


Introduction
The sphenopalatine foramen is a clinically important landmark in endoscopic sinus surgery; it transmits the sphenopalatine artery and is a site at which nasal pathology may arise. Anatomical variations of the sphenopalatine foramen and its surroundings can lead to difficulty in intra-operative visualisation, which may contribute to surgical failures. The identification of reliable bony landmarks for endoscopic approaches to the sphenopalatine foramen is clinically significant for diagnostic purposes and the planning of endoscopic procedures.Reference Padua and Voegels1 Endoscopic sinus surgery often routinely entails pre-operative imaging. The use of validated surgical landmarks identified on computed tomography (CT) imaging would allow surgeons to reliably identify the sphenopalatine foramen and anatomical variability pre-operatively in patients.
Currently, sphenopalatine foramen identification through bony landmarks is poorly documented in the literature, with most available data relying on anatomical dissection.Reference Prades, Asanau, Timoshenko, Faye and Martin2 The cadavers used in dissection studies can be subject to artifactual damage. Furthermore, the location of the sphenopalatine foramen can be harder to determine in cadavers with artifactual preservation of tissue.
This study aimed to establish, independently of age and gender, whether nasal bony landmarks on CT imaging could be reliably utilised to identify the sphenopalatine foramen. A study by Hadoura et al.Reference Hadoura, Douglas, McGarry and Young3 previously determined that osteological data correlated with radiological data, thus supporting the use of radiological imaging as an alternative for anatomical measurements.
Relevant anatomy
The sphenopalatine foramen is the main route of communication between the pterygopalatine fossa and the nasal cavity through which the neurovascular bundle enters. The sphenopalatine foramen lies on the lateral nasal wall and consists of a single or double orifice. It is related to the ethmoid crista of the palatine bone where it fixes to the tail of the middle turbinate.Reference Scanavine, Navarro, Megale and Anselmo-Lima4 The anterior border of the sphenopalatine foramen is characterised by a sharp bony crest, called the crista ethmoidalis, located at the narrow middle part of the hourglass-shaped foramen. However, the shape of the sphenopalatine foramen varies; it can be oval, square, triangular or piriform (pear-shaped). It has an average horizontal diameter of 5.1 mm (range, 4–7 mm) and an average vertical height of 6.2 mm (range, 4.5–7.5 mm).Reference Hadoura, Douglas, McGarry and Young3, Reference Scanavine, Navarro, Megale and Anselmo-Lima4 The opening of the sphenopalatine foramen is a vertically oriented oval shape, located at the end of the 4–7 mm canal which extends superiorly and inferiorly.Reference Chiu5 Anatomical variations on the lateral nasal wall include accessory foramens, arterial ramifications, variations within sphenopalatine foramen morphology and dimension, and relations to the middle turbinate.Reference Abuzayed, Tanriover, Gazioglu, Cetin and Akar6, Reference Cavallo, Messina, Gardner, Esposito, Kassam and Cappabianca7
Traditionally, the sphenopalatine foramen was described as an opening in the superior meatus located at the posterior end of the attachment of the middle turbinate on the lateral nasal wall. Some authors have reported the sphenopalatine foramen lying under the cover of the posterior part of the middle turbinate attachment, extending superiorly beyond the posterior horizontal portion of the superior turbinate lamella.Reference Lee, Kim, Kim, Son, Kim and Cho8, Reference Padgham and Vaughan-Jones9 In other studies, the sphenopalatine foramen has been reported to lie below the posterior end of the line of the middle turbinate attachment (middle meatus) and crista ethmoidalis, or at the transition of the middle and superior meatus.Reference Prades, Asanau, Timoshenko, Faye and Martin2, Reference Hadoura, Douglas, McGarry and Young3
The ethmoidal crest is a protrusion of bone formed as the perpendicular plate of palatine bone blends with the middle turbinate. It is an important anatomical landmark for the sphenopalatine foramen.Reference Rezende, Soares, Moraes, Oliveira and Nakanishi10 As the perpendicular plate of palatine bone runs obliquely and in a forwards direction, the plane of the sphenopalatine foramen opens forwards at an angle with the sagittal plane ranging from 0 to 30 degrees.Reference El-Guindy11
The sphenopalatine artery arises in the pterygopalatine fossa and courses medially in a large ‘S’ shape, eventually piercing the sphenopalatine foramen into the nasal cavity.Reference Midilli, Orhan, Saylam, Akyildiz, Gode and Karci12, Reference Solari, Magro, Cappabianca, Cavallo, Samii and Esposito13 The sphenopalatine artery is the terminal branch of the maxillary artery, which continues as a single stem artery and then divides into two branches: the posterior nasal artery and the nasopalatine artery.Reference Hadoura, Douglas, McGarry and Young3 The artery supplies 90 per cent of nasal mucosa, with the posterior septal artery supplying the septum and the posterolateral nasal artery supplying the middle and inferior turbinates and fontanelle.Reference Prades, Asanau, Timoshenko, Faye and Martin2 Additional collateral branches to the superior and/or middle turbinates can arise from the stem of the main branches or directly from the sphenopalatine foramen.Reference Prades, Asanau, Timoshenko, Faye and Martin2, Reference Schwartzbauer, Shete and Tami14 Often, the sphenopalatine and posterior nasal artery may not emerge in close proximity in the sphenopalatine foramen.Reference Schwartzbauer, Shete and Tami14 Thus, it follows that the success rate of sphenopalatine artery ligation is based on accurate identification and ligation of these responsible branches at the sphenopalatine foramen.Reference Holzmann, Kaufmann, Pedrini and Valavanis15, Reference Pothier, Mackeith and Youngs16
Anatomical variability
Wareing et al.,Reference Wareing and Padgham17 in 1998, were the first to propose a classification system of the osteology of the sphenopalatine foramen (Table I). The authors analysed 238 cadaveric lateral nasal walls and proposed 3 classes of sphenopalatine foramen opening. In class I cases (accounting for 35 per cent in that study), the opening of the sphenopalatine foramen is purely in the superior meatus, above the middle turbinate and the ethmoidal crest of the palatine bone. In class II cases (56 per cent), the sphenopalatine foramen spans the ethmoidal crest to open at the transition of the middle and superior meatus. In class III cases (9 per cent), there are two separate openings on either side of the ethmoidal crest, which in 98 per cent of cases lies anterior to the sphenopalatine foramen.
Table I Osteological classification of sphenopalatine foramenReference Wareing and Padgham17
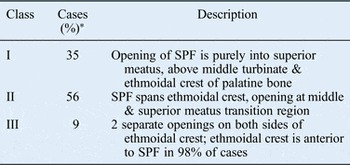
*As reported in Wareing et al.Reference Wareing and Padgham17 SPF = sphenopalatine foramen
Traditionally, identifying the bony ethmoidal crest of the palatine bone, onto which the middle nasal turbinate is attached, forms the basis for locating the sphenopalatine foramen for endonasal access. Since Wareing et al., only a limited number of studies have focused on identifying the anatomy of the sphenopalatine foramen and its relations. Most of the study findings were based on cadaveric dissection and have limited application in a surgical setting.
Materials and methods
A prospective analysis of 102 consecutive helical CT scans of the paranasal sinuses was carried out by 2 senior ENT surgeons. Distances from the sphenopalatine foramen to endoscopically palpable bony landmarks were measured. The following mean measurements were recorded on axial CT images: sphenopalatine foramen width and length; distances from the sphenopalatine foramen to the posterior fontanelle and to the inferior turbinates; and pterygomaxillary raphe width. On the coronal views, the vertical distance between the floor of the sphenopalatine foramen and the bony attachment of the inferior turbinate was measured (Figure 1). The sphenopalatine foramen was categorised as having the foramen opening either at, above or below the middle turbinate. Each of these measurements (Table II) were determined for the left and right sides, and verified by a second senior consultant.
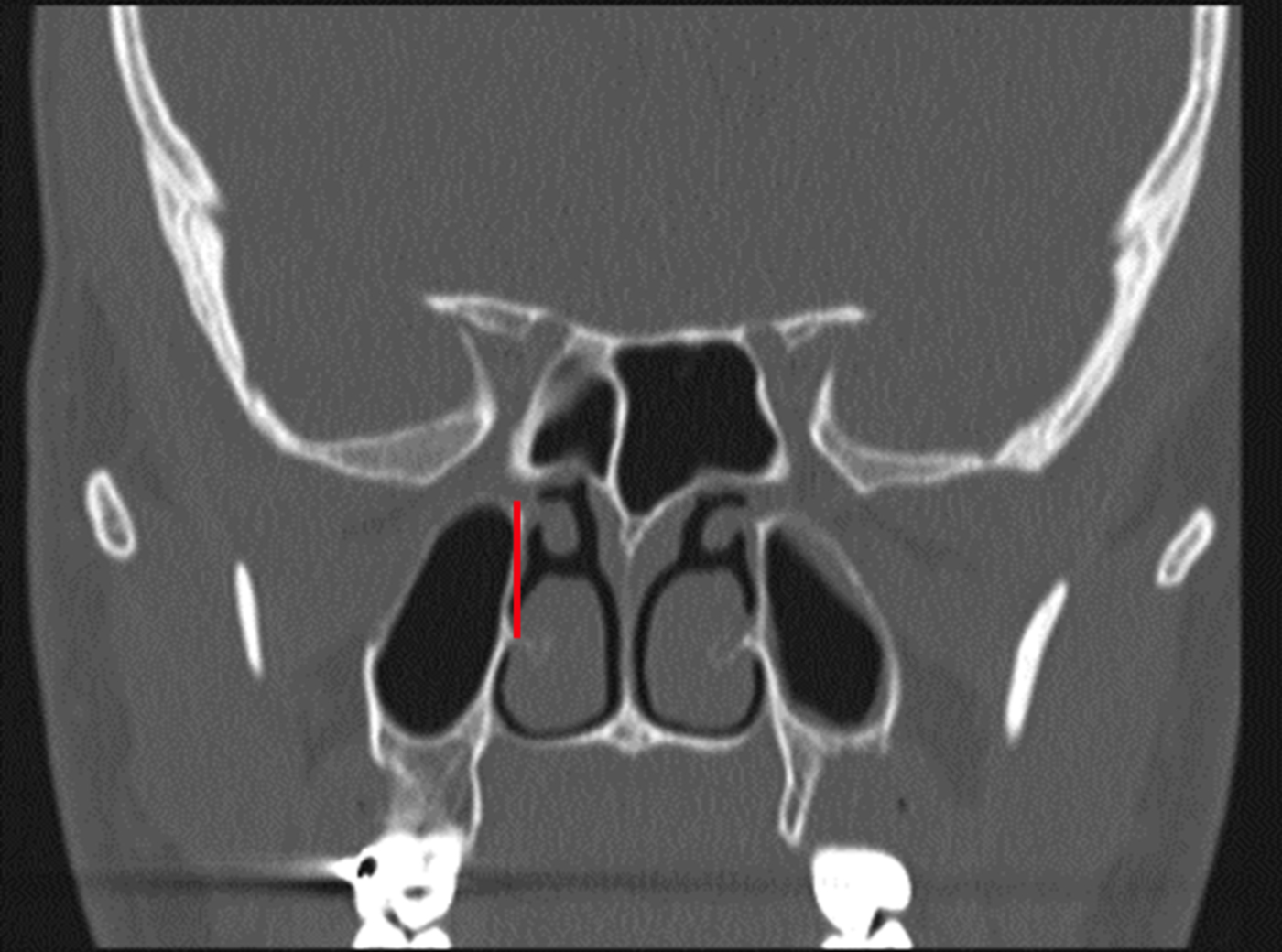
Fig. 1 Sphenopalatine foramen appears to open symmetrically at the level of the middle turbinate (red line), as shown on coronal computed tomography.
Table II Bony landmarks of sphenopalatine foramen
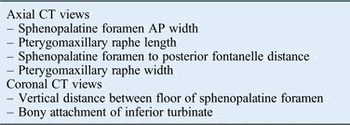
CT = computed tomography; AP = anteroposterior
Results
There were a total of 102 patients, comprising 45 females and 57 males with mean ages of 73 years and 51 years respectively (Table III). The mean distance from the posterior fontanelle to the sphenopalatine foramen was 14.1 mm (standard deviation (SD) = 2.13). The average vertical distance of the sphenopalatine foramen opening from the bony attachment of inferior turbinate was 14.13 mm. The average width of the sphenopalatine foramen was 4.62 mm (SD = 1.55). Data showing the relation of the sphenopalatine foramen to the middle turbinate are presented in Table IV.
Table III Patient demographics

*Total n = 102
Table IV Relation of sphenopalatine foramen distance to middle turbinate

Min = minimum; max = maximum; SD = standard deviation
The data were analysed for statistical differences between left and right sides and in terms of gender based on individual measurements. The data were first analysed in terms of symmetry. This revealed no significant difference between the left and right sides for any individual measurement. Differences in the average distances to the sphenopalatine foramen between genders were then compared. Analyses demonstrated no statistically significant difference between any of our measurements according to gender. Analyses revealed no statistically significant differences between any of the measurements (foramen width p-value = 0.714, distance from fontanelle p-value 0.43 and distance from inferior turbinate p-value = 0.48).
The measurement of most clinical relevance to endoscopic procedures was the distance of the sphenopalatine foramen to the posterior fontanelle; this average length was 14.1 mm (Table V). Notably, only 3 of 102 patients had measurements that lay outside of a 10–20 mm range (Figure 2). The SD was 2.13, indicating that 95 per cent of the sphenopalatine foramens in our sample population opened between 12 and 16 mm from the posterior wall of the fontanelle.
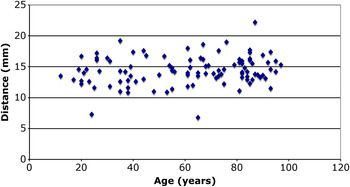
Fig. 2 Distance of the sphenopalatine foramen to the posterior fontanelle for all patients.
Table V CT Correlated landmarks for identifying sphenopalatine foramen

CT = computed tomography; PMR = pterygomaxillary raphe
Discussion
This study aimed to identify surgically reliable and reproducible landmarks for endoscopic approaches to the sphenopalatine foramen. The findings revealed a mean distance from the posterior fontanelle to the bony attachment of the inferior turbinate of 14.1 mm (SD = 2.13), with a mean sphenopalatine foramen width of 4.62 mm (SD = 1.55). Importantly, these measurements did not vary significantly with age or gender. The results of this work also reflect variability in the position of the sphenopalatine foramen, consistent with Wareing and colleagues'Reference Wareing and Padgham17 findings of three distinct patterns of sphenopalatine foramen position (Table I). Several cadaveric studies have confirmed this variability in the sphenopalatine foramen position (Table VI).Reference Prades, Asanau, Timoshenko, Faye and Martin2, Reference Midilli, Orhan, Saylam, Akyildiz, Gode and Karci12
Table VI Surgical landmarks for identifying sphenopalatine foramen

SPF = sphenopalatine foramen
Prades et al.Reference Prades, Asanau, Timoshenko, Faye and Martin2 performed a cadaveric analysis of 12 adult dry skulls under microscopy. The study aimed to locate the sphenopalatine foramen with emphasis on the sphenopalatine artery. The inferior border of the sphenopalatine foramen was situated 18.27 mm (range, 15.09–20.87 mm) above the horizontal plate of the palatine bone. It lay 13.04 mm (range, 9.01–14.85 mm) above the horizontal lamina of the inferior turbinate. Endoscopically, the posterior wall of the maxillary sinus was located at the level of or anteriorly within 10 mm of the anterior edge of the sphenopalatine foramen.Reference Prades, Asanau, Timoshenko, Faye and Martin2 In another study, by Simmen et al.,Reference Simmen, Raghavan, Briner, Manestar, Groscurth and Jones18 97 per cent of specimens had 2 or more branches, and 64 per cent of specimens had between 3 and 10 branches. The findings of the Prades et al.Reference Prades, Asanau, Timoshenko, Faye and Martin2 study were in agreement with the frequencies of the sphenopalatine foramen locations described by Wareing et al.,Reference Wareing and Padgham17 with the middle and superior meatus transitional region being the most frequent location.
Padua and VoegelsReference Padua and Voegels1 reported that the ethmoidal crest lay anterior to the sphenopalatine foramen in 98 per cent of cases. In that study, the sphenopalatine foramen most frequently lay at the transitional region of the middle and superior meatus (86.9 per cent), and less frequently at the superior meatus (13.1 per cent). The mean distance from the sphenopalatine foramen to the anterior nasal spine was 6.6 cm and to the accessory foramen was 6.7 cm, the latter of which is often found inferior and anterior to the sphenopalatine foramen. In endoscopic surgery, the ethmoidal crest may not be well demarcated. As the posterior ethmoidal cells lie just above the ethmoidal crest, this can be a particularly hazardous route.
Hadoura et al.Reference Hadoura, Douglas, McGarry and Young3 performed a radiological study of the sphenopalatine foramen that confirmed the validity of CT scans as an alternative to osteological studies. The anterior nasal spine on the plane of the piriform aperture was used as a fixed bony landmark. The mean distance from the sphenopalatine foramen to the nasal spine was 59.027 mm and to the piriform aperture was 48.481 mm, and the mean angle of elevation from the nasal floor was 22.5608 degrees.Reference Hadoura, Douglas, McGarry and Young3 Limitations of that study include the small sample size of 28 patients, inter/intra-observer variation and the use of surgically inappropriate landmarks.
To address the anatomical variations of the sphenopalatine foramen, Midilli et al.Reference Midilli, Orhan, Saylam, Akyildiz, Gode and Karci12 examined the bony landmarks of 20 cadaveric specimens. The sphenopalatine foramen appeared as a single foramen in 90 per cent of the specimens (n = 18); bony bridges created multiple foramens in the remaining two specimens. The sphenopalatine foramen was located superiorly to the horizontal lamina of the middle turbinate in 20 per cent of specimens (n = 4), and was located at the transition of the middle and superior meatus in 80 per cent of specimens (n = 16). The vertical distance between the inferior tip of the sphenopalatine foramen and the base of the nose was 22.1 ± 3.0 mm (range, 16.6–29.6 mm).Reference Midilli, Orhan, Saylam, Akyildiz, Gode and Karci12
Lee et al.Reference Lee, Kim, Kim, Son, Kim and Cho8 examined 50 mid-sagittal cadaver sections; in 45 specimens (90 per cent), the sphenopalatine foramen was located in the superior meatus, between the middle turbinate and the posterior horizontal end of the superior turbinate lamella, attaching to the lateral nasal wall. The distance from the anterior part of the nose to the sphenopalatine foramen was 49.1 ± 3.7 mm from the limen nasi, and was 59.4 ± 4.2 mm from the nasal sill.Reference Lee, Kim, Kim, Son, Kim and Cho8 During surgery, the ethmoidal crest that is exposed following removal of mucosa is often used as a landmark for the sphenopalatine foramen.
Scanavine et al.Reference Scanavine, Navarro, Megale and Anselmo-Lima4 examined 54 hemiskulls and 12 hemifaces from cadavers in order to determine the anatomical variation of the sphenopalatine foramen. The authors measured the opening of the sphenopalatine foramen and the anterior nasal spine, and determined that the mean distance from the anterior nasal spine to the sphenopalatine foramen was 55.24 ± 385 mm, whilst the mean angle between the nasal floor and sphenopalatine foramen was 25.8 degrees. The ethmoid crista was observed in 44 bone specimens (81.5 per cent) and was directed towards the inferior margin of the sphenopalatine foramen, in the superior meatus. Additionally, the superior nasal turbinate was noted to point towards the superior border of the sphenopalatine foramen in 55.6 per cent of cases. However, the role of these structures as landmarks remains unclear.
• Anatomical variations of the sphenopalatine foramen and its surroundings can hinder intra-operative visualisation, contributing to surgical failures
• The average vertical distance of the sphenopalatine foramen opening from the inferior turbinate bony attachment was 14.13 mm
• The average width of the sphenopalatine foramen was 4.62 mm (standard deviation = 1.55)
• The sphenopalatine foramen is a superior meatus opening at the posterior end of the middle turbinate attachment on the lateral nasal wall
• Inferior turbinate attachment and posterior fontanelle are reliable surgical landmarks for endoscopic approaches to the sphenopalatine foramen
None of the aforementioned studies identified a clinically relevant landmark in the endoscopic identification of the sphenopalatine foramen. The data from this work suggest that the posterior fontanelle and inferior turbinate are relevant and consistent landmarks for locating the sphenopalatine foramen during endoscopic sinus surgery. Furthermore, the identification of an accessory foramen on pre-operative CT imaging can be helpful in order to minimise therapeutic failure.
Surgery for sphenopalatine artery ligation may fail if dissection is not continued up to the posterior portion of the sphenopalatine foramen. This is because of the presence of arterial branches through the accessory foramen that are considered the primary source of bleeding.
Conclusion
This work suggests that the inferior turbinate attachment and posterior fontanelle may be used reliably as surgical landmarks for endoscopic approaches to the sphenopalatine foramen. The dimensions of the pterygomaxillary fissure and sphenopalatine foramen do not vary significantly with age or gender. Identification of the accessory foramina is important to correctly identify all branches of the sphenopalatine artery. Finally, the sphenopalatine foramen has a variable relationship to the posterior end of the middle turbinate and has a variable number of vessels passing through it.








