Introduction
Voice impairment evaluation and quantification are necessary in clinical practice to effectively determine the severity of dysphonia and to evaluate any possible treatment. The voice assessment can be done by objective or subjective voice analysis methods.
Objective voice examination is done by acoustic analysis,Reference Werth, Voigt, Döllinger, Eysholdt and Lohscheller1 whereas subjective voice quality assessment can be done both from the clinician's or patient's point of view. Physicians and other professionals use the auditory perceptual evaluation of voice method to evaluate patient voice quality.Reference Ziwei, Zheng and Pin2 Several scales are broadly used with different criteria, including the grade, roughness, breathiness, asthenia and strain (‘GRBAS’) scale, as proposed by the Japanese Society for Logopedics and PhoniatricsReference Hirano, Arnold, Winckel and Wyke3 and recommended by the European Laryngological Society,Reference Dejonckere, Bradley, Clemente, Cornut, Crevier-Buchman and Friedrich4 and the consensus auditory perceptual evaluation of voice (‘CAPE-V’), as proposed by the American Speech–Language–Hearing Association.Reference Kempster, Gerratt, Verdolini Abbott, Barkmeier-Kraemer and Hillman5 The national outcomes measurement system (‘NOMS’) as developed by the American Speech–Language–Hearing Association to measure therapeutic outcomes in understanding the effectiveness of speech therapy is a less-used clinician scale.Reference Childs, Bielinski, Toles, Hamilton, Deane and Mau6,7
On the other hand, patient voice self-assessment can be done using other scales to evaluate the impact of voice disorders on the patient's physiological, social and psychological functions. One of the most used scales is the voice handicap index (‘VHI’) scale described by Jacobson et al Reference Jacobson, Johnson, Grywalski, Silbergleit, Jacobson and Benninger8 or its shortened and validated version with 10 items, the voice handicap index-10.Reference Rosen, Lee, Osborne, Zullo and Murry9 The 10-item voice-related quality of life scale (‘V-RQOL’) is also a valid index of quality of life impairments as a result of voice disorders.Reference Hogikyan and Sethuraman10 Another similar scale with three items added to voice-related quality of life was developed in a personal communication at the University of Iowa and was named later as Iowa patient's voice index (‘IPVI’).Reference Karnell, Melton, Childes, Coleman, Dailey and Hoffman11
Clinician and patient measures related to quality-of-life topics do not always agree. In this study, we checked the relationship between both clinician and patient measurements in muscular tension dysphonia, a functional voice disorder. Muscular tension dysphonia has been chosen because these type of voice disorders are defined by absence of organic lesions of the vocal folds, and voice analysis is the main way to evaluate severity and response to treatment. They are usually produced by vocal misuse or abuse and a psychological background is often assumed.Reference Koufman and Blalock12,Reference Van Houtte, Van Lierde and Claeys13
Muscular tension dysphonia is the most frequent functional voice disorderReference Cobeta Marco, Nuñez Batalla, Fernández González, Cobeta Marco, Nuñez Batalla and Fernández González14 and was characterised by Morrison et al. in 1983.Reference Morrison, Rammage, Belisle, Pullan and Nichol15 In this pathological condition, the extensive tension of the extra and intra-laryngeal musculature, caused by a diverse number of aetiological factors, leads to a disturbed voice.Reference Van Houtte, Van Lierde and Claeys13
Although there is no internationally accepted classification system of muscular tension dysphonias, the following different patterns are the most frequently used: type 1 muscular tension dysphonia, laryngeal isometric contraction with posterior open chink because of a hypertonic state of the posterior cricoarytenoid muscle; type 2 muscular tension dysphonia, approximation to the midline of the false vocal folds; type 3 muscular tension dysphonia, anteroposterior contraction that results in a reduced space between the epiglottis and the arytenoids prominences; and type 4 muscular tension dysphonia, complete supraglottic closure of the larynx with extreme anteroposterior contraction and approximation of the arytenoids to the petiole.Reference Koufman and Blalock12,Reference Van Houtte, Van Lierde and Claeys13 Even though this classification is not a severity scale, type 4 muscular tension dysphonia could be considered the most serious version of the disease because of a combination of type 2 and type 3 muscular tension dysphonia.
The objective of this study was to determine any possible relationship between the results of the grade, roughness, breathiness, asthenia and strain scale and voice handicap index-10 scale to see the degree of consensus between patients and physicians in the severity evaluation of a voice dysfunction. As far as we know, this is the first paper that considers this relationship by comparing all items of each scale relating to any kind of functional dysphonia, for which physicians do not observe any lesion in physical examination.
We tried finding any influence of muscular tension dysphonia type on variation in grade, roughness, breathiness, asthenia and strain and voice handicap index-10 scale in order to assess which type of muscular tension dysphonia can affect voice more severely. We hypothesised that different patterns of larynx muscular contraction could impact subjective voice analysis.
Materials and methods
We performed a retrospective study including all patients diagnosed with muscular tension dysphonia over six years in the laryngology department of a tertiary care hospital. The study received approval from the ethics committee of La Paz University Hospital, Madrid, Spain (reference number: PI-2445).
A complete clinical history was taken. Patients filled in the voice handicap index-10 questionnaire as a subjective measurement of the severity of the dysphonia from their point of view before entering the examination room. In order to measure the severity of dysphonia from the clinician's point of view, we used the grade, roughness, breathiness, asthenia and strain scale, which was taken before performing any other exploration. A senior physician was in charge of determining these scores without knowing the previous voice handicap index-10 results.
Thereafter, acoustic analysis and physical exploration including stroboscopy was performed. After the endoscopic and stroboscopic examination, patients were categorised with muscular tension dysphonia types 1 to 4 by following the previously mentioned classification. All laryngoscopy videos were reviewed by a second physician to obtain the inter-rater reliability for the grade, roughness, breathiness, asthenia and strain scale and muscular tension dysphonia type. This reliability was measured with Cohen's kappa coefficient in both cases. Muscular tension dysphonia Cohen's kappa coefficient was 0.9, and the grade, roughness, breathiness, asthenia and strain scale coefficient was 0.81, which suggests an almost perfect agreement between the observers.
Different factors that could influence voice handicap index-10 or grade, roughness, breathiness, asthenia and strain scale parameters were studied. Gender influence was determined with student t-test and Wilcoxon test to compare the results. A univariate linear model (linear regression) was used to detect any age influence, and analysis of variance (ANOVA) was used to evaluate the influence of different smoking habits. The significance level chosen for all measures was α = 0.05.
The possible relationship between the subjective clinician measurements (grade, roughness, breathiness, asthenia and strain scale) and the subjective patient scores (voice handicap index-10) in each patient was assessed by Spearman correlation. We excluded those patients for whom either the voice handicap index-10 and grade, roughness, breathiness, asthenia and strain scale were not completed. We checked correlation between grade, roughness, breathiness, asthenia, and strain scale and voice handicap index-10 global values and between each grade, roughness, breathiness, asthenia, and strain scale parameter and voice handicap index-10 to see which item could give us more information about a patient's perception of his or her own voice.
Finally, we tested the relationship of different muscular tension dysphonia patterns with the grade, roughness, breathiness, asthenia and strain scale and voice handicap index-10 values. This was estimated using one-way ANOVA test. As sample size was limited, we did a non-parametric variance test (Kruskal–Wallis) too.
Results
Seventy-five patients were diagnosed with muscular tension dysphonia. The mean age was 50 years, and 60 per cent of patients were women. Up to 59 per cent of patients presented with vocal abuse in their social or work life. Dysphonia was the main complaint and was present in all patients. Half of the patients (49 per cent) reported vocal fatigue, and only 15 per cent presented odynophonia.
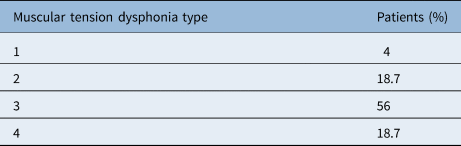
The percentage of patients presenting with each type of muscular tension dysphonia is given in Table 1. It was impossible to determine information about muscular tension dysphonia type in two patients (2.7 per cent).
Table 1. Percentage of patients with each muscular tension dysphonia type

We did not observe any statistically significant influence of gender in voice handicap index-10 index or in the grade, roughness, breathiness, asthenia and strain scale. Also, no statistically significant influence of age was found for voice handicap index-10 (age explains 0.4 per cent of variability of voice handicap index-10) or in the grade, roughness, breathiness, asthenia and strain scale (age explains 2 per cent of variability of the grade, roughness, breathiness, asthenia and strain scale). Likewise, we did not find smoking habits (smokers, non-smokers and ex-smokers) to have any impact on these subjective indexes.
Additionally, we also looked for any influence of muscular tension dysphonia type in voice handicap index-10 and the grade, roughness, breathiness, asthenia and strain scale. We found no statistical difference in voice handicap index-10 score between muscular tension dysphonia types (ANOVA: p = 0.23; Kruskal–Wallis: p = 0.22) even though it seemed there was an inclination to have lower values in muscular tension dysphonia type 1 and scores that were higher when muscular tension dysphonia type 4 was present (Figure 1).

Fig. 1. Box-plot showing VHI-10 values depending on muscular tension dysphonia type. VHI-10 values showed no statistical difference between muscular tension dysphonia types, even though muscular tension dysphonia type 1 tends to have better values and muscular tension dysphonia type 4 worse values. VHI = voice handicap index; MTD = muscular tension dysphonia
On the other hand, the ANOVA test showed that muscular tension dysphonia type 4 had a statistically different result in comparison with the grade, roughness, breathiness, asthenia and strain scale indexes (ANOVA: p = 0.006; Kruskal Wallis: p = 0.01). When a mean comparison with corrected p-value was done, the obtained grade, roughness, breathiness, asthenia and strain scale scores were statistically different when compared with muscular tension dysphonia type 1 (p = 0.04) and muscular tension dysphonia type 3 (p = 0.01) with muscular tension dysphonia type 4 (Figure 2).

Fig. 2. Box-plot of GRBAS scale scores depending on muscular tension dysphonia type. Muscular tension dysphonia type 4 presents worse GRBAS scale scores than the rest of muscular tension dysphonia types. GRBAS = grade, roughness, breathiness, asthenia, strain; MTD = muscular tension dysphonia
Regression analysis was performed to demonstrate any possible correlation between the grade, roughness, breathiness, asthenia and strain scale and voice handicap index-10. Only patients with both indexes registered were included (n = 63). A Spearman rank correlation coefficient (rho) of 0.56 (95 per cent confidence interval (CI), 0.36–0.71) was obtained (Figure 3).

Fig. 3. Regression analysis between GRBAS and VHI-10 scores. Rho = 0.56 (95 per cent confidence interval, 0.36–0.71). We can observe a moderate correlation but a wide dispersion. VHI = voice handicap index; GRBAS = grade, roughness, breathiness, asthenia, strain
Correlation between voice handicap index-10 and each item of the grade, roughness, breathiness, asthenia and strain scale was checked. Results are shown in Table 2.
Table 2. Correlation between VHI-10 and each item of GRBAS scale

VHI = voice handicap index; GRBAS = grade, roughness, breathiness, asthenia, strain
Discussion
It is known that subjective perceptual evaluation is sometimes more important than voice analysis or physical examination to determine severity of voice pathology.Reference Ziwei, Zheng and Pin2 Hence, perceptual evaluation of voice scales from the clinician's point of view are used in most laryngology departments, and they are extremely important for very dysphonic voices where acoustic analysis cannot be performed. On the other hand, self-assessment measures provide inestimable information of vocal function from the patient's point of view. Owing to these measures, patients are able to show the clinician how a particular pathology affects their personal or professional life depending on their vocal demands.
We might think that a clinician's auditory-perceptual evaluation of severity of dysphonia and a patient's perception of handicap is highly correlated, meaning that when the clinician perceives greater dysphonia the patient would report greater handicap. However, contrary to that supposition, a correlation of 0.56 (95 per cent CI, 0.36–0.71) was found between perception of the listener (grade, roughness, breathiness, asthenia and strain scale) and the speaker (voice handicap index-10). Thus, we obtained just a moderate correlation with wide dispersion.
There are several studies that correlate subjective voice assessment from the clinician's and the patient's point of view, even though none of them specifically studied patients suffering from muscular tension dysphonia where there would be no observable lesions in vocal folds. In these studies, we can find comparison between different subjective perceptual scales other than voice handicap index-10 and the grade, roughness, breathiness, asthenia and strain scale (Table 3).
Table 3. Spearman correlations between patient- and clinician-based scales in different studies

*Correlation is negative because high voice-related quality of life ratings represent less severely dysphonic voices, and high CAPE-V severity and high grade (GRBAS) ratings represent more severely dysphonic voices. The same situation occurs with the NOMS system and the personal scale used in Ugulino et al.;Reference Ugulino, Oliveira and Behlau20 †Pearson correlation was obtained in the study by Childs et al. instead of Spearman correlation; ‡lineal regression was obtained in study by Behrman et al. instead of Spearman correlation. VHI = voice handicap index; GRBAS = grade, roughness, asthenia, breathiness, strain; V-RQOL = voice-related quality of life; CAPE-V = consensus auditory perceptual evaluation of voice; S-E = social-emotional; IPVI = Iowa patient's voice index; NOMS = national outcomes measurement system
Most of these studies show weak-to-moderate correlation between both measurements.Reference Childs, Bielinski, Toles, Hamilton, Deane and Mau6,Reference Karnell, Melton, Childes, Coleman, Dailey and Hoffman11,Reference Murry, Medrado, Hogikyan and Aviv16–Reference Bauer, Aleric and Jancic18 However, when the study was focused only on the social-emotional domains of the voice-related quality of life or emotional component of the voice handicap index, the strength of the agreement went down with the correlation being weak or non-existent.Reference Ziwei, Zheng and Pin2,Reference Karnell, Melton, Childes, Coleman, Dailey and Hoffman11,Reference Murry, Medrado, Hogikyan and Aviv16
The study by Child et al. found moderate correlation as well, but this correlation increased when the clinician determined moderate-to-severe levels of vocal dysfunction; that is, when the function perceived by the clinician worsened, the correlation appeared stronger. Additionally, they found the strongest correlation in patients suffering from functional dysphonia (r = −0.64).Reference Childs, Bielinski, Toles, Hamilton, Deane and Mau6
There were other studies that tried to find factors that may be predictive of patient perception of severity of dysphonia, but they did not find any correlation.Reference Behrman, Sulica and He19,Reference Ugulino, Oliveira and Behlau20
There are only a few studies that performed a comparison between the grade, roughness, breathiness, asthenia and strain scale and voice handicap index per se, even though they are widely used scales in clinical practice. However, none of the studies studied patients suffering from any kind of functional dysphonia. In two recent studies (similar to our study) carried out in patients after thyroid surgery and in patients affected by multiple sclerosis, weak-to-moderate correlation between the two assessment measures was found.Reference Papadakis, Asimakopoulou, Proimos, Perogamvrakis, Papoutsaki and Chimona17,Reference Bauer, Aleric and Jancic18
Alternatively, some studies found a strong correlation when comparing different items of the grade, roughness, breathiness, asthenia and strain scale with different components of the voice handicap index. The study by Ziwei et al. showed a strong correlation between grade and just functional and physiological items of the voice handicap index.Reference Ziwei, Zheng and Pin2 Señaris González et al. found the strongest correlation between breathiness and strain parameters with the voice handicap index, mainly with functional and emotional subscales of the voice handicap index.Reference Señaris González, Núñez Batalla, Corte Santos and Suárez Nieto21 In our study, when we compared each grade, roughness, breathiness, asthenia and strain scale item with voice handicap index-10, we found a low to moderate correlation (r = 0.33–0.46). With this data, we cannot find any grade, roughness, breathiness, asthenia and strain scale item that correlates with a given voice handicap index-10 item.
We have chosen muscular tension dysphonia for our study as this disease produces symptomatic patients without organic lesions and, as a result, voice analysis is crucial to evaluate its severity and response to treatment. The study by Child et al. found the strongest correlation between the patient's and clinician's perspective of voice handicap in functional dysphonia. Child et al. believed that patients with muscular tension dysphonia were more concerned about their voices than other patients. Dysphonia was the patient's primary reason for seeking care; therefore, the patient may expect the clinician's assessment of dysfunction to be closer to their own point of view.Reference Childs, Bielinski, Toles, Hamilton, Deane and Mau6 In our study, despite patients suffering from a kind of functional dysphonia, correlation was not stronger than in the rest of the studies.
Finally, we tried to determine if there was any influence of muscular tension dysphonia type in voice assessments. Contrary to our hypothesis, we did not find influence of muscular tension dysphonia type in voice handicap index-10 assessments even though it seems that there was an inclination towards lower values in muscular tension dysphonia type 1 and higher values when muscular tension dysphonia type 4 was present. We believe that the greater the presence of contraction, the more the patient's perception of their own voice worsens; however, with our data we cannot determine that different patterns in muscle contraction differentially affect the quality of voice from patient's point of view.
• The relationship between grade, roughness, breathiness, asthenia and strain scale and voice handicap index-10 in muscular tension dysphonia was analysed
• A moderate correlation was found, which is similar to other studies
• Use of both measures is necessary to perform a complete assessment of dysphonia
• This study found no variation in voice handicap index-10 score with different muscular tension dysphonia types, but there was an inclination towards worse scores with muscular tension dysphonia type 4
• Grade, roughness, breathiness, asthenia and strain scale scores were worse in muscular tension dysphonia type 4
• This result could be explained by considering muscular tension dysphonia type 4 as the most severe form of this disease
On the contrary, we obtained statistically different higher grade, roughness, breathiness, asthenia and strain scale scores in patients suffering from muscular tension dysphonia type 4 when we compared them with muscular tension dysphonia type 1 and type 3 patients. Muscular tension dysphonia type 2 patients had the same tendency, but this difference was not statistically significant with our number of patients. The finding of worst grade, roughness, breathiness, asthenia and strain scale score results in muscular tension dysphonia type 4 could be explained, speculatively, by considering the fact that this muscular tension dysphonia type is the most severe form of disease as it produces a contraction in all planes.
This study has limitations as it was a retrospective study, which made it difficult to collect all the data properly. A greater number of patients would have been ideal to corroborate the moderate correlation between grade, roughness, breathiness, asthenia and strain scale and voice handicap index-10 and to demonstrate the hypothesis of considering muscular tension dysphonia type 4 as the most severe form of muscular tension dysphonia disease.
Conclusion
Our study, along with most of the literature, shows that there are differences among scaling systems that measure perception of voice pathology from the clinician's and the patient's point of view. Even though the two scales are moderately correlated, each one provides different information about the voice disorders and how patients perceive them. Both the scales have their own values and limitations. Clinician-based scales are needed in order to determine the characteristics and severity of voice problems because a clinician is likely to better separate the emotional aspect that affects perception of voice with other domains and decrease this bias. However, a similar degree of dysphonia can impact every patient differently depending on vocal demands and expectations. These factors will probably be reflected better on patient-based scales. Usually, the grade, roughness, breathiness, asthenia and strain scale is used to measure improvement after treatment, whereas voice handicap index-10 reflects the impact on patient quality of life and, therefore, is related to the need for an intervention to improve the dysphonia. Use of both the scales is necessary to perform a complete assessment of dysphonia, and they can be considered as complementary clinical tools.
Additionally, we found that type of muscular tension dysphonia merely affects severity of dysphonia. Patients themselves did not report different perceptions regarding each muscular tension dysphonia type. However, our results show that a clinician could differentiate muscular tension dysphonia type 4 from other muscular tension dysphonia types (1 and 3) following their grade, roughness, breathiness, asthenia and strain scale evaluation. These findings, though statistically significant, are difficult to integrate into a daily clinical practice. In future, studies with a higher number of patients would be necessary to support these findings.
Competing interests
None declared