


Introduction
What would human civilisation be like if there were no singing? It is highly likely that without the development of human singing there would have been no development of music or culture. The singer inspires not only through the content of their song but more dramatically through the character and emotion of their voice. Singing is a complex and difficult task which frequently requires years of training to achieve the highest levels of performance. The audience takes this sacrifice for granted, and will only recognise the risks of vocal injury or difficulty when the singer cannot perform. The care of these performers requires an understanding of the multiple physiological systems which interact to enable maximal presentation of voice. The layered structure of the vocal fold is unique among animals and confers the vibratory characteristics of the human larynx, enabling the volume to shout, the flexibility to sing an aria, and the vocal subtlety to sing a soft, soothing lullaby to an infant.
When the voice begins to fail, and particularly when there is a change in the voice of a singer, the clinician's approach to patient care may require more intensity, compared with other patients whose quality of voice is not critical to their profession. This paper will briefly describe the anatomy and physiology of the voice, with attention to factors that are particularly important to singers. The paper will also describe the evaluation and treatment of the singer, and the importance of the voice care team.
Laryngeal anatomy and physiology
The production of the human voice can be related to the production of sound from any musical instrument. Musical instruments have three major components: something that activates the sound (e.g. plucking a string or striking a piano key); a vibrator to produce the desired frequencies (e.g. the string of a violin or the reed of a wind instrument); and a resonator (i.e. the body of the instrument, which gives each instrument its unique sound). When the human voice is produced, the lungs serve as the activator of the sound, the vocal folds vibrate to produce the desired frequencies, and the resonating cavities of the pharynx, oral cavity, nose, sinuses and chest modify or amplify the sounds. Unlike other music instruments, however, the vocal instrument is always with the performer and is greatly affected by other body systems; therefore, singing is much more complex than just the above three key components. Voice production, and particularly singing, involves interaction of the vocal tract, the abdomen and diaphragm, the musculoskeletal system, and the psychoneurological system. Each of these systems needs to function in a coordinated fashion to produce the singing voice.
The vocal folds are the structures that produce the fundamental frequencies for voice production. The vocal folds themselves are quite small (1.5 to 2.3 mm in length), and there are 22 muscles which interact in a coordinated and precise fashion to produce the voice. The thyroarytenoid joint is the principle joint allowing each vocal fold to move, and is one of the most complex joints in the body, providing three degrees of rotation: rocking, gliding and rotation. These are adjusted by minute changes in each of the laryngeal muscles. Phonation is the term used to describe voice production in which vocal fold modification determines the frequency, and it is the major determinant of pitch.Reference Benninger1
The large frequency range of the human voice extends beyond those frequencies able to be produced by muscle contracture alone. The viscoelastic properties of the larynx allow maximal control of aerodynamic forces, resulting in rapid vibration in a coordinated fashion. Although the full interaction of aerodynamic forces and muscular tension needed to produce voice is probably more complex than can be described in a simple formula, the model that best describes the vibration of the vocal folds is the myoelastic aerodynamic theory of phonation.Reference Van den Berg2 This theory holds that the vibration of the vocal folds depends upon two components: myoelastic, referring to the muscular contraction and neural control of the vocal folds, and the elastic properties needed for phonation; and aerodynamic, referring to airflow and fluid dynamics and the impact of Bernoulli's principle on these movements.Reference Benninger1, Reference Jiang, Benninger and Murry3
When an individual prepares to produce voice, they inhale by creating negative pressure in the chest, which essentially ‘pulls’ air into the lungs. They then place their vocal folds in a closed position, with a tension which helps to determine the frequency of vocal fold vibration. The more tightly the vocal folds are positioned and the longer they are stretched, the higher the frequency that is produced, in a fashion not dissimilar to tightening a piano or guitar string. As the person exhales, air flows between the vocal folds, setting them in motion. The air pressure in the area below the vocal folds, or subglottic pressure, increases to overcome the tension which holds the vocal folds together, essentially pushing or blowing them apart. As the air passes through the vocal folds, the subglottic pressure drops quickly and the pressure of the muscular tension of the vocal folds becomes greater than the subglottic pressure, allowing the vocal folds to come back together. The stronger the force of airflow, the more rapidly this cycle occurs. As air passes through the narrowed glottis, the reduced pressure creates a Bernoulli effect, drawing the vocal folds together and reducing the subglottic pressure as the air passes through the open larynx.Reference Jiang, Benninger and Murry3 In the very short period of time that the vocal folds are together, the subglottic pressure will again increase, and so the cycle repeats itself. This cycle occurs many times per second, enabling the human larynx to produce vibrations of frequencies ranging from below 100 cycles/second to well over 1000 cycles/second in some individuals.Reference Benninger1 Elite operatic sopranos can produce frequencies well above a high C (i.e. 1046 cycles/second).
There are a number of important factors that determine vocal pitch, and these are particularly important when considering singers' voices. These factors are similar to those affecting other musical instruments. Frequency is affected by the mass and tension of the vocal folds and the level of subglottic pressure. A larger or heavier vocal fold will vibrate more slowly than a smaller or thinner vocal fold. This is not dissimilar to the effect that mass and tension have on the frequency of vibration of a violin or piano string. A woman's vocal fold tends to have less mass than a man's, and this is one of the factors that result in the higher frequencies of the female voice compared with the male voice. This effect also accounts for the lowering in pitch that occurs with mass lesions on the vocal fold. Increasing vocal fold tension has a similar effect: the tighter the muscle contraction, the higher the frequency produced. Lastly, raising the subglottic pressure will increase the rapidity of the cycle described above, elevating pitch.Reference Coulton, Benninger, Jacobson and Johnson4 These principles help to explain the impact of altered vocal fold mass, vocal fold tension and subglottic pressure upon pitch. Vocal pitch will increase with reduced vocal fold mass, increased vocal fold tension and increased subglottic pressure. The opposite is true for decreased pitch, which is related to increased vocal fold mass, decreased vocal fold tension and decreased subglottic pressure.
The microarchitecture of the vocal folds plays a critical role in facilitating the viscoelastic pliability which allows the vocal folds to vibrate in an efficient manner. Stiff vocal folds vibrate less well than pliable vocal folds. This microarchitecture was initially described by Hirano and colleagues in the early 1970s as comprising a layered structure consisting of a body (the thyroarytenoid or vocalis muscle) and a cover (the tissue covering the muscle) (Figure 1).Reference Hirano5–Reference Hirano7 The cover has three layers of lamina propria, the deepest layer being the vocal ligament. Each of these layers has the ability to vibrate independently or as a unit, giving remarkable flexibility to the voice.Reference Benninger1, Reference Hirano7 Coulton has stated that ‘[d]ifferences between modal tone, chest voice phonation or falsetto may be explainable by the coupling or independent movement of these layers’.Reference Jacobson, Johnson, Grywalski, Silbergleit, Jacobson and Benninger1, Reference Coulton, Benninger, Jacobson and Johnson4
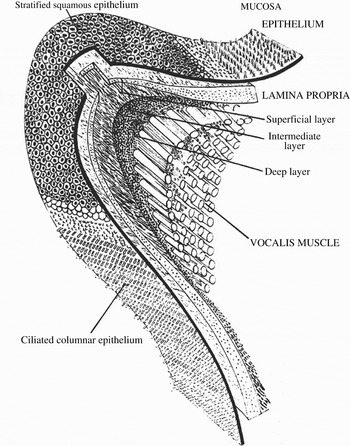
Fig. 1 The layered structure of the human vocal fold, comprising epithelium, three layers of lamina propria and the vocalis muscle. Reprinted with permission.Reference Hirano5
Increasing vocal intensity increases vocal loudness, although increasing loudness does not require a change in frequency. Untrained singers’ attempts to increase vocal intensity or pitch can frequently lead to an unwanted change in pitch. Even contraction of the strap muscles of the neck can lead to pitch changes via alteration of subglottic pressure. Contraction of the thyrohyoid muscle results in elevation of the larynx; if all other things are equal, this should decrease the subglottic pressure, lowering pitch. Alternatively, contraction of the sternohyoid or sternothyroid muscles results in lowering of the larynx, which can increase subglottic pressure and raise pitch.
Although the vocal folds are responsible for the production of the fundamental frequency, the sound that emanates from the vocal folds alone would resemble that of a typical vibrating object, i.e. a buzzing sound. It is the resonating cavities of the upper and lower respiratory tracts which give the voice its unique, rich sound. If a guitar string is strummed in isolation from the body of the guitar, only a buzzing sound will result. The harmonics and partials that give the voice richness are in part produced by the vibration of the tissues of the larynx and pharynx. Most singers use these vibrating characteristics to enhance the quality of the vocal sound they produce. When the length of the upper respiratory vocal tract is shortened, the higher frequency components of the voice are enhanced; increasing the opening at the front of the oral cavity also intensifies higher frequencies. In contrast, if the front of the circumference of the upper vocal tract is widened, the lower frequency components are enhanced.
It has been speculated that the ability of humans to create complex language was secondary to a unique evolutionary change that resulted in the descent of the larynx in the neck.Reference Benninger1, Reference Laitman and Reidenburg8 The lower position of the larynx in the neck frees up a wider pharynx, and this enables the production of certain sounds, including the quantum vowels [a], [i] and [u], which are universal to all human languages but not to other species.Reference Benninger1, Reference Laitman and Reidenburg8, Reference Lieberman, Laitman, Reidenburg and Gannon9 Infants have a higher position of the larynx which allows them to suckle and breath at the same time; the descent of the larynx occurs in humans within the first few years of life (Figure 2). Although other species (including other humanoid and primate species) have similar laryngeal structures to humans, their inability to produce the complex sounds enabled by the resonating structures of the human vocal apparatus may have played a significant role in the development of human language, and was perhaps influential in the extinction of non-Homosapiens humanoid species such as Neanderthals.Reference Benninger1 The other unique aspect of the human voice is the presence of the deep layer of the lamina propria (i.e. the vocal ligament), which other species do not have. The importance of this difference is unclear, but it may enable subtle modifications of pitch.

Fig. 2 The descent of the larynx. The left-hand picture shows the abutting relationship of the soft palate and epiglottis in a child, a configuration common to many animal species. The right-hand picture shows the separation between the soft palate and epiglottis seen in the older child. Published with permission (Jeffrey T Laitman).
The unique evolutionary change that occurred with the descent of the larynx is probably the critical factor in the development of human civilisation. Human language was necessary for humans to organise and develop civilisation, which ultimately led to the development of culture and the arts.Reference Diamond10 The voice was probably the first musical instrument, without which it is very unlikely that other musical instruments would have been created.
Various characteristics of the human voice greatly affect how it is perceived by the listener. The voice should have a pleasing quality, with appropriate loudness and a proper balance between oral and nasal elements. The fundamental frequency and pitch should be appropriate for the age, sex and size of the individual, and there should be inflections of pitch and loudness. The voice should also be consistent with cultural dialects and accents.
Evaluation of the singing voice
It is beyond the scope of this paper to describe the complete evaluation of the singing voice, but there are some common principles that should be considered in such an evaluation. In general, care of the vocalist should take place within the context of a voice care team, which may include otolaryngologists, speech and language (voice) pathologists, phoniatrists, teachers of music and singing, and perhaps voice scientists. This care should be supported by easy access to other medical specialists, to provide supportive medical care and advice on illness prevention and general well-being. The complexity of the voice care team will vary depending on the sophistication of the care provided and the needs of the patient.
The single most important aspect of the evaluation is comprehensive history-taking. Through the history, the clinician can understand the unique aspects of the performer's career and performance schedule. History-taking can reveal the precipitating episode or episodes and the factors that may be associated with the voice problem. The history also reveals aspects of general health, medications and irritants which may affect the performer's symptoms or their overall voice disorder. In most cases, the primary diagnosis can be made from the history alone. Important aspects of the history are: the time and duration of singing practice; the performer's next major performance or recital; and the performer's career goals. These will help to determine the urgency and/or intensity of treatment.
Information can be obtained from the singer either through direct interview or via a questionnaire. Completion of a validated quality of life outcomes instrument may constitute an important part of history-taking, and can provide information about specific symptoms, and also about the performer's impression of the impact of their voice disorder on their quality of life. The most widely utilised such questionnaire is the Voice Handicap Index.Reference Jacobson, Johnson, Grywalski, Silbergleit, Jacobson and Benninger11 This questionnaire has a long history of use, is relatively simple to administer, and is very useful in assessing the impact of the voice disorder and the patient's responsiveness to treatment. Of the newer versions of the Voice Handicap Index, one may be more specific to singers.
Minimal formal evaluation of the voice requires an assessment of pitch, perturbation, airflow and vibration, and an anatomic assessment of the vocal fold structure. Although there are complex devices and equipment to enable more formal evaluation, a satisfactory assessment can be performed using a laryngeal mirror, video stroboscopy (assessing anatomy and vibration) and a piano or pitch pipe (assessing frequency), and by measuring the maximal phonatory time (assessing airflow). Such parameters should be assessed at presentation and before and after any medical or surgical treatment.
Medical and surgical disorders in the singer
Disorders of any of the body's systems can result in voice changes; however, the following discussion will focus on disorders specific to the larynx and vocal folds. The primary reason that vocalists consult a physician is for an acute change in voice, often due to an upper respiratory tract infection. In such cases, there are a number of considerations: the severity of the illness, the quality of the voice, the timing of the next performance, and the vocal demands of the performer and their professional need to perform. All of these factors need to be considered in the context of the physical examination of the vocal folds. Evidence of significantly increased vascularity or swelling should prompt serious consideration of cancelling or delaying a performance, while vocal haemorrhage should prompt a recommendation for complete voice rest (Figure 3). More moderate inflammation can be treated with relative voice rest, antibiotics, anti-inflammatory drugs or oral steroids.

Fig. 3 Laryngoscopic view showing a vocal polyp with prominent vascularity on the left vocal fold, and a small haemorrhage on the right vocal fold.
More sustained vocal problems may be associated with functional problems, errors in singing technique, or the amount or intensity of voice training or performance. These problems can be managed by voice pathologists, phoniatricians and singing teachers. Careful consideration of the various aspects of voice use and technique will guide treatment.
Some patients will have more substantial problems with the architecture of the vocal folds, including vocal masses or lesions. Classical examples are vocal nodules, most vocal fold polyps and some vocal cysts (particularly mucous retention cysts or pseudocysts). Fortunately, these lesions are almost always confined to the epithelium and the superficial layer of the lamina propria. Injury or surgery confined to the epithelium or superficial layer of the lamina propria will heal with essentially no impact on vocal fold function, since the fibres of the lamina propria will re-establish in an orientation parallel to the epithelium.Reference Benninger, Alessi, Archer, Bastian, Ford and Koufman12 However, when injury or surgery involves both the epithelium and the deep layer of the lamina propria, a scar can develop perpendicular to the epithelium, resulting in stiffness and reduction of the vocal wave.Reference Benninger, Alessi, Archer, Bastian, Ford and Koufman12 This can result in dramatic, and at times permanent, vocal changes. Vocal nodules are particularly worrisome to performers, and assurance that these rarely result in long term disability will help to focus the patient on recovery. Vocal nodules should respond well to voice therapy and vocal health and behavioural modifications, and rarely require surgery. With changes in the intensity, quantity and/or technique of voice use, recovery can be expected.Reference Benninger and Jacobson13
Communicating with the performer
It is important to realise that performers and healthcare workers have different vocabularies. In addition, it is incumbent upon the voice care team to achieve a level of comfort when communicating with the performer. This is facilitated by providing care in an environment that is reassuring to the performer. Having a clinical environment where literature and art consistent with the interests of the performer are displayed will help them to feel comfortable. Understanding the performer's terminology and/or being familiar with their repertoire or performance schedule will further reassure them that they are being treated by a voice care team that will meet their needs and expectations. It is important to realise that singers often have multiple concerns, ranging from their ability to deliver their next performance safely and with good vocal quality, through to how their vocal problem may affect their voice and career in the long term. It is essential that the clinician understand the performer's issues, in order to care for them effectively and to obtain the best results.
An important aspect of communication with a performer is a careful discussion of the expected benefits and risks of any intervention. This is particularly true when surgery is being considered. The risks should be presented thoroughly, but not in such a way as to frighten the singer. The benefits should be presented honestly and not overstated. The clinician should be well aware of the need for confidentiality regarding all communication related to the patient. This is particularly true for high-level performers; in such cases, the singer's agent, the theatre or venue promoter, and the press may want to know details of the singer's voice problem and its likely impact on upcoming performances. The singer should determine which forms of communications between doctor and patient are acceptable, and it is best that this decision is confirmed in writing. All care should be well documented in the medical chart. With caution and appropriate communication, the appropriate level of documentation and confidentiality can be obtained.
Conclusion
The care of the singer requires an in-depth understanding of the anatomy of the voice and the intricate physiological principles that result in elite voice production. A clinical focus on voice disorders, together with a solid multidisciplinary voice care team, will facilitate evaluation and diagnosis and help maximise treatment outcomes. A careful history and physical examination is essential in order to identify each singer's unique issues, and will help to clarify the intensity and urgency of treatment. Surgery should be performed with great care, bearing clearly in mind the risks and benefits of the procedure. With attention to the unique aspects of care of the singer, excellent outcomes should be expected in most cases.



