


Introduction
Osteomas are benign, slow-growing tumours originating from bone tissue. Although they may be seen in all age groups, they are more frequent in males aged between 40–50 years.Reference Molher, Pujol, Zounon, Darrouzet and Bonnard1,Reference Abouzayd and Seghir2 Middle-ear osteomas are usually asymptomatic and are detected incidentally on tomography scans performed for other medical reasons.Reference Silver, Orobello, Mangal and Pensak3
Temporal bone osteomas are mostly localised in the external auditory canal. Middle-ear osteomas are very rare and may present with various clinical findings including conductive or mixed hearing loss, facial nerve dysfunction, vertigo and otitis media according to the site of involvement in the temporal bone.Reference Curtis, Bance, Carter and Hong4 Herein, the author reports a very rare case of osteoma of the promontory that mimicked otosclerosis, causing progressive conductive hearing loss and tinnitus by limiting stapes mobility, which is an uncommon condition.
Case report
A 21-year-old man presented with a 4-year history of progressive conductive hearing loss in his right ear. The patient had no remarkable history of chronic ear disease of his affected ear including ear discharge, ventilation tube insertion or surgical intervention. The patient also denied familial hearing loss, chronic noise exposure and trauma. The patient's only complaint was progressive hearing loss with intermittent tinnitus of recent onset.
Otoscopic examination showed an intact tympanic membrane with normal appearance in both ears. Other otorhinolaryngological examination findings were unremarkable. Pure tone audiometry values at frequencies of 0.5, 1, 2 and 4 kHz showed conductive hearing loss in the right ear (47 dB with a 30-dB air–bone gap), and tympanometry showed a type A tympanogram for the affected ear. Furthermore, Carhart's notch, suggesting otosclerosis, was observed (Figure 1). However, an ipsilateral stapedial reflex was obtained. The Weber test was performed and lateralised towards the affected ear. A history of the patient, audiological evaluation and otoscopic examination suggested otosclerosis. On the other hand, temporal bone high-resolution computed tomography (CT) scans showed a hyperdense 4 × 3.5 mm mass with bone density (1365 Hounsfield units) located on the promontory with impingement on the stapes (Figure 2). High-resolution CT findings resembled osteoma of the promontory. Because superior semicircular canal dehiscence syndrome may also lead to conductive hearing loss with intact stapedial reflex, high-resolution CT images were also examined for superior semicircular canal integrity, and no radiological evidence of dehiscence was observed.
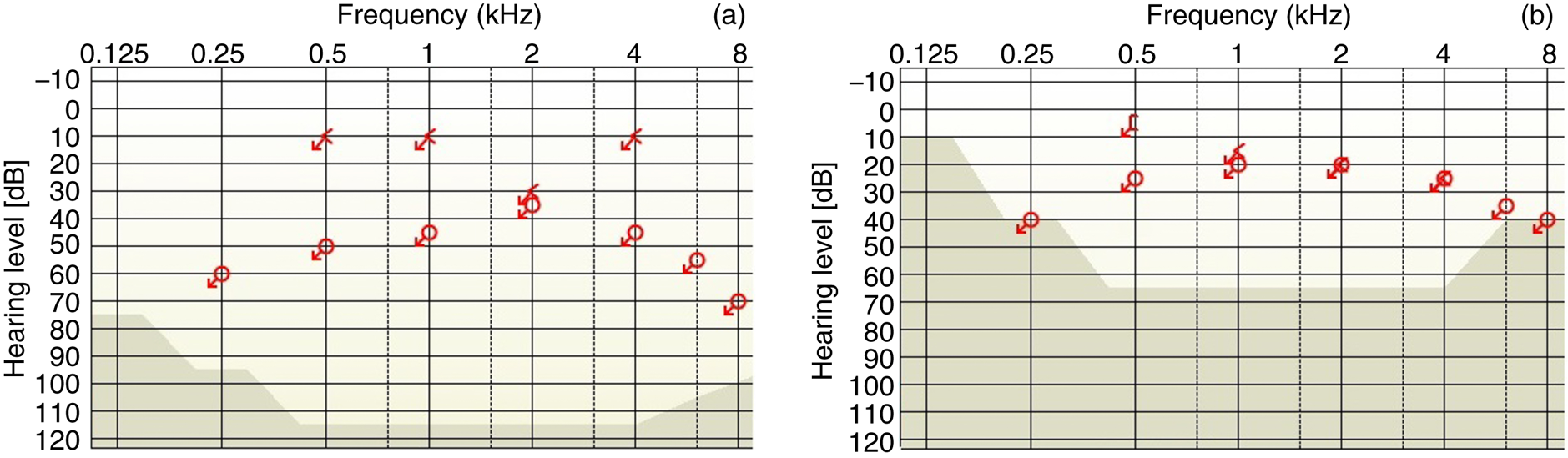
Fig. 1. Graphs showing: (a) pre-operative pure tone audiometry result of the right ear, 47 dB air-conduction threshold with 30 dB air–bone gap and Carhart's notch at a frequency of 2 kHz; (b) pure tone audiometry result of the right ear after removal of the middle-ear osteoma, 23 dB air-conduction threshold with a 5 dB air–bone gap.
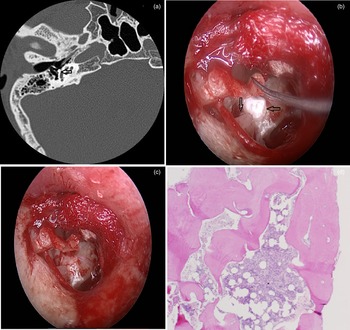
Fig. 2. Photographs showing: (a) temporal bone high-resolution computed tomography view of the promontory osteoma (left arrow); (b) intra-operative view of the promontory osteoma with the vertical arrow showing an osteoma impinging on the anterior crus of the stapes and the horizontal arrow showing the osteoma; (c) endoscopic view of the middle ear after meticulous removal of the osteoma; and (d) haematoxylin and eosin stained specimen showing fragments of lamellar bone and normal bone tissue. (H&E; ×200)
Endoscopic transcanal middle-ear exploration showed that an osteoma located on the promontory was restricting the mobility of the stapes by affecting the anterior crus of the stapes (Figure 2). No involvement of adjacent middle-ear structures such as the stapes, footplate, facial nerve and round window was observed. Stapes mobility was ensured after meticulous resection of the osteoma using both a curette and diamond drill via a transcanal endoscopic approach. Histopathological examination of the specimen showed normal bone tissue structures surrounded by fragments of lamellar bone, which is diagnostic for osteoma. The post-operative course was uneventful. In the first post-operative month, pure tone audiometry improved to 23 dB with a 5-dB air–bone gap (Figure 1), and tinnitus resolved spontaneously without any additional treatment.
Discussion
Osteomas of the temporal bone are infrequent, slow-growing, benign tumours that are commonly observed in the external ear canal. However, middle-ear osteomas, usually asymptomatic and incidentally detected, are an extremely rare entity. Osteomas of the temporal bone occur predominantly in males and younger patients, as in our case.Reference Molher, Pujol, Zounon, Darrouzet and Bonnard1 Although the aetiology of osteomas still remains unclear, genetic factors, embryological developmental disorders and chronic inflammation have also been proposed to play a role in osteoma formation.Reference Abouzayd and Seghir2 Middle-ear osteomas usually occur in patients with no previous history of ear surgery or trauma, with normal otoscopy findings, and are incidentally diagnosed in patients without any symptoms.Reference Silver, Orobello, Mangal and Pensak3 Osteomas of the middle ear present symptoms according to their involvement site when they reach a certain size. Curtis et al. reported a case of middle-ear osteoma that caused House–Brackmann grade IV facial nerve dysfunction that improved to House–Brackmann facial nerve dysfunction grade II after surgery.Reference Curtis, Bance, Carter and Hong4 Conductive or mixed hearing loss is the most frequently presented symptom of middle-ear osteomas.Reference Molher, Pujol, Zounon, Darrouzet and Bonnard1,Reference Yuan, Chen, Jiang and Zhang5
In most cases, osteoma diagnosis is established according to high-resolution CT findings. Histopathological confirmation is possible by examining the specimen intra-operatively in symptomatic cases. The classic histopathological view of osteomas contains few osteocytes or lacunae and includes an excess of fibrovascular channels covered by lamellar bone tissue.Reference Yoon, Yoon and Lee6 Temporal bone high-resolution CT is the preferred radio-diagnostic modality in the diagnosis of middle-ear osteomas.Reference Silver, Orobello, Mangal and Pensak3 Moreover, high-resolution CT is very helpful in detecting the localisation and boundaries of tumours and identifying whether or not there is ossicle or facial nerve involvement. Surgical approach and ossiculoplasty techniques may be planned pre-operatively according to high-resolution CT findings.Reference Curtis, Bance, Carter and Hong4
Because middle-ear osteomas exhibit an extremely low growth rate, surgery is not recommended in asymptomatic cases. Follow-up with otoscopic examination and temporal bone high-resolution CT scans is recommended in asymptomatic patients.Reference Silver, Orobello, Mangal and Pensak3 Surgery is indicated when findings associated with middle-ear osteoma become symptomatic. On the other hand, Yoon et al. advocated that surgical treatment of the asymptomatic middle-ear osteomas incidentally detected on CT scans should be performed due to potential complications later in life, including facial nerve paralysis, sensorineural hearing loss and vertigo.Reference Yoon, Yoon and Lee6
So far, to the best of the author's knowledge, only two cases of middle-ear osteoma involving the stapes have been reported. Yuan et al. reported a case of middle-ear osteoma originating from the stapes that caused conductive hearing loss. They reported that the air–bone gap improved after ossiculoplasty using titanium prosthesis following the removal of the osteoma with stapes.Reference Yuan, Chen, Jiang and Zhang5 Vérillaud et al. reported a conductive hearing loss due to middle-ear osteoma involving the stapes and incus that improved post-operatively.Reference Vérillaud, Guilleré, Williams, El Bakkouri and Ayache7 In this study, it was fortunate that the osteoma that was only limiting stapes mobility had originated from the promontory and was not invading the stapes or other middle-ear structures. Therefore, the meticulous removal of the osteoma arising from promontory without performing ossiculoplasty was sufficient in the treatment of conductive hearing loss in this case.
• Osteomas of the middle ear are usually diagnosed incidentally, are infrequent and rarely become symptomatic
• Symptoms associated with middle-ear osteomas include conductive or mixed hearing loss, vertigo and facial paralysis depending on their specific location, size and involvement site
• Surgery is indicated when findings associated with middle-ear osteoma become symptomatic
Conclusion
In conclusion, although middle-ear osteomas are a rare entity and usually asymptomatic, differential diagnosis should be considered for patients with progressive conductive hearing loss and tinnitus with intact stapedial reflexes and normal otoscopic findings.
Competing interests
None declared


