Introduction
Acute mastoiditis, an acute inflammatory disease of the mastoid process,Reference Gross, McMenomey, Glasscock and Gulya 1 represents the most frequent intra-temporal complication of acute otitis media, with an estimated incidence of 1.2–4.2 per 100 000 person years among children in developed countries.Reference Van Zuijlen, Schilder, Van Balen and Hoes 2 Mastoid involvement is expected in most cases of acute otitis media, as mastoid air cells form part of the middle-ear cleft; however, acute mastoiditis becomes clinically significant if it spreads through the periosteum and induces periostitis or bone destruction (acute coalescent mastoiditis).Reference Dudkiewicz, Livni, Kornreich, Nageris, Ulanovski and Raveh 3 The clinical and radiological differentiation between the stages of mastoid involvement (mucosal inflammation, periostitis, osteomyelitis) can be difficult if there is no previous imaging.
Different textbooksReference Wald, Conway, Long, Pickering and Prober 4 – Reference Kerschner, Kliegman, Stanton, St Geme, Schor and Behrman 6 argue that osteal involvement indicates the need for prolonged antimicrobial treatment of three to six weeks’ duration, without any reference to evidence-based data. Two recently published studiesReference Van den Aardweg, Rovers, de Ru, Albers and Schilder 7 , Reference Psarommatis, Voudouris, Douros, Giannakopoulos, Bairamis and Carabinos 8 demonstrated a lack of consensus regarding diagnostic criteria and management of paediatric acute mastoiditis.
The current study aimed to evaluate acute mastoiditis treatment at our medical centre, focusing on the duration of antimicrobial therapy and its short- and long-term sequelae.
Materials and methods
A retrospective review of all acute mastoiditis patients (International Classification of Diseases, ninth revision, code 383) admitted to the Children's Hospital at Westmead, Sydney, from 1 July 2003 to 30 June 2012, was conducted. There were a total of 101 cases.
Acute mastoiditis was diagnosed using the following clinical criteria: signs of acute otitis media on otoscopy and local inflammatory findings over the mastoid process (including pain, redness, local sensitivity and/or protrusion of the auricle), or local inflammatory findings over the mastoid process and imaging or surgical findings of mastoiditis (with no signs of acute otitis media).Reference Luntz, Brodsky, Nusem, Kronenberg, Keren and Migirov 9 Imaging findings of mastoiditis were defined as the presence of increased attenuation of the mastoid cells on computed tomography (CT) or magnetic resonance imaging (MRI) scans, with or without osseous resorption or periostitis.Reference Vazquez, Castellote, Piqueras, Mauleon, Creixell and Pumarola 10
In total, 88 cases met the diagnostic criteria and were included in the final statistical analysis. Demographic, historical, clinical, laboratory and bacterial culture data were collected for all patients.
The months April to September were considered winter (in the southern hemisphere), while October to March were considered summer.
The cases were examined in terms of: antibiotics used, surgical treatment modality, complications, and short- and long-term sequelae. Complications can be intracranial or extracranial, and a list is provided in Table I. Short-term and long-term sequelae that concerned the treating team included: non-resolving ear ache or ear discharge, persistent high fevers, evidence of disequilibrium, persistent tympanic membrane perforation, recurrent acute otitis media and otitis media with effusion, recurrent acute mastoiditis, diagnosis of cholesteatoma, the need for subsequent grommet insertion, and requirement for an adenoidectomy. To be included in the ‘short-term sequelae’ analysis, a minimum follow-up period of 14 days after completion of the oral antibiotic therapy immediately following hospital discharge was necessary. As for ‘long-term sequelae’ analysis, the minimum follow-up period necessary was four months after discharge or prior evidence of long-term sequelae.
Table I Intracranial and extracranial complications

*One patient had three different extracranial complications. †Three patients had two different intracranial complications.
The student's t-test and chi-square test were employed (using JMP statistical software, version 10.1; SAS Institute, Cary, North Carolina, USA) to compare independent variables between groups prescribed with antibiotics for either 10 days or fewer or more than 10 days. A p value of less than 0.05 was considered to be statistically significant. The present study was approved by the Children's Hospital at Westmead Institutional Review Board.
Results
Of the 101 cases reviewed, 88 were found to meet the inclusion criteria. Median age at time of acute mastoiditis diagnosis was 22 months (range, 3–150 months; standard deviation (SD) = 35.36); 52 patients (59 per cent) were boys.
Only 11 children (12.5 per cent) had relevant positive past medical history: recurrent acute otitis media, in 7 children; previous grommet insertion, in 2; gastroesophageal reflux disease, in 2; ipsilateral cholesteatoma, in 1; severe combined immunodeficiency, in 1; and chronic lung disease, in 1.
Admission date distribution according to calendric month is shown in Figure 1. Fifty-two patients were admitted during the winter months. Median hospitalisation duration was 5 days (range, 2–26 days; SD = 3.42). All patients were managed as in-patients for the initial treatment.

Fig. 1 Admission date distribution according to calendric month.
Acute mastoiditis was bilateral in 1 case (1 per cent), right-sided in 49 cases (56 per cent) and left-sided in 38 cases (43 per cent). Pre-admission signs and symptoms were present from 1 to 30 days (median = 4 days; SD = 5.06); these signs and symptoms are listed in Table II.
Table II Pre-admission signs and symptoms

*Calculated from patients with available data for analysis. †Median = 38.8 °C; range = 37.9–40.7 °C; standard deviation = 0.71.
Forty-eight out of 86 patients (56 per cent) received systemic antibiotic treatment prior to admission at the Children's Hospital at Westmead. Data regarding the specific antibiotic agents used were available in only 46 cases; generally, the treatment comprised a form of penicillin and/or cephalosporin (45 out of 46 cases) (Table III).

Results of the auditory canal swab cultures taken at the time of admission were available in 26 cases (Table IV). The swabs were taken in all patients with acute otitis media and tympanic membrane perforation.
Table IV Microbial culture results*

Data represent numbers of cases.
* Of swabs from the external auditory canal, or tympanic or mastoid cavities, on admission and during surgery. †Total n = 26 (1 patient's culture showed growth of 2 different organisms); ‡total n = 37.
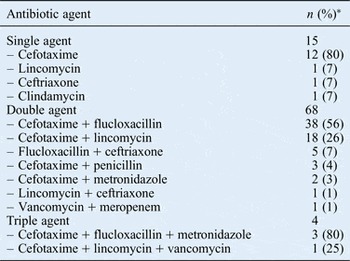
All patients were treated with intravenous (IV) antibiotics throughout their admission period (Table V). Temporal bone and brain CT or MRI scans were obtained for 42 and 3 patients respectively. Extracranial complications occurred solely in 34 patients, while 8 patients had solely intracranial complications. Six patients had both intracranial and extracranial complications (Table I).
Table V In-patient intravenous antibiotic treatment

*One patient was treated with an intravenous antibiotic of an unknown type.
A total of 42 patients underwent some form of surgical procedure(s) (Figure 2). Indications for the surgical procedures included: evidence of either intracranial or extracranial complications (n = 31); no clinical improvement within 48–72 hours of commencing IV antibiotics (n = 10); and evidence of recurrent acute otitis media (n = 3).

Fig. 2 Surgical procedures among 43 patients.
The first two aforementioned indications were the reason for surgery in two patients, while one patient was operated on because of recurrent acute otitis media and suspected cholesteatoma. One patient underwent multiple procedures on different days: an initial ventilation tube insertion and post-auricular drainage procedure was needed on admission, but a cortical mastoidectomy was required 3 days later because of a recurrent post-auricular subperiosteal abscess.
Positive microbial cultures results at the time of surgery (in 15 out of 37 cases, 40 per cent) invariably grew a streptococcal species, while a significant number had no microbial growth (Table IV).
Sufficient data regarding the type and duration of antibiotic therapy administered during and after admission were available for 78 patients (Table VI). ‘Post-discharge’ refers to the time period immediately after leaving the hospital, when care is continued in the home environment. The median period of post-discharge antibiotic therapy was 10 days (range, 5–49 days; SD = 7.46). The median follow-up period post-discharge was 52 days (range, 0–2350 days; SD = 439).
Table VI Post-discharge oral antibiotic treatment

*Five patients were treated with two different antibiotic agents. †Given intravenously.
Fifty-two and 40 patients met the inclusion criteria for short- and long-term sequelae analysis, respectively. There were no deaths in this series. No short-term sequelae were reported among the 52 patients analysed. Fourteen of the 40 patients evaluated (35 per cent) had documented long-term sequelae (Table VII). Only one patient had recurrent acute mastoiditis, which occurred 25 days after completion of a 13-day course of antibiotic therapy for her first episode of acute mastoiditis. No organism was isolated for either episode. The treatment for the first episode included 1 day of oral amoxicillin and clavulanate pre-admission, 5 days of IV cefotaxime and lincomycin, and 7 more days of amoxicillin and clavulanate post-discharge.
Table VII Long-term sequelae

*Five patients had more than one long-term sequela.
The seasonality effect on surgery, complication rate, and duration of hospitalisation and antibiotic therapy is presented in Table VIII. Only hospitalisation duration was found to be significantly longer during the winter period.
Table VIII Seasonality effect on surgery, complication rate, and duration of hospitalisation and antibiotic treatment*

* ‘Winter’ refers to the months of April to August and ‘summer’ represents the months of September to March. †Indicates significance (p < 0.05). ‡The sum days of pre-admission, admission and post-admission antibiotic therapy. SD = standard deviation
No significant difference was found in terms of the total antibiotic therapy time (the sum of pre-admission, admission and post-admission antibiotic therapy durations) or the complication rate in different age groups (Table IX).
Table IX Total antibiotic treatment duration and complication rate in different age groups

*The sum days of pre-admission, admission and post-admission antibiotic therapy. SD = standard deviation
The incidence and relative risk for complications according to the pre-admission culture result are shown in Table X. Twenty-five out of 48 patients (52 per cent) who received pre-admission antibiotic therapy were diagnosed with complications. However, only 10 out of 37 patients (27 per cent) who did not receive pre-admission antibiotic therapy were diagnosed with complications. This finding was statistically significant (p = 0.01).
Table X Pre-admission cultures and complication incidence

Data represent number of patients unless indicated otherwise. *Extracranial or intracranial complication. †Relative complication risk as compared to the overall complication rate – 36 of 88 (41 per cent). RR = relative risk
Discussion
This review of the demographic, historical, clinical and laboratory findings in 88 acute mastoiditis patients, who presented over a 9-year period at a tertiary paediatric medical centre where patient management is carried out by different specialty disciplines (i.e. otolaryngologists, paediatricians and infectious disease specialists), at both junior and senior levels, informs as to how one might approach acute mastoiditis. It is generally agreed that appropriate oral antibiotic therapy immediately following hospital discharge is essential for the prevention of residual and recurrent infection. However, an inappropriately short course of antibiotic therapy may allow disease recurrence or persistence, while prolonged antibiotic therapy may produce unnecessary side effects such as diarrhoea, mycotic infection and microbial resistance. Physicians from different medical fields rely on low-level evidence and common practice to determine this form of therapy;Reference Wald, Conway, Long, Pickering and Prober 4 – Reference Kerschner, Kliegman, Stanton, St Geme, Schor and Behrman 6 this study attempted to address this issue in an evidence-based manner.
Our study population had similar characteristics to acute mastoiditis cohorts in other published studies in terms of age range and distribution,Reference Psarommatis, Voudouris, Douros, Giannakopoulos, Bairamis and Carabinos 8 , Reference Luntz, Brodsky, Nusem, Kronenberg, Keren and Migirov 9 , Reference Groth, Enoksson, Hultcrantz, Stalfors, Stenfeldt and Hermansson 11 pre-admission signs and symptoms,Reference Psarommatis, Voudouris, Douros, Giannakopoulos, Bairamis and Carabinos 8 , Reference Luntz, Brodsky, Nusem, Kronenberg, Keren and Migirov 9 , Reference Groth, Enoksson, Hultcrantz, Stalfors, Stenfeldt and Hermansson 11 and the isolated pathogen.Reference Luntz, Brodsky, Nusem, Kronenberg, Keren and Migirov 9 , Reference Groth, Enoksson, Hultcrantz, Stalfors, Stenfeldt and Hermansson 11 , Reference Bakhos, Trijolet, Morinière, Pondaven, Al Zahrani and Lescanne 12 Nevertheless, other studies showed a peak incidence of acute mastoiditis in the second year of life, while this study found a peak incidence between 6 and 12 months of age.Reference Groth, Enoksson, Hultcrantz, Stalfors, Stenfeldt and Hermansson 11 , Reference Migirov, Yakirevitch and Kronenberg 13 In addition, this study did not show any increases in antibiotic therapy duration and complication rate with age, which is in line with the findings of Groth et al.Reference Groth, Enoksson, Hultcrantz, Stalfors, Stenfeldt and Hermansson 11
In terms of seasonality, our findings, in accordance with published data,Reference Psarommatis, Voudouris, Douros, Giannakopoulos, Bairamis and Carabinos 8 demonstrated a spike in acute mastoiditis incidence during late winter and early spring. This spike in incidence matches the peak incidence of viral upper respiratory tract infections in mid-winter among young children. Hospitalisation duration was found to be significantly longer during winter. Nevertheless, surgery rate, complication rate and total antibiotic therapy duration were not increased during winter months, which indicates that the prolonged hospitalisation during winter was not attributed to a more severe condition.
Post-discharge oral antibiotic therapy was chosen as the primary covariate for evaluation because of the heterogeneity of the patients reviewed. All patients had been treated with IV antibiotics throughout their admission. Admission duration is determined not only by patient factors (including signs and symptoms, complications, and surgical findings), but also by consultant preferences, concerns and institutional guidelines. We feel it is reasonable to assume that all patients, regardless of the length and type of treatment given while an in-patient, should be discharged from hospital in a similar state: this includes being afebrile, being able to swallow oral antibiotics and having no clinical evidence of abscess collection necessitating further drainage. Persistent acute mastoiditis was defined as the diagnosis of acute mastoiditis within two weeks following the completion of antibiotic therapy. Only a single patient in the cohort studied had recurrent (rather than persistent) acute mastoiditis, 26 days after completing 5 days of IV antibiotic therapy and a subsequent 7 days of oral antibiotic therapy. As no patient in the current study had persistent acute mastoiditis, a comprehensive statistical analysis to determine the optimal regimen of post-discharge oral antibiotic therapy could not be undertaken. Nevertheless, the authors feel that 10 days of post-discharge oral antibiotic therapy, which represents the median duration in the current study, is a safe and reasonable baseline guideline.
The microbial characteristics of the organisms treated in this study indicate that streptococcus was the commonest organism grown, and this is reflected by the type of antibiotic therapy prescribed during the patients’ admission. However, complicated cases of acute mastoiditis, such as patients with intracranial and extracranial complications, and patients who are immunosuppressed or infected with bacteria of increased resistance, need to be assessed individually and considered for a more aggressive treatment regimen. This is reflected in the frequent use of multiple forms of antibiotic therapy, with four of our cases requiring triple-mode therapy. A similar approach was used by Psarommatis et al., wherein 167 children with acute mastoiditis were given post-discharge oral antibiotic therapy for 7–10 days, while children with intracranial complications received 15 or more days of such therapy.Reference Psarommatis, Voudouris, Douros, Giannakopoulos, Bairamis and Carabinos 8
One-third of the children in the present study (35 per cent) had long-term sequelae. The most prevalent clinical sequelae were recurrent otorrhoea and recurrent acute otitis media, while the most prevalent surgical sequela was the requirement for subsequent ventilation tube insertion. Although the aforementioned sequelae were in the 10–15 per cent range, which is comparable to the observations of Glynn et al.,Reference Glynn, Osman, Colreavy, Rowley, Dwyer and Blayney 14 these findings highlight that the vast majority of mastoiditis processes are acute and sporadic in nature, rather than recurrent or chronic.
We found that patients with negative growth on pre-admission microbial cultures were at a higher risk for complications. Pre-admission antibiotic therapy is associated with negative growth on pre-admission microbial culture.Reference Bartolomé Benito and Pérez Gorricho 15 Further analysis demonstrated that pre-admission antibiotic therapy was associated with a statistically significant higher complication rate in patients with acute mastoiditis. This finding may be the result of inclusion bias: this study only included patients who did not improve with antibiotic therapy and were thus referred to our tertiary medical centre, making them already prone to developing complications. From the point of view of an admitting medical officer in a tertiary medical centre, this indicates that a patient with acute mastoiditis treated with antibiotics prior to admission might be suitable for more proactive management such as early imaging and surgical intervention, rather than a conservative approach.
-
• Acute mastoiditis is the most common acute otitis media intra-temporal complication
-
• There is a lack of consensus and insufficient evidence-based data regarding appropriate antibiotic management of paediatric acute mastoiditis
-
• Children with acute mastoiditis treated with antibiotics prior to admission are at higher risk of complications
-
• Oral antibiotic treatment is recommended for 10 days after hospital discharge in all uncomplicated acute mastoiditis cases
Overall, the current study represents an initial approach towards determining the optimal antibiotic management of acute mastoiditis. Further studies, whether they are prospective, controlled and double-blinded, or follow outcome research methodology, are needed to examine this heterogeneous group of individuals.
Conclusion
Patients with acute mastoiditis who receive pre-admission antibiotic therapy may require more proactive management (early imaging and surgical intervention), rather than conservative therapies alone. It is recommended that oral antibiotic therapy is given for 10 days following hospital discharge in all uncomplicated cases of treated acute mastoiditis. There is no evidence to suggest that prolonged hospitalisation is necessary to successfully treat acute mastoiditis, whether it be during the summer or winter months.