngoscope to be passed on either side of the anterior maxillary teeth to view the glottic larynx. This is important in those patients with limited mouth opening or a prominent overbite.

Fig. 5. Side profiles of the Macintosh blade and anterior commissure laryngoscope. The anterior commissure laryngoscope, shown above the Macintosh blade, has a ‘lower’ or ‘slimmer’ straight profile.

Fig. 6. Proximal profiles of the Macintosh blade and anterior commissure laryngoscope. The ‘high’ profile of the Macintosh blade shown on the left, which has to utilise the oral axis to gain entry towards the larynx, can make intubation difficult and potentially damage teeth. The arrow demonstrates the difference in height between the two scopes.
Figure 7 demonstrates the axes in traditional intubation.Reference Mace12 The Macintosh laryngoscope blade uses the ‘oral axis’, but requires the curvature of the blade to retract the tongue with the blade tip within the vallecula. The Miller blade takes advantage of the pharyngeal axis, as the blade is straight and the tip is used to elevate the epiglottis. With both Macintosh and Miller blades, the retraction is anterior and superior, to avoid contact with the upper teeth, and both blades are open, which can allow prolapsed tissue into the field of view.
Fig. 7. Axes of traditional intubation using the (a) Macintosh and (b) Miller blades. Reproduced with permission.Reference Mace12
The anterior commissure laryngoscope is used differently. This blade almost always utilises the laryngeal axis or pharyngeal axis to view the glottic larynx directly. Unlike the Macintosh or Miller blades, the surgeon ‘intentionally’ places pressure from the scope onto the upper teeth which are protected with a tooth guard. The mechanics are different, with only a gentle tilting of the distal end of the anterior commissure laryngoscope superiorly, using the upper teeth as a fulcrum. No excessive force is required. Dental injuries are rare, and otolaryngologists routinely apply considerable force onto the upper teeth when performing procedures within the larynx and pharynx. This different approach runs counter to what our anaesthesia colleagues are taught as they struggle to avoid hitting the teeth.
It is our opinion that the method of intubation with laryngoscopes that have a ‘high’ profile in difficult airway patients may contribute to more dental injuries than intentionally resting a scope with a ‘lower’ profile against the teeth using minimal force and a tooth guard. Davies and Balachandran described the anterior commissure laryngoscope method of intubation as the ‘paraglossal or retromolar technique’, wherein:
‘…the anterior commissure laryngoscope is passed from the right corner of the mouth, displacing the tongue to the left and advanced towards the larynx (under direct view) between the tongue and tonsil. The neck is flexed and the head extended to bring the axes of the mouth, pharynx and larynx into alignment. Displacement of the tongue to the left removes the tongue from the line of view. This prevents the tongue from limiting anterior movements of the blade, which may be the cause of difficult intubation when a Macintosh blade is used. This technique is not new and has been described before but is forgotten amongst most anesthesiologists’.Reference Davies and Balachandran13
A difficult airway requires proper evaluation and planning to optimise success. As described by Rose and Cohen, the patients most likely to have a difficult intubation are obese, diabetic males aged 40–59 years.Reference Rose and Cohen3 A more recent study has shown that patients of advanced age (over 60 years) are more likely to score higher on risk factor indices such as Mallampati and Arne scores, as are those with physical indicators such as a decreased thyromental length, decreased inter-incisor gap (i.e. a patient with trismus) (Figure 8) and increased cervical joint rigidity.Reference Moon, Baek, Kim, Koo, Kim and Woo4 In addition, it is important to obtain a thorough medical and surgical history, with special considerations to previous intubations, oropharyngeal or laryngeal masses (Figure 9), or any other co-morbidities that may affect airway access. Eighty-seven per cent of patients in this series did not have a history of difficult intubation during previous hospitalisations. Seventy-three per cent undergoing intubation were expected to have airway access difficulties, which reinforces the importance of careful pre-operative evaluation.

Fig. 8. Patient with trismus, showing status following chemoradiation for oropharyngeal cancer.

Fig. 9. Axial, contrast-enhanced computed tomography scan of the neck, showing a right-sided neck abscess.
Use of a bougie with a traditional Macintosh blade has previously been described as a first-line technique for establishing a difficult or lost airway.Reference Sofferman, Johnson and Spencer11 The use of a bougie in these previous descriptions is especially relevant only if an adequate view of the glottis can be obtained with the traditional Macintosh or Miller blade. As our study shows, this is not always possible. The difficult intubations in this series are a result of inadequate glottic views using traditional laryngoscopy techniques, resulting from the anatomical and pathological difficulties in this cohort. The difficult view was overcome with the rigid anterior commissure laryngoscope, and only then was a bougie helpful in securing the airway. The authors advise against blind intubation or blind bougie insertion in difficult airway patients, as this may cause unnecessary trauma to surrounding structures, and may further compromise the airway, leading to an emergent airway situation.
In this study, those intubations performed in paralysed (under general anaesthesia) or awake patients highlight the usefulness of the anterior commissure laryngoscope and bougie. First, we discuss the difficult airway patient who has already been paralysed for intubation in the operating theatre, and who presents an urgent airway situation for the anaesthesiologist and surgeon. When the anaesthesia team plans to perform intubation in a patient with a potentially difficult airway, our recommendation is that a rigid anterior commissure laryngoscope, light source and bougie be available in the room in case the initial attempts by the anaesthesiology team are unsuccessful. Despite our best attempts at early identification of difficult airways, there will often be emergent, unplanned situations in the operating theatre that require surgeon-performed intubation. It has become common at our institution, and often a recommendation at other institutions, for anaesthesiologists to have an anterior commissure laryngoscope set and light source available in the operating theatre for emergency intubations; all otolaryngology residents at our institution are trained to use this method when indicated.
Second is the subset of 20 patients who were intubated whilst awake using an anterior commissure laryngoscope and bougie, with no paralytic and no local anaesthetic. The avoidance of paralytics, sedatives and local topical anaesthetic allows a patient to maintain their own airway tone, and reduces the potential for obstruction and loss of airway prior to intubation. Our method was well-tolerated, and all but one of these patients avoided an awake tracheostomy.
This series suggests that surgeon-performed intubation in awake patients is a reliable option for most patients anticipated to have a difficult airway. Ideally, those who are expected to have a difficult intubation by traditional methods can be managed on the first attempt with well-planned surgeon-performed intubation using an anterior commissure laryngoscope and bougie. Communication is key to success. The anaesthesiology and surgery teams should be accustomed to discussing the expectations and intubation plan prior to an emergent situation.
Anticipation of a difficult airway does not necessarily ensure successful intubation, as evidenced by two unsuccessful intubations, in addition to the cases that required multiple attempts. Equipment for an awake tracheostomy must always be available if intubation fails, and will continue to be essential in patients who are unable to tolerate direct laryngoscopic intubation when awake.
• Outcomes and complications of direct laryngoscopy and bougie-assisted, surgeon-performed intubations in adults over a 10-year period were investigated
• Direct rigid laryngoscopic intubation by 5 surgeons was successful in 47 of the 49 cases (96 per cent)
• Over half the patients had previously had one or more failed intubations with other methods and other providers
• Only one patient who underwent surgeon-performed direct laryngoscopy required urgent tracheostomy because of intubation failure
• Surgeon-performed laryngoscopic intubation using a bougie should be considered in select adults with unfavourable anatomy or pathological obstruction
• This is a reliable and safe procedure for those who need an urgent, secure airway, as it may preclude the need for an urgent tracheostomy in an awake patient
Limitations of this study include the possibility that not all patients who underwent anterior commissure laryngoscope intubation at our institution were identified. If the Current Procedural Terminology code for ‘intubation by surgeon’ was not included in the billing record, that case would not be captured. Intubations performed by surgeons using the anterior commissure laryngoscope and bougie that were conducted outside of the operating theatre were not included in this review. However, in our experience, the technique has been useful on numerous occasions in the intensive care unit and emergency department, and this may warrant further study.
Another limitation was the inability to accurately record methods of attempted intubation by the anaesthesia team prior to intubation by the surgeon using the anterior commissure laryngoscope technique. In most cases, the intubation attempts were made using a video laryngoscope and/or flexible nasolaryngoscope in the awake patients, but the patients were unable to tolerate these procedures, or the anaesthesiology team were unable to pass the scope or endotracheal tube into the airway. Interestingly, we found that patients easily tolerated the rigid anterior commissure laryngoscope when awake, most likely because of its slim profile and the timeliness of intubation.
This retrospective series, with a level of evidence of IV, demonstrated a 96 per cent success rate of surgeon-performed intubation using an anterior commissure laryngoscope and bougie in patients with a difficult airway, including those who were unable to have their airways secured by the anaesthesiology team using standard techniques. It is also a well-tolerated initial approach for patients who need to remain awake whilst their airway is secured. The high success rate demonstrates that this method warrants further consideration regarding its utility in securing a difficult airway.
Competing interests
None declared










