


Introduction
Auditory canal exostoses are known to have a higher prevalence in cold-water recreation enthusiasts.Reference DiBartolomeo1, Reference Wong, Cervantes, Doyle, Karamzadeh, Boys and Brauel2 Regular surfers are particularly at risk. The literature suggests a prevalence of 70–86 per cent in those surfing during winter, without ear plugs, for a period of more than 5–10 years, or those surfing more than 50 times per year for less than 5 years.Reference Deleyiannis, Cockroft and Pinczower3–Reference Nakanishi, Tono and Kawano6 It is for this reason that the condition is generally referred to as ‘surfer's ear’. It is well documented that increased severity of auditory exostoses is associated with longer exposure to lower water and air temperatures, increased duration of recreation, and increased frequency of exposure.Reference Deleyiannis, Cockroft and Pinczower3, Reference Chaplin and Stewart5, Reference Nakanishi, Tono and Kawano6
A drill or chisel are the commonly described tools used to remove the exostoses. We describe a novel technique for treatment of exostoses involving the use of a piezo saw, which has been used safely in other forms of ear surgery.
Technique
The procedure was performed under general anaesthesia. The ear canal was infiltrated with 2 per cent lignocaine with 1:80 000 adrenaline. Permeatal incisions were placed to raise flaps from the exostoses: a laterally based flap for the lateral surface of the exostosis and a medially based flap for the medial side. A piezo saw (Piezoflex; Mectron, Loreto, Italy) was used to reduce the exostoses layer by layer, with a medial to lateral motion. The ear canal was widened and full visualisation of the tympanic membrane was achieved (Figures 1 and 2). The medial and lateral flaps of the ear canal skin were repositioned, and the ear canal was dressed in Spongostan™. A two-week course of antibiotic ear drops was prescribed.

Fig. 1. Pre-operative photograph showing ear canal exostoses.
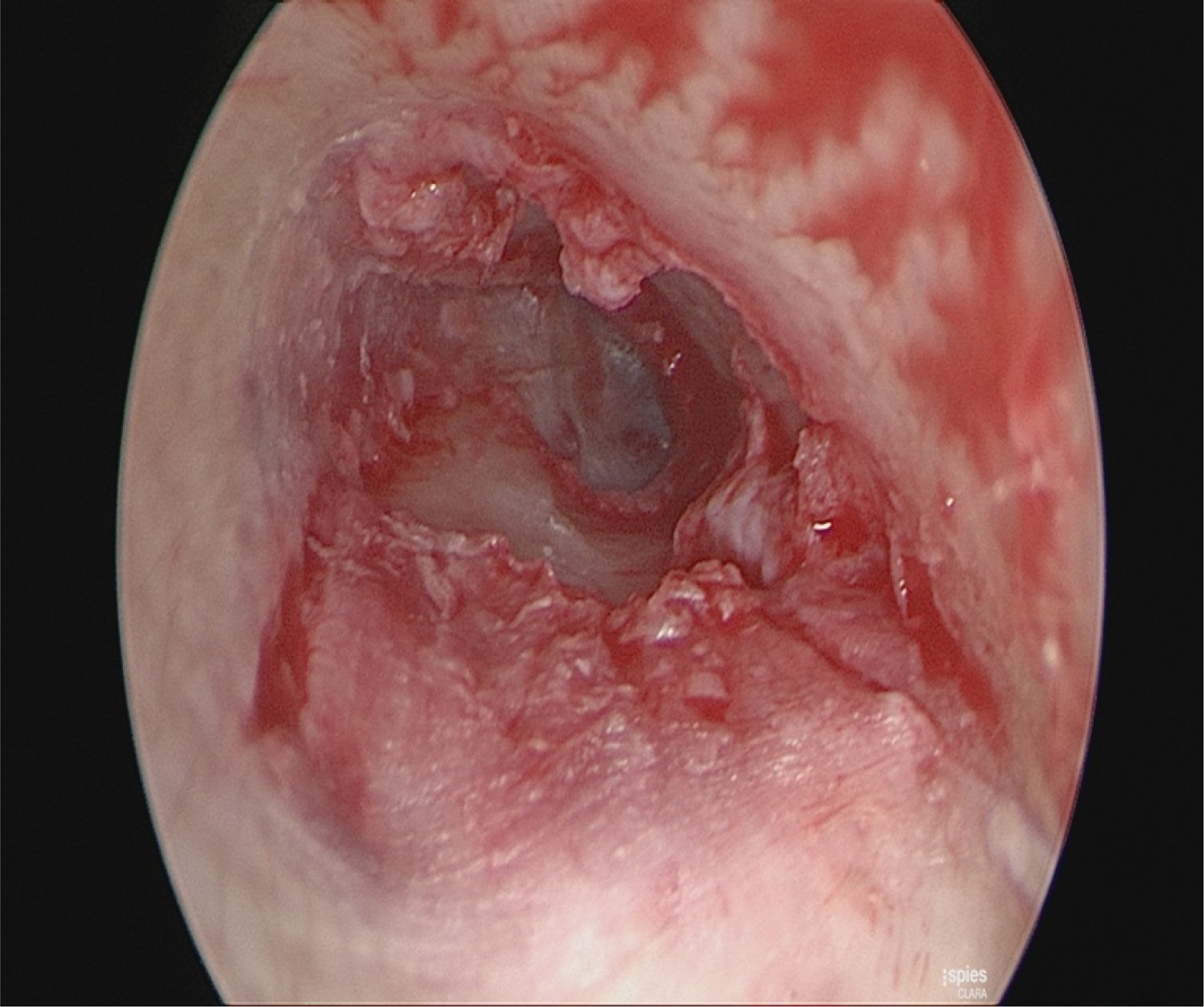
Fig. 2. Photographic view of the tympanic membrane and preserved ear canal skin following removal of exostoses.
Following surgery, the patient was reviewed on the first, second and fourth week, which showed a well-healed ear canal. The frequent follow up was necessary to monitor the outcome of this novel surgery. Follow up can probably be reduced to a single out-patient visit once the procedure is performed routinely. Post-operative pain had resolved within the first week, as well as mild tinnitus in the ear, which was probably due to the packing in the ear. No facial weakness or change in hearing was noted.
Discussion
The commonly described techniques for removing exostoses involve using a drill or a chisel. A study comparing the experience of both a drill and micro-chisel advocated using the chisel for larger laterally based exostoses and the drill for medially based lesions as a time-efficient technique.Reference Barrett, Ronan, Cowan and Flanagan7 Excision of exostoses using a drill is carried out preserving as much canal wall skin as possible. If skin flaps are left intact, then healing by primary intention is possible. If skin is lost, then a process of healing by secondary intention takes place; this is slower and means that the patient must keep their ears drier for longer. They may also require more follow-up appointments.
Complications of drill excision include risk to the facial nerve via direct or thermal injury, deafness, perforation of the eardrum, and post-operative stenosis. One study found an overall complication rate of 12.5 per cent.Reference Stougaard and Tos8 Two studies of 65 and 59 patients reported post-operative canal stenosis rates of approximately 1 per cent.Reference Frese, Rudert and Maune9, Reference Timofeev, Notkina and Smith10
The use of a piezo saw in the treatment of ear canal exostoses has not been described previously in the literature. The piezoelectric system is a surgical cutting tool. It operates at an ultrasonic frequency, and is active on mineralised tissue only, such as teeth and bone. It does not damage the surrounding soft tissues, such as skin, nerves or mucosa.Reference Labanca, Azzola, Vinci and Rodella11
Although the surgical time needed to excise the exostoses using a piezo saw is longer compared to using a drill or chisel, the device offers very high precision cutting via a number of differently sized and shaped probes, reducing complications to surrounding structures. The precise removal of the exostoses whilst preserving the canal skin assists in speedy recovery, within two to three weeks, which enables patients to resume water sports quickly. In contrast, the recovery time using a drill or a chisel can be up to five weeks. It is hoped that the safety profile of the device will allow bilateral surgery in the future, with the principle aim of a significant reduction in recovery time for the patient. The surgeon at our institution found that operative times decreased with experience.
The cost of the disposable piezo surgery or drill instrument sets used for removing exostoses are similar. The osteotomy insert (piezo saw) and irrigation tubing cost approximately £277, and the burr (based on an average of three different sizes) along with the irrigation cassette used to drill the exostoses cost £280.
The piezo saw system is already used by maxillofacial surgeons for osteotomy,Reference Salami, Dellepiane, Proto and Mora12 and has been successfully used for a variety of ear surgical procedures, including atticotomy, stapedotomy and facial nerve decompression.Reference Labanca, Azzola, Vinci and Rodella11 Salami et al. found no side effects on middle- or inner-ear structures.Reference Labanca, Azzola, Vinci and Rodella11 The device has also been used to remove osteomata from the ear canal.Reference Salami, Mora, Dellepiane and Guastini13 Osteomas are benign, pedunculated solitary bony tumours that arise in the bony ear canal, unlike exostosis which have a broad base and are multiple. One paper describes 10 patients who underwent successful surgery for osteoma without otological or other complications.Reference Salami, Mora, Dellepiane and Guastini13
With its soft tissue preserving characteristics, the piezo saw has the potential to remove canal bone without compromising the overlying skin. Additionally, with minimal complications to the surrounding structures, it is a safer technique than that using a conventional drill or micro-chisel. Faster healing should allow surfers an earlier return to their sport.
Conclusion
Excision of ear canal exostoses using a piezo saw is a safe technique and patients have a speedy recovery. We have described a new technique for removing exostoses, one which has been used to perform other otological procedures with no side effects.
The safety profile of the piezo saw when used in other otological surgical procedures raises the possibility of its future use in bilateral surgery. This would further minimise surfers’ time out of the water.
Competing interests
None declared.


