Introduction
Cerebrospinal fluid (CSF) otorrhoea is a rare phenomenon that can potentially be life threatening. The presence of an abnormal communicating tract between sterile fluid from the subarachnoid space and middle-ear mucosa susceptible to various viral and bacterial infections can render a patient more at risk of developing meningitis.1 Cerebrospinal fluid otorrhoea can manifest either in childhood or later on in adult life.Reference Pachauri, Nagasonkar and Kirtane2 Reported cases from the latter category are usually secondary to a bony and dural defect in the tegmen tympani from iatrogenic injuries (e.g. otoneurological and neurosurgical interventions), trauma and infection.Reference Brown, Grundfast, Jabre, Megerian, O'Malley and Rosenberg3, Reference Savva, Taylor and Beatty4
Spontaneous CSF otorrhoea in children is largely congenital in origin.Reference Pachauri, Nagasonkar and Kirtane2 Gacek and colleagues have described four common locations for a congenital CSF fistula in the region of a normal labyrinth.Reference Gacek and Leipzig5, Reference Gacek, Gacek and Tart6 These are through the petromastoid canal, a wide cochlear aqueduct, the fallopian canal, and the tympanomeningeal fissure also known as Hyrtl's fissure.Reference Gacek and Leipzig5, Reference Gacek, Gacek and Tart6
Meningitis can often be the presenting condition for CSF otorrhoea, with quoted figures of 93 per cent in children and 36 per cent in adults.1 Other clinical features include clear otorrhoea or even rhinorrhea as CSF travels down the eustachian tube.1 Here, we describe the case of a young child who presented with spontaneous unilateral CSF otorrhoea as a result of a persistent Hyrtl's fissure. There is a paucity of published cases in the literature, and this is the first reported scenario where the CSF otorrhoea resolved spontaneously without the need for operative intervention.
Case report
A seven-year-old boy was seen in the ENT clinic because his external ears had altered shape. He had been troubled with right hearing loss since birth. Otherwise, his medical and drug history were unremarkable.
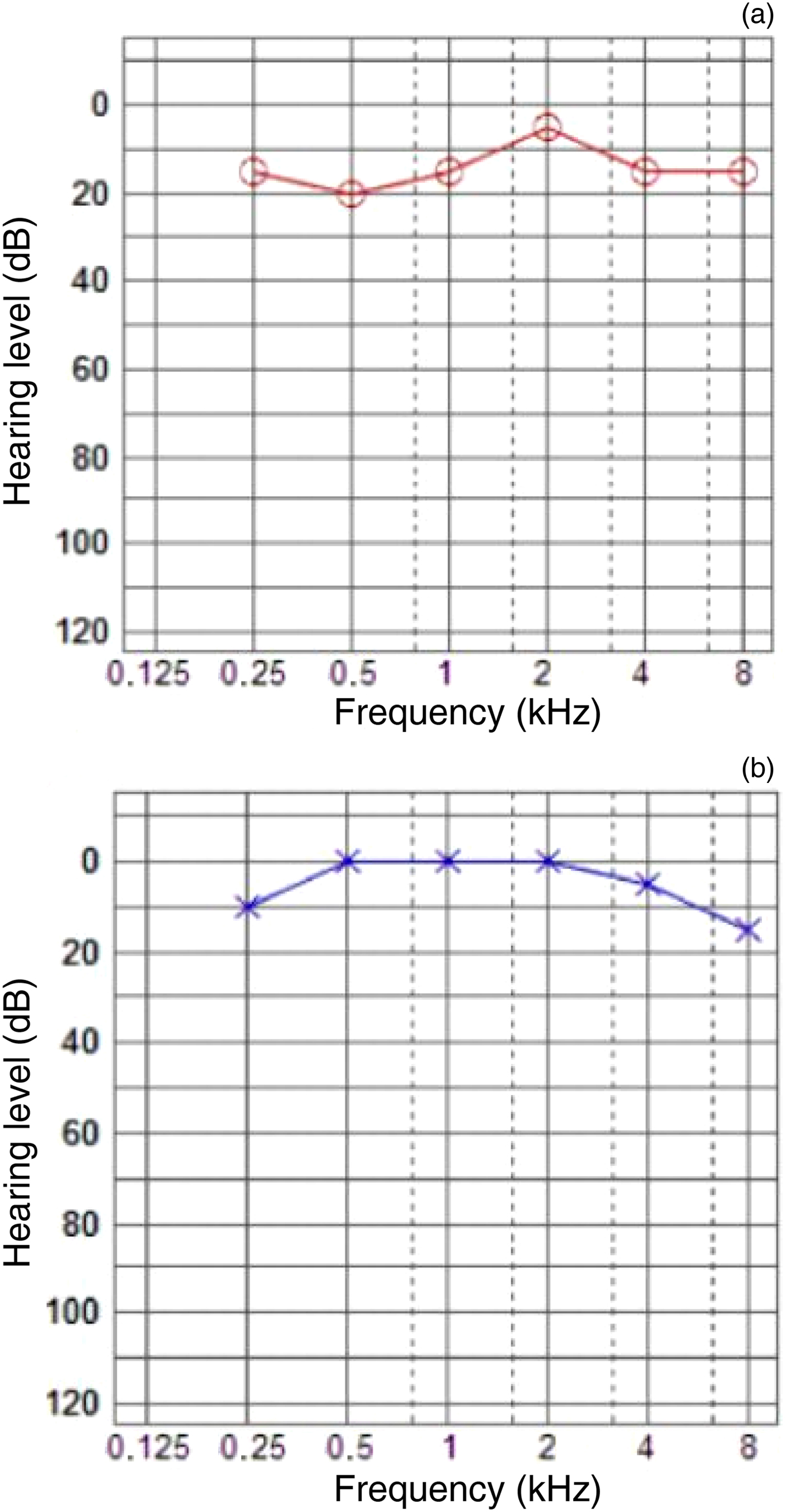
On otological examination, the child was noted to have bilaterally prominent ears, and a retracted eardrum and fluid-filled right middle ear. Left otoscopy findings were unremarkable. His tuning fork and hearing test results (Figure 1) confirmed right conductive hearing loss, and the diagnosis of unilateral otitis media with effusion was made. After discussing the options with his parents, the child was consented for bilateral pinnaplasty, examination under anaesthesia (EUA) and grommet insertion in the right ear.

Fig. 1 Pre-operative tympanogram of the (a) right ear (note the flat trace, suggesting ‘glue’ or fluid) and (b) left ear.
The procedure was carried out under general anaesthesia, and the pinnaplasty was performed uneventfully. During EUA of the right ear, myringotomy revealed a significant amount of clear fluid within the middle ear. A Shah's grommet was subsequently inserted. As the fluid continued to drain through the grommet, half an hour later, a sample was collected for Tau protein analysis. The grommet was then removed and the ear was packed with ribbon gauze impregnated in Betnovate®-C ointment.
Biochemical analysis of the fluid tested positive for beta-2 transferrin, confirming the presence of CSF within the right middle ear. The child then underwent a computed tomography (CT) scan of his temporal bones.
The CT images were reviewed at the regional skull base multidisciplinary team meeting in a tertiary neuro-otology unit. The panel concluded that the patient had a Hyrtl's fissure (Figure 2a and b), and suggested that the patient undergo surgical exploration to close the defect. However, when the patient was followed up in clinic at one month and four months later, his hearing was reported to have markedly improved. Otological examination and hearing tests (Figure 3) subsequently revealed a healed right tympanic membrane with no middle-ear fluid, and normal hearing. As such, it was decided that the child should be actively monitored every six months, with a view to undertake further CT scanning or magnetic resonance imaging (MRI).

Fig. 2 (a) Axial and (b) coronal computed tomography scans showing Hyrtl's fissure (red arrows).

Fig. 3 Pure tone (air conduction) audiogram of the (a) right ear and (b) left ear, four months post-myringotomy.
Discussion
A Hyrtl's fissure is a transient embryonic communication between an area inferior to the round window and the meninges of the posterior fossa.Reference Jegoux, Malard, Gayet-Delacroix, Bordure, Legent and Beauvillain de Montreuil7, Reference Rich, Graham and Phelps8 A thorough literature search using various search engines such as Google Scholar and PubMed revealed that this fissure is a rare phenomenon, with only a handful of reported cases.
One of the earliest reports was by Gacek and Leipzig, in 1979.Reference Gacek and Leipzig5 They described a case very similar to our own in that CSF otorrhoea was noted during myringotomy. In contrast to our scenario, the radiological images of the patient in their study showed that the leak was due to a meningocele that had herniated through the Hyrtl's fissure, requiring excision and packing of the middle ear and mastoid cavities.Reference Gacek and Leipzig5 This is similar to a case presented by Jegoux et al., who also reported a hernia that was repaired surgically.Reference Jegoux, Malard, Gayet-Delacroix, Bordure, Legent and Beauvillain de Montreuil7 In addition, Rich et al. wrote about a five-year-old child who presented with meningitis secondary to a Hyrtl's fissure, which required operative interventions.Reference Rich, Graham and Phelps8 More recently, Mouzali et al. reported a case of a failed cochlear implantation in an eight-year-old where the electrode array was misplaced in a Hyrtl's fissure.Reference Mouzali, Ouennoughi, Haraoubia, Zemirli and Triglia9 As this necessitated further repositioning, the authors suggested that pre-surgical imaging could be of paramount importance for patients undergoing cochlear implantation, to help identify congenital deformities. To date, there have been no published cases of a Hyrtl's fissure resolving spontaneously without surgical intervention.
Understanding the embryological development of these congenital fissures is vital in explaining their clinical features and guiding management. Spector et al. carried out multiple post-mortem examinations to outline the timescale from when the fissure is formed to the point where it helps become the lateral aspect of the cochlear aqueduct.Reference Spector, Lee, Carr, Davis, Schnettgoecke and Strauss10 Present from an early gestational period, the fissure begins to ossify by 16–18 weeks gestation and closes completely by the 24th week.Reference Spector, Lee, Carr, Davis, Schnettgoecke and Strauss10 In some individuals, incomplete ossification causes a persistent communication between the posterior cranial fossa and the round window, allowing CSF to drain into the middle ear.Reference Jegoux, Malard, Gayet-Delacroix, Bordure, Legent and Beauvillain de Montreuil7, Reference Rich, Graham and Phelps8 Because of its rarity, we were unable to find any data on its incidence and prevalence, but noted that most reported cases were unilateral.
The commonest presentations are conductive hearing loss, as seen in our case, and recurrent episodes of otitis media as a result of viral and bacterial colonisation of the persistent middle-ear fluid.1 Untreated, the disease can ascend and cause unexplained episodes of meningitis or other related neurological infections.Reference Rich, Graham and Phelps8 The appearance of clear otorrhoea is rare, especially in patients with intact tympanic membranes.1 However, on occasion, CSF can travel through the eustachian tube and result in persistent rhinorrhoea being the only symptom.1, Reference Jegoux, Malard, Gayet-Delacroix, Bordure, Legent and Beauvillain de Montreuil7
A high index of suspicion is vital in concluding a diagnosis.1 The presence of beta-2-transferrin, which is highly specific for CSF, aqueous humour and perilymph, should be determined in cases of unexplained clear otorrhoea or rhinorrhea.Reference Levenson, Desloge and Parisier11 Once this is established, imaging modalities such as contrast-enhanced CT or MRI scans are useful in delineating the defect and planning onward management.1
• Hyrtl's fissure is a transient embryonic communication between an area inferior to the round window and meninges of posterior fossa
• The fissure is present during the gestational period, with ossification from 16–18 weeks and closing completely by 24th week
• The incidence of a persistent Hyrtl's fissure is unknown because of its rarity
• The resultant cerebrospinal fluid (CSF) otorrhoea can cause conductive hearing loss and recurrent otitis media
• Untreated, this can lead to meningitis and ascending brain infections
• Surgical closure has been recommended, but active monitoring may suffice as CSF otorrhoea may resolve spontaneously
To date, numerous surgical methods of managing a Hyrtl's fissure have been described. Previous published work suggests that the fissure can be closed using either natural or synthetic materials.Reference Kutz, Husain, Isaacson and Roland12, Reference Kveton and Goravalingappa13 The commonest technique reported is to seal the fissure with muscle (e.g. temporalis muscle), bone wax or fibrin glue via a transmastoid approach.Reference Levenson, Desloge and Parisier11 A study by Kutz et al. showed that both alloplastic and autologous materials produced high rates of success, with no post-operative infections or complications.Reference Kutz, Husain, Isaacson and Roland12
As in our case, we feel that a conservative approach with active monitoring may suffice, as there is a possibility that the CSF otorrhoea will resolve spontaneously. We postulate this may be due to the transient nature of the fissure undergoing delayed closure.