



Introduction
The endoscopic transcanal transpromontorial approach was introduced to establish a direct corridor to the internal auditory canal. The transcanal transpromontorial approach has attracted the attention of surgeons because of its minimally invasive features, including no or very partial soft tissue dissection, limited drilling of the temporal bone, no need for craniotomy, no cerebellar or temporal lobe retraction, and a direct and straight view of the surgical target.
Furthermore, pathological lesions invisible under an optical microscope can be identified and removed using an angled endoscope and the applied tools. However, the surgical field through the ear canal is limited. The middle ear is surrounded by the labyrinth, petrous carotid artery, facial nerve, internal and external acoustic canal, Eustachian tube, jugular bulb, and the middle and posterior cranial bases.Reference Komune, Matsuo, Miki and Rhoton1 This makes careful identification of the surgical landmarks essential to prevent the risks involved in the surgery. Preservation of the facial nerve should be prioritised, although hearing and vestibular impairments are unavoidable during tumour removal. Identification and preservation of segments of the facial nerve originating from the fundus of the internal auditory canal are essential.
This study aided our understanding of a three-dimensional (3D) transcanal transpromontorial approach to the internal auditory canal by measuring the distances and angles of the surgical landmarks using 3D computed tomography (CT) and analysing the origin of the facial nerve labyrinthine segment from the internal auditory canal.
Materials and methods
This study retrospectively examined 48 ears of 24 patients (12 males and 12 females; 20–74 years old) using 3D reconstructions of normal temporal bone CT scan data. We performed high-resolution CT imaging (Somatom Definition AS + 128; Siemens, Seoul, Korea) of the temporal bone (section thickness, 0.6 mm; length and width, 500 and 2600 mm, respectively; field of view, 512 × 512 pixels). The 3D reconstructed images were obtained using V-works three-dimensional reconstruction software (version 4.0; CyberMed, Seoul, Korea) to analyse the axial scans. Patients who had a previous history of head trauma, radiologically abnormal findings including fracture lines, tumours and chronic otitis media, or a history of temporal bone surgery were excluded from the study.
All procedures complied with national and institutional guidelines for human experimentation (approval number: UC12RISE0064) and the 1975 Declaration of Helsinki (revised in 2008). The need for informed consent was waived because this retrospective study examined radiographical images only.
The inner structures of the temporal bone were reconstructed three-dimensionally. Eight points were marked in the 3D objects with reference to the axial, coronal and sagittal plane images of the CT scans as follows: point 1: the highest level of the jugular bulb; point 2: the posterior wall of the ascending petrous internal auditory canal at the level of the hypotympanum; point 3: the level of the Eustachian tube; point 4: the cochlear apex; point 5: the facial nerve at the centre of the geniculate ganglion; point 6: the centre of the second genu; point 7: the branch of the chorda tympani nerve; and point f: the branch of the labyrinthine segment from the internal auditory canal. Distances and angles to each point were measured from the oval window and round window (Figure 1).

Fig. 1. The inner structures of the temporal bone were three-dimensionally reconstructed. Eight points were marked in the three-dimensional object (a) with reference to a three-dimensional cursor of the axial (b), sagittal (c) and coronal (d) plane images of a computed tomography scan. The white arrow shown in b–d indicates the points where the labyrinthine segment of the facial nerve branches from the internal auditory canal. Point 1: the highest level of the jugular bulb; point 2: the posterior wall of the ascending petrous internal auditory canal at the level of the hypotympanum; point 3: the level of the Eustachian tube; point 4: cochlear apex; point 5: facial nerve at the centre of the geniculate ganglion; point 6: centre of the second genu; point 7: the branch of the chorda tympani nerve; and point f: the branch of the labyrinthine segment from the internal auditory canal. A = anterior; R = right; L = left; H = highest; P = posterior; F = floor
Using an imaginary plane connecting three points, the angle between the planes and the distance to point f were calculated (Figure 2). Distances (d) to each point (P) were measured from the oval window (O; dPnO) and round window (R; dPnR). Angles (a) to each point were measured from the oval window (aPnOR) and round window (aPnRO), which were based on a line passing through the oval window and round window (Figure 3).

Fig. 2. The inner structures of the temporal bone were three-dimensionally reconstructed. The angle between the planes, acquired using three points, was measured. The two angles (aPLf45PLfOR and aPLf45PLf67) between the planes were measured. The vertical distances (dPL567Pf) to the plane (PL567) from point f were also determined. Point 1: the highest level of the jugular bulb; point 2: the posterior wall of the ascending petrous internal auditory canal at the level of the hypotympanum; point 3: the level of the Eustachian tube; point 4: cochlear apex; point 5: facial nerve at the centre of the geniculate ganglion; point 6: centre of the second genu; point 7: the branch of the chorda tympani nerve; and point f: the branch of the labyrinthine segment from the internal auditory canal. a = angle; PL = plane; O = oval window; R = round window; d = distance; P = point

Fig. 3. (a) Distances to each point were measured from the oval window (dPnO) and round window (dPnR). (b) Angles to each point were obtained from the oval window (aPnOR) and round window (aPnRO), which were based on the line passing through oval window and round window. d = distance; P = point; O = oval window; R = round window
All data were measured in triplicate, and average values were calculated. The means and standard deviations of the measured values were subjected to statistical analyses.
Results
Distance dPnO was longer than dPnR at the beginning of P1 and shorter after P4 in the P1 to P5 section. Angle aPnOR gradually increased, and aPnRO gradually decreased. Angle aPnOR was larger than aPnRO at the beginning of P1 and smaller after P4. The measurements for dP4O and dP4R were similar. The values of aP4OR and aP4RO were also similar (Figure 3). The value of aPfOR was between those of aP4OR and aP5OR (Table 1 and Figure 3).
Table 1. Distances and angles to each point from the line connecting the oval window and round window

d = distance; P = point; O = oval window; R = round window; SD = standard deviation; a = angle
The angle between the plane (PL) PLf45 and the plane PfOR was 93.18 ± 16.32°. The angle between the plane PLf45 and the plane PLf67 was 90.26 ± 12.80°. The distance from Pf to the imaginary plane PL567 was 4.19 ± 0.54 mm. The average distance from the centre of the oval window to the centre of the round window was 2.65 ± 0.36 mm (Table 2).
Table 2. The angle between the planes, the distance to point f from the planes and the distance between the two centres of the oval window and round window

SD = standard deviation; d = distance; PL = plane; P = point; OR = oval and round window
Discussion
Following the development of endoscopic middle-ear surgery, the number of reports of a direct approach to the internal auditory canal to remove vestibular schwannoma has increased. However, the disadvantages include limited access, difficult haemostasis, and difficulty removing the tumour when it extends through the porus and cerebellopontine angle. Therefore, the endoscopic transcanal transpromontorial approach technique was clinically proposed to remove vestibular schwannomas limited to less than 1 cm in diameter involving the most lateral portion of the internal auditory canal and tumours more than 1 cm but less than 2 cm involving the cerebellopontine angle, classified as Koos grading scale stage I and II, respectively.Reference Marchioni, Carner, Soloperto, Bianconi, Sacchetto and Sacchetto2
The disadvantages and limitations of surgery have been improved following various trials and previous studies. For example, Marchioni et al. removed tumours equal to or less than 3 cm in size with linear progression into the cerebellopontine angle using an expanded transcanal transpromontorial approach technique with a microscope and endoscope.Reference Marchioni, Carner, Soloperto, Bianconi, Sacchetto and Sacchetto2 They reported preservation of facial nerve function in 95.9 per cent of cases using this technique (House–Brackmann grade I–II) with stable results at follow up; facial nerve function was reduced in 4.1 per cent of cases but was no worse than grade III.Reference Marchioni, Soloperto, Masotto, Fabbris, Rossi and Villari3
Another criticism of this approach is that it requires the removal of the cochlea to access the internal auditory canal and therefore precludes possible simultaneous or subsequent cochlear implantation. A transcanal infrapromontorial route with near-total cochlear preservation was performed by Rubini et al., who removed only the most posterior portion of the basal turn of the cochlea in cadaveric dissections. This approach may be considered an option for removing small intracanalicular schwannomas (less than 0.5 cm cerebellopontine angle spread) when concurrent cochlear implantation is indicated.Reference Rubini, Bianconi, Patel and Marchioni4 However, to reach the internal auditory canal without damaging the cochlea, the infracochlear corridor must have a specific anatomical geometry to allow adequate visualisation while avoiding the jugular bulb and internal carotid artery. First, to allow for safe passage past the jugular bulb and internal carotid artery, the diameter of the infracochlear tunnel must be more than 3 mm to accommodate both an endoscope and drill.Reference Kempflea, Fiorilloa, Kanumuria, Barbera, Edgea and Cunnanea5 An aberrantly high jugular bulb can limit the surgical approach (Figure 4).
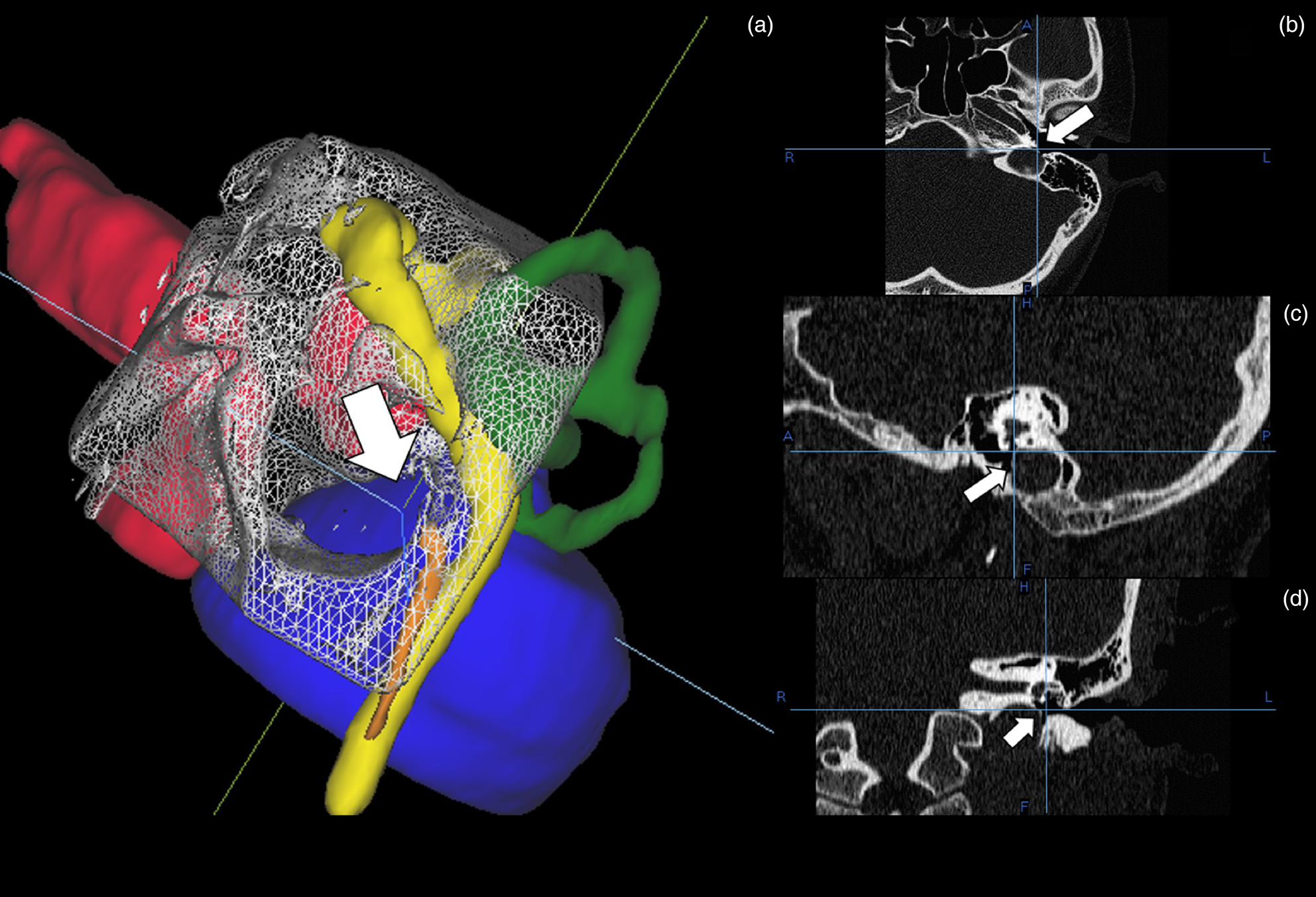
Fig. 4. The three-dimensionally reconstructed images (a) and axial (b), sagittal (c), and coronal (d) plane images of temporal bone computed tomography with a high jugular bulb (arrow). Endoscopic transcanal transpromontorial approach is limited by the high jugular bulb occupying the space (white arrow in a–d) in the middle-ear cavity. A = anterior; R = right; L = left; P = posterior; H = highest; F = floor
In the conventional transcanal transpromontorial approach procedure, the following surgical landmarks limit dissection: the jugular bulb is located inferiorly, the internal carotid artery is located anteriorly, the geniculated ganglion and tympanic segments of the facial nerve lie superiorly, and the mastoid segments of the facial nerve lie posteriorly. After fully exploring the medial wall of the vestibule, this approach allowed identification of an anatomical triangle among the geniculate ganglion superiorly, the basal turn of the cochlea anteriorly and the spherical recess of the internal auditory canal posteroinferiorly. Drilling into this anatomical triangle enabled identification of the intralabyrinthine tract of the facial nerve from the internal auditory canal to the geniculate ganglion, and the anatomical position of the intralabyrinthine facial nerve was noted.Reference Marchioni, Alicandri-Ciufelli, Mattioli, Nogeira, Tarabichi and Villari6
Identification of the labyrinthine segment of the facial nerve among the four nerve segments coming from the internal auditory canal fundus is essential. The directions of the four nerve segments and the bony crest serve as guides because the labyrinthine segment is located superior-anterior to the internal auditory canal and runs toward the geniculate ganglion (point 5).
A radiological study using six radiological points to measure the maximum area of exposure in the transcanal transpromontorial approach using 3D temporal bone reconstructions showed a mean lateral window in the middle ear of 152.9 mm2 and a similar medial window at the internal auditory canal porus of 151.9 mm2.Reference Yacoub, Wimmer, Molinari, Alicandri-Ciufelli, Presutti and Caversaccio7 The six points were applied in this study.
The image transmitted to the monitor through the endoscope is not stereoscopic. The critical structures of the surgical landmarks are located under the medial wall of the middle-ear cavity (Figure 5). Therefore, knowledge of the surgical landmarks is mandatory to preserve the facial nerve.Reference Marchioni, Carner, Rubini, Nogueira, Masotto and Alicandri-Ciufelli8 At each stage of an operation, the surgeon must check for the facial nerve using an endoscope and decide where to drill. If the distance and angle between the structures are known, especially in a narrow space, this will help the surgeon understand and proceed with the surgery.

Fig. 5. Composite and endoscopic images of the three-dimensional reconstruction of the temporal bone computed tomography. The structures of critical surgical landmarks are located underneath the medial wall of the middle-ear cavity. Point 1: the highest level of the jugular bulb; point 2: the posterior wall of the ascending petrous internal auditory canal at the level of the hypotympanum; point 3: the level of the Eustachian tube; point 4: cochlear apex; point 5: facial nerve at the centre of the geniculate ganglion; point 6: centre of the second genu; and point 7: the branch of the chorda tympani nerve.
In the cadaveric study by Presutti et al., an imaginary line passing from the geniculate ganglion to the spherical recess just above the apical turn of the cochlea indicated the facial nerve route through the inner ear.Reference Presutti, Bonali, Marchioni, Pavesi, Feletti and Anschuetz9 We obtained similar results in this study. The value of aPfOR (101.81 ± 8.86°) was between those of aP4OR (77.32 ± 6.31°) and aP5OR (111.77 ± 7.87°) but closer to aP5OR, which is similar to the imaginary line reported by Presutti et al.Reference Savic and Djeric10 The distances dPfR and dPfO were 6.18 ± 0.34 and 5.30 ± 0.41 mm, respectively (Table 1).
The internal carotid artery and jugular bulb are the two largest blood vessels neighbouring the middle-ear cavity. As the internal carotid artery travels through the petrous bone, it first passes the middle-ear cavity and cochlea anteriorly and then bends to run medially to the Eustachian tube.
An aberrant high jugular bulb is characterised by a high-positioned jugular fossa, either medial or lateral to the cochlea. Histopathological studies show an estimated 25 per cent incidence of a high jugular bulb protruding into the tympanic cavity in the temporal bone.Reference Savic and Djeric10 Therefore, pre-operative assessment of the vascular structures within the temporal bone is of prime importance.Reference Wang, Shi, Liu, Wang, Huang and Chen11 In this study, P1–P3 were localised to the vascular structure. In particular, the standard deviation of the dP1O and dP1R values, which are the distances from the oval window and round window to the jugular bulb, were larger than the distances to P2 and P3 (Table 1).
The point P3 could be identified by drilling underneath the Eustachian tube, and P5 could be traced using the cochleariform process during surgery because the cochleariform process is also positioned just inferolateral to the geniculate ganglion.Reference Komune, Matsuo, Miki and Rhoton1 The cochlear apex (P4) traces along the modiolus and could be identified between P3 and P5. The distance and angle to P4 based on the oval window and round window could be affected by various cochlear morphologies.Reference Erixon, Högstorp, Wadin and Rask-Andersen12
Removing the triangular bone landmark exposes the dura lining the internal acoustic canal. Opening the dura of the internal acoustic canal exposes the facial, cochlear, and superior and inferior vestibular nerves. The upper portion of the middle turn of the cochlea serves as a landmark for the labyrinthine part of the facial nerve (Pf) because it is located just superior to the middle turn of the cochlea.Reference Komune, Matsuo, Miki and Rhoton1
• The transcanal transpromontorial approach is minimally invasive, but the surgical field through the ear canal is limited
• Distances and angles to critical radiological points of the temporal bone were measured from the oval window and round window to provide a three-dimensional (3D) image
• The facial nerve from the internal auditory canal to labyrinthine segment could be traced between the angle to the cochlear apex and the geniculate ganglion
• A 3D reconstruction of pre-operative computed tomography scans will further knowledge of inner structures of temporal bone
• This reconstruction can also help identify surgical landmarks for the transcanal transpromontorial approach
The expanded transcanal transpromontorial approach is a combined microscopic and endoscopic technique proposed for large vestibular schwannomas up to 3 cm in diameter.Reference Marchioni, Carner, Soloperto, Bianconi, Sacchetto and Sacchetto2 In the expanded transcanal transpromontorial approach, the mastoid segment of the facial nerve becomes the boundary for surgery, marking the related P6 and P7 surgical indicators. The facial nerve gives rise to the chorda tympani in the vertical mastoid segment, which lies near the lower margin of the bony tympanic ring and 4–5 mm proximal to the stylomastoid foramen. However, this branching point is variable.Reference McManus, Dawes and Stringer13
Radiological evaluation is less accurate than microscopic anatomical studies by cadaver dissection of the temporal bone structures. Moreover, the anatomical landmarks found in actual surgery are more critical. Nevertheless, the advantage of an imaging study is that it can be performed pre-operatively for patients in order to customise their surgery.
In this study, the measured distance to the centre point of the oval window and round window was 2.65 ± 0.36 mm. This value is similar to that of 2.02 ± 0.56 mm from the study by Shraddha et al., considering that it was measured with the shortest distance between the edge of the oval window and round window in cadaver studies.Reference Shraddha, Gaurkar, Deshmukh, Khatri, Kalambe and Lakhotia14 In this study, to increase the accuracy of the designation of this position on 3D reconstructed images, a 3D cursor was activated on the axial, sagittal and coronal plane images. Despite the limitations of this imaging study, it has the advantage of 3D confirmation to check the location of important structures and prepare surgeons for any likely problems they may encounter during surgery.
Conclusion
This study furthers our knowledge of important surgical landmarks and helps distinguish the facial nerve from the internal auditory canal during the transcanal transpromontorial approach using 3D reconstruction of pre-operative CT scans. It can also assist surgeons in selecting appropriate candidates for the transcanal transpromontorial approach and tailoring the treatment approaches used.
Competing interests
None declared.







