


Introduction
Rhino-orbital-cerebral mucormycosis is a dreaded opportunistic infection caused by the Mucorales group of fungi in immunosuppressed individuals.Reference Lin, Moua and Limper1 When the fungal spores are inhaled by an immunocompromised individual, the vascular endothelium is invaded,Reference Sugar, Mandell, Bennett and Dolin2 which causes endarteritis obliterans and angioinvasion, inducing a prothrombotic state and resulting in ischaemia and necrosis of tissues.Reference Jeong, Keighley, Wolfe, Lee, Slavin and Kong3,Reference Werthman-Ehrenreich4 The classical hallmark is necrotic black eschar or crust in the nasal cavity, nasal dorsum, palate or face. Orbital and cranial nerve involvement are classical indicators of the extent of disease. The mortality rate even with treatment is around 50 per cent.Reference Werthman-Ehrenreich4
The risk factors for rhino-orbital-cerebral mucormycosis include: uncontrolled diabetes mellitus, corticosteroid therapy, immunosuppressant drugs, haematological malignancies and organ transplantation.Reference Hirabayashi, Idowu, Kalin-Hajdu, Oldenburg, Brodie and Kersten5 Immunocompetent individuals are hardly ever infected.Reference Bottone, Weitzman and Hanna6 To our surprise, coronavirus disease 2019 (Covid-19) infection and its management have caused significant immunosuppression in otherwise immunocompetent individuals, inviting opportunistic infections. India is a diabetic capital, with 47 per cent of Indians being unaware of their diabetes and only one-fourth achieving glycaemic control.Reference Sen, Lahane, Lahane, Parekh and Honavar7,Reference Prenissl, Jaacks, Mohan, Manne-Goehler, Davies and Awasthi8 Diabetes mellitus type II is associated with a two-fold increase in mortality as well as severity of Covid-19 relative to non-diabetic patients.Reference Kumar, Arora, Sharma, Anikhindi, Bansal and Singla9,Reference de Almeida-Pititto, Dualib, Zajdenverg, Dantas, de Souza and Rodacki10
The full spectrum of Covid-19 is still unfolding. As we know, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has a propensity for diffuse alveolar damage and severe inflammatory exudation, with a picture of immunosuppression and alteration in innate immunity due to reduced cluster of differentiation 4 and cluster of differentiation 8 T-cell counts.Reference Yang, Cao, Qin, Wang, Cheng and Pan11 A decrease in lymphocytes and an increase in neutrophils with a rise in inflammatory markers lead to co-infections.Reference De Pauw, Walsh, Donnelly, Stevens, Edwards and Calandra12 It has been reported in the literature that Covid-19 patients admitted to the intensive care unit, on mechanical ventilation, and staying in hospital for longer than 50 days, are more prone to fungal co-infections.Reference Yang, Yu, Xu, Shu, Xia and Liu13 The majority of patients develop symptoms of rhino-orbital-cerebral mucormycosis after recovering from Covid-19, indicating the importance of follow up in high-risk Covid-19 patients.Reference Sen, Lahane, Lahane, Parekh and Honavar7
Rhino-orbital-cerebral mucormycosis has now been declared a notifiable disease by the Government of India, with the intention of gathering nationwide data. Only early detection and correct management at the earliest stage can help save lives. The warning signs and symptoms are the development of nasal obstruction, nasal crusting, foul or bloody nasal discharge, blackening of the nose or cheek, unilateral facial or orbital pain, facial numbness, toothache, loosening of teeth, palatal eschar, facial palsy, headache, peri-orbital swelling, diplopia, blurred vision, ptosis, proptosis, reduced vision, and focal seizures.Reference Honavar14
We present a series of 41 patients with mucormycosis associated with Covid-19, along with the diagnostic and management challenges. Otorhinolaryngologists, maxillofacial surgeons and dentists should be motivated to report such cases of co-infection in order to reveal the wide spectrum of the disease and to add data to the pool of literature on a global level.
Materials and methods
We performed an analysis of 41 patients with rhino-orbital-cerebral mucormycosis at our tertiary healthcare centre over three months. The history, clinical presentation, examination findings, associated co-morbidities, diagnostic modalities, medical and surgical management, and outcomes were analysed. Consent was obtained from all patients. The included patients had Mucor confirmed on direct microscopic examination, showing broad aseptate fungal hyphae, associated with a current or past history of Covid-19 infection.
Based on the clinical findings and potassium hydroxide calcofluor white mount smear report, systemic antifungals were started. Lyophilised amphotericin B, which is available for free in our institute thanks to the Government of Rajasthan, was started at doses of 1–1.5 mg/kg/day. Liposomal amphotericin B was started for patients with deranged kidney function tests and those hypersensitive to lyophilised amphotericin B at the dose of 5 mg/kg/day, maximum 10 mg/kg/day for extensive infection and central nervous system involvement.Reference Cornely, Alastruey-Izquierdo, Arenz, Chen, Dannaoui and Hochhegger15 Contrast-enhanced magnetic resonance imaging and contrast-enhanced computed tomography were performed to ascertain the extent of disease. An amphotericin B chart, comprising information on daily dosing, cumulative dose, serum electrolytes, renal function tests, input/output volume, fasting blood sugar, haemoglobin, magnesium, calcium, erythrocyte sedimentation rate and C-reactive protein, was updated every day for all patients. Surgical procedures performed included endoscopic endonasal debridement by Denker's approach, maxillectomy, and orbital exenteration with permanent tarsorrhaphy in selected cases. Post-operative systemic antifungals were continued.
Results
There were 41 patients, with a male-to-female ratio of 28:13, who presented to us at a mean age of 48.2 years (range, 21–68 years). The clinical and demographic details are described in Table 1. Six patients were positive for Covid-19 on reverse transcription polymerase chain reaction testing at the time of presentation, and 35 had recovered from Covid-19 with negative results on reverse transcription polymerase chain reaction testing.
Table 1. Patients’ demographic details and clinical spectrum
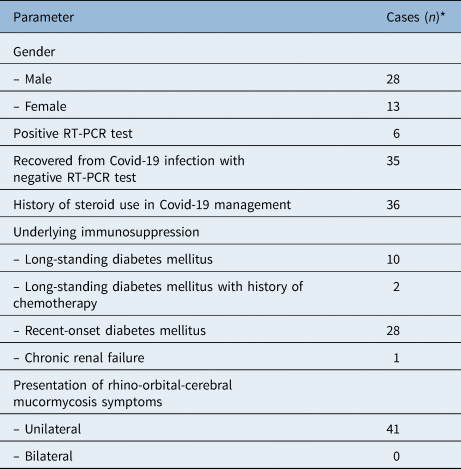
*Total n = 41. RT-PCR = reverse transcription polymerase chain reaction; Covid-19 = coronavirus disease 2019
Thirty-six patients had a history of corticosteroid usage, while oxygen supplementation was used by 22 patients. Twelve patients had long-standing diabetes mellitus, five of them having uncontrolled glycaemia with a mean glycated haemoglobin (haemoglobin A1C) of 8.34 per cent. Twenty-eight patients were diagnosed with recent-onset diabetes mellitus and had a mean glycated haemoglobin of 9.08 per cent. Two patients in our series had undergone chemotherapy. One patient had chronic renal failure and was on haemodialysis.
The symptoms of rhino-orbital-cerebral mucormycosis presented 2–48 days after Covid-19 infection. Clinical symptoms were divided into five categories; their incidence is described in Table 2.
Table 2. Incidence of various clinical presentations of rhino-orbital-cerebral mucormycosis

*Total n = 41
The symptoms of rhino-orbital-cerebral mucormycosis include nasal, orbital, facial, oral and intracranial signs. The most common nasal sign is black turbinate. Others include nasal blockade and crusting, and foul-smelling black discharge (Figure 1a). These symptoms were present in 39 patients. The most common orbital sign is ptosis. Others include peri-orbital oedema and pain, ophthalmoplegia, chemosis, necrosis, proptosis, diplopia, and blurred or reduced vision (Figure 1b–d). These symptoms were present in 36 patients. The facial signs are most commonly facial palsy, cheek swelling or numbness, and cheek or nasal dorsum blackening (Figure 1e and 1f). These symptoms were present in 10 patients. The most common oral sign is palatal eschar or discoloration. Others include loosened teeth and dental pain (Figure 1g and 1h). These symptoms were present in 19 patients. The intracranial signs include altered sensorium, paralysis and focal seizures. These symptoms were present in nine patients.

Fig. 1. Clinical pictures showing: (a) nasal sign – black coloured right middle turbinate (the earliest sign); (b–d) orbital sign – ptosis of right eye, necrosis and crusting of left eye, chemosis and complete ophthalmoplegia of right eye; (e & f) facial sign – blackening of left cheek, left facial palsy, and involvement of IIIrd and VIth cranial nerves; and (g & h) oral sign – palatal discoloration and eschar formation. Published with patients' permission.
The maxillary sinus was the most common sinus involved, implicated in 68.2 per cent of patients (28 out of 41); all four sinuses were involved in 29.2 per cent of patients (12 out of 41). The orbital apex was involved in 24.3 per cent of patients (10 out of 41), and cavernous sinus thrombosis was seen in 19.5 per cent (8 out of 41). Infratemporal fossa with pterygopalatine fossa involvement was seen in 17 per cent of patients (7 out of 41). Contrast-enhanced magnetic resonance imaging was helpful to identify the extent of disease and was also performed in the post-operative period to determine the response to amphotericin B and detect residual disease (Figure 2). Thrombosis of the internal carotid artery was seen in one patient. A middle cerebral artery infarct was present in two patients. Unfortunately, none of these three individuals survived. Five patients had unilateral loss of vision with no perception of light.

Fig. 2. Contrast-enhanced magnetic resonance imaging scans showing: (a–c) involvement of maxillary sinus and intra-orbital extension in coronal planes; (d & e) involvement of intraconal orbit and intracranial extension in axial planes; and (f) post-operative right orbital exenteration showing no residual disease (axial plane).
The mode of management and outcomes are described in Table 3. Four patients refused admission, while three refused surgery. Endoscopic endonasal debridement with Denker's approach was performed in 21 patients, total maxillectomy in 6 patients, and orbital exenteration with eyelid sparing in 4 patients. At the last follow up, 37 patients were alive and on antifungal therapy.
Table 3. Management and outcomes of rhino-orbital-cerebral mucormycosis patients

*Total n = 41
Discussion
Coronavirus disease 2019 infection is a global public health disease emergency,Reference Zhou, Yang, Wang, Hu, Zhang and Zhang16 and it is giving rise to another life-threatening emergency of rhino-orbital-cerebral mucormycosis. Although the incidence is 0.005–1.7 per million,Reference Wang, Wang, Chen and Qin17 cases are increasing at present. If an immunocompromised patient suffers from Covid-19, the propensity for co-infection with mucormycosis is high. In addition, if an immunocompetent patient suffers from Covid-19, the resultant immunosuppression due to the disease and its management per se can lead to rhino-orbital-cerebral mucormycosis.
During the severe acute respiratory syndrome outbreak in 2003 caused by SARS-CoV-1, the incidence of co-infection with the fungus was 14.8–27 per cent, which was an eye-opener.Reference Sharma, Grover, Bhargava, Samdani and Kataria18,Reference Zhang, Li, Huang, Cao and Hao19 There exists a similarity between SARS-CoV-2 and the previous SARS-CoV-1.Reference Peeri, Shrestha, Rahman, Zaki, Tan and Bibi20 The proteomic similarity analyses of both the strains showed highly homologous behaviour (95–100 per cent), and they share 76 per cent sequence similarity in their S proteins.Reference Kaur, Singh, Dar, Bijarnia, Dhingra and Kaur21
The lethal triad of Covid-19, uncontrolled diabetes mellitus and corticosteroid therapy carries the highest risk for rhino-orbital-cerebral mucormycosis and ultimately results in exhausted immunity. Other risk factors include organ or bone marrow transplantation, neutropenia, other forms of metabolic acidosis, increased serum iron levels, malignant haematological disorders, deferoxamine, and iron chelation therapy in patients receiving haemodialysis.Reference Waizel-Haiat, Guerrero-Paz, Sanchez-Hurtado, Calleja-Alarcon and Romero-Gutierrez22,Reference Serris, Danion and Lanternier23 Coronavirus disease 2019 infection results in lymphopenia, reduced cluster of differentiation 4 and 8 counts, and an inflammatory cytokine surge.Reference Liu, Li, Liu, Liang, Wang and Wang24 It induces a prothrombotic and diabetogenic state by direct viral infection of endothelial cells and diffuse endothelial inflammation.Reference Liu, Li, Liu, Liang, Wang and Wang24–Reference Mehta and Pandey26 In our series, 14.6 per cent of patients were positive for Covid-19 on reverse transcription polymerase chain reaction testing at the time of presentation.
Uncontrolled diabetes mellitus results in impaired neutrophil function, leading to defective chemotaxis, transmembrane migration and reduced superoxide production. It causes reduced binding of transferrin to iron in acidotic conditions and favours Mucor growth. By increasing 78-kDa glucose-regulated protein GRP78, it mediates invasion of and damage to human endothelial cells. Through structural and functional modifications of platelets, it results in a defect in membrane properties and alterations of nitric oxide metabolism. The active ketone reductase system in uncontrolled diabetes favours Mucor growth in the acidic and glucose-rich environment.Reference Lim, Bae, Kwon and Nauck27 Those with diabetes are at a higher risk for complications and mortality than non-diabetics.Reference Kumar, Arora, Sharma, Anikhindi, Bansal and Singla9,Reference de Almeida-Pititto, Dualib, Zajdenverg, Dantas, de Souza and Rodacki10,Reference Apicella, Campopiano, Mantuano, Mazoni, Coppelli and Del Prato28 In our series, 29.2 per cent of patients had long-standing diabetes mellitus, while 68.2 per cent had been diagnosed with recent-onset diabetes mellitus.
Corticosteroid therapy results in hyperglycaemia and causes impaired neutrophil migration and phagolysosome fusion.Reference White, Dhillon, Cordey, Hughes, Faggian and Soni29 As we have no definitive management for Covid-19, only systemic corticosteroids have been shown to improve survival in patients with immunomodulation-related lung damage.Reference Müller, Groß, Conzelmann, Krüger, Merle and Steinhart30,Reference Sterne, Murthy, Diaz, Slutsky and Villar31 In our series, 87.8 per cent of patients had a history of corticosteroid usage. Cases of rhino-orbital-cerebral mucormycosis can be reduced by the cautious use of steroids with careful titration and strict sugar monitoring.
According to Indian guidelines, moderate cases should receive systemic methylprednisolone 0.5–1 mg/kg/day or dexamethasone 0.1–0.2 mg/kg for 3 days within 48 hours of admission if inflammatory markers are raised or the need for mechanical ventilation is present. Severe cases should receive systemic methylprednisolone 1–2 mg/kg/day or dexamethasone 0.2–0.4 mg/kg for 5–7 days.Reference Sen, Lahane, Lahane, Parekh and Honavar7 A European Confederation of Medical Mycology study reported a 46 per cent incidence of corticosteroid therapy administration one month before Mucor, and 44 per cent of patients had a history of immunosuppressant drugs.Reference Skiada, Pagano, Groll, Zimmerli, Dupont and Lagrou32
The incidence of superadded co-infections with fungi and bacteria in hospitalised Covid-19 patients is documented as 8 per cent. Broad-spectrum antibiotics were used in 72 per cent of patients.Reference Rawson, Moore, Zhu, Ranganathan, Skolimowska and Gilchrist33 Song et al. reported that these opportunistic infections are more common in the middle and later phases of infection.Reference Song, Liang and Liu34 White et al. stated that the mortality rate among Covid-19 patients with mucormycosis is 53 per cent, while those without mucormycosis have a reduced mortality rate of 31 per cent.Reference White, Dhillon, Cordey, Hughes, Faggian and Soni29 In our series, one death was observed among active Covid-19 patients. The remaining three deaths occurred in patients who were negative for Covid-19 at that time.
Extensive examination of patients suffering and recovered from Covid-19, and awareness of the warning signs, allow detection of the dreaded complication at an early stage. The goals of mucormycosis management include reversal of the underlying immunosuppression; in addition, systemic antifungals reduce fungal load and aggressive debridement can enhance penetration of antifungal therapy.Reference Liu, Li, Liu, Liang, Wang and Wang24 Topical therapy with amphotericin B increases the local penetration of the drug and enhances outcomes. A delay of even 6 days in commencing treatment increases the mortality from 35 per cent to 66 per cent.Reference Sen, Lahane, Lahane, Parekh and Honavar7 The prognosis is poor even after all efforts, with 33.3–80 per cent mortality, and even more than 80 per cent mortality in poorly managed cases.Reference Jung, Kim, Park, Song, Cho and Lee35
First-line therapy is liposomal amphotericin B, amphotericin B lipid complex and oral posaconazole suspension. Isavuconazole is used as salvage therapy.Reference Cornely, Alastruey-Izquierdo, Arenz, Chen, Dannaoui and Hochhegger15 The ideal duration of amphotericin B treatment is unclear, and there are no guidelines. We should monitor the individual's response by assessing inflammatory markers, serum electrolytes and renal function test results during the clinical response. The cost of amphotericin B carries a financial burden and can be back-breaking for a poor healthcare system. In one Indian study, 24.3 per cent of patients left hospital because of the high anticipated costs associated with mucormycosis management.Reference Patel, Kaur, Xess, Michael, Savio and Rudramurthy36 Treatment for Covid-19 is already a financial burden, and liposomal amphotericin B is adding to it.
We performed endoscopic endonasal debridement with Denker's approach in 21 patients and found the maxillary sinus to be the most commonly involved, implicated in 19 patients (90 per cent), followed by the ethmoid sinuses in 78 per cent, sphenoid sinus in 58 per cent and frontal sinus in 20 per cent of cases. On the contrary, Sharma et al. stated that the ethmoids were the most commonly affected sinuses in their study of 23 patients with coronavirus-associated mucormycosis.Reference Sharma, Grover, Bhargava, Samdani and Kataria18 It has been stated that disease limited to sinonasal areas can be managed by endoscopic debridement, and up to 94.4 per cent success can be achieved.Reference Sen, Lahane, Lahane, Parekh and Honavar7 Total maxillectomy was performed in six patients because of palatal and cheek involvement. Orbital exenteration with eyelid sparing was performed in four patients in our series because function and cosmesis could not be salvaged in the presence of extensive orbital involvement. There are no guidelines for orbital exenteration.Reference Sen, Lahane, Lahane, Parekh and Honavar7 At the last follow up, 37 patients were alive and on antifungal therapy.
• Coronavirus disease 2019 (Covid-19), its management and other co-morbidities result in immunosuppression, which invites lethal fungal infection
• Management protocols for Covid-19 are the same globally
• An emerging epidemic of rhino-orbital-cerebral mucormycosis in India is concerning, and adds to the economic and financial burdens of the healthcare infrastructure
• Follow up of high-risk Covid-19 patients to optimise immunity can help reduce rhino-orbital-cerebral mucormycosis
• We can learn from our dealings with this combination of viral and fungal infection, to better combat future casualties
• International collaboration for pandemic and epidemic planning is needed to ensure a better outcome, with minimal loss to humanity
Acknowledgements
We would like to acknowledge the contribution of junior residents, Dr Karishma Agarwal, Dr Umang Vyas, Dr Ruchika Gupta and Dr Preeti Dhakad, for the collection of clinical pictures.
Competing interests
None declared





