


Introduction
Cosmetic and functional nasal surgery requires a detailed knowledge of the anatomy of nasal structures, in order to plan the most effective strategies for changing those structures. Autologous nasal septal grafts are often believed to be the most successful material for nasal reconstruction during external rhinoplasty.Reference Keefe and Cupp1 Although artificial materials such as Medpor® have been used, they have been associated with a higher incidence of short- and long-term complications, including extrusion when placed in areas with thin overlying skin.Reference Sajjadian, Naghshineh and Rubinstein2 Traditional representations of the nasal septal cartilage commonly portray it as having a quadrilateral shape – indeed, this cartilage is also known as the quadrilateral cartilage. However, the true shape of this cartilage includes a posterior ‘tail’ of cartilage which lies between the vomer and the perpendicular plate of the ethmoid (Figure 1).Reference Daniel3 This posterior prolongation of cartilage has been described in some anatomical texts as the ‘sphenoidal process’ of the nasal cartilage.Reference Mladina and Krajina4, Reference Van Loosen, Van Zanten, Howard, Verwoerd-Verhoef, Van Velzen and Verwoerd5 This area has the potential to provide extra cartilage in surgical cases requiring reconstruction or augmentation of nasal structures.

Fig. 1 The true shape of the septal cartilage (shaded).
Structured rhinoplasty procedures involve substantial reconstruction of the nasal cartilage skeleton. Additional cartilage may be needed for spreader grafts or a columella strut. Further cartilage may be required to provide onlay grafts to achieve the desired nasal shape. Even in primary rhinoplasties, the availability of cartilage may be scarce, and all possible sources of cartilage from the nasal septum must be harvested in these cases if the use of cartilage from other sites (e.g. conchal or costal) is to be limited.
Previously, we had noted the posterior prolongation of the nasal septum to be consistently present in surgical cases, and had found it a useful material for nasal reconstruction. However, we found no work documenting the presence, characteristics and possible uses of the posterior prolongation area of the septal cartilage in a clinical setting. We therefore set out to prospectively examine the dimensions and use of this area in primary, open, structured rhinoplasty procedures. We also aimed to investigate the extent to which this cartilage could be demonstrated on computed tomography (CT) scanning.
Materials and methods
Institutional ethical board approval was granted, and informed consent was obtained from all patients.
In order to assess the presence of, and uses for, the posterior prolongation of the septal cartilage, we studied consecutive primary, open, structured rhinoplasty procedures and measured the dimensions of the posterior cartilage projection.
In addition, we evaluated consecutive CT radiographs of a separate cohort of patients, obtained from an electronic CT database of unoperated cases, in order to assess the radiologically determined dimensions of the posterior prolongation of the cartilaginous nasal septum.
Operative procedure
The standard external or open, structured rhinoplasty approach was used, exposing the upper lateral cartilages, the dorsum of the cartilaginous septum, and the bony dorsum.Reference Timperley, Stow, Srubiski, Harvey and Marcells6 The septum was freed from its surrounding mucoperichondrium on both sides, and the upper lateral cartilages were freed from the nasal septum. Using a size 15 blade and a Freer's elevator, the septal cartilage was harvested as far posteriorly as possible, leaving a minimum 1 cm wide caudal and dorsal strip to maintain structural integrity. The posterior prolongation of the cartilage was followed and freed as far back as possible. This was initially done under headlight guidance; however, if the cartilage proceeded far posteriorly an endoscope was used to facilitate the most posterior dissection of the cartilage (Figure 2). If possible, the cartilage was removed in one piece (see Figure 3).

Fig. 2 Endoscopic view of the posterior prolongation, or ‘cartilage tail’, being harvested from within the bony septum.

Fig. 3 Pathological photograph showing an example of a harvested septal cartilage with posterior prolongation.
Measurement of harvested cartilage
The resultant cartilage piece was measured and photographed; if the cartilage had been harvested in more than one piece, the pieces were carefully reconstructed before measurement. Measurement was done by extending a line representing the posterior bone–cartilage junction inferiorly to the bottom of the excised cartilage. A second line was then extended from this line posteriorly through the middle of the posterior prolongation, to the posterior limit of the prolongation, as shown in Figure 4. The length of this second line was noted. The width and thickness of the septal cartilage were measured three times and the mean value for each parameter noted. The length and height were multiplied to estimate the posterior prolongation area in the sagittal plane. The position of the process relative to the surrounding septal bone (i.e. left, right or middle) was also noted.

Fig. 4 Measurement of posterior prolongation dimensions. The yellow line indicates the posterior bone–cartilage junction, which is extended inferiorly and used to delineate the anterior boundary of the posterior prolongation. The length, width and height of this prolongation are then measured (red lines).
The subsequent use of the posterior prolongation cartilage was documented. This was categorised as either crush cartilage coverage for contouring, spreader graft, strut or ‘unused’.
Post-operative follow up
The most recent post-operative follow-up data available were used to assess patient-reported cosmetic outcome after septorhinoplasty. A global Likert change scale was used to assess cosmesis, with patients rating their cosmesis change from −3 to +3.
Computed tomography study
In order to categorise the radiological characteristics of the posterior prolongation of the septal cartilage, a separate patient cohort was studied. The CT scans of a separate group of patients who had not undergone previous septal surgery or rhinoplasty were examined, by viewing multiplanar CT images stored electronically, and cartilage measurements in multiple planes were made digitally to optimise accuracy. The patients were chosen in alphabetical sequence from an electronic database, after verification that no previous septal surgery had taken place. The presence and dimensions of the posterior prolongation of the septal cartilage were noted by examining the parasagittal images to determine the configuration of the nasal cartilage. Identification of the posterior prolongation of the cartilage was possible by identifying the boundaries of the bony septum when viewing successive parasagittal images. This enabled the quadrilateral cartilage and its posterior extension to be located, usually defined by surrounding bony boundaries. A line was extended from the posterior bone–cartilage junction, as in the operative study, to indicate the anterior limit of the posterior prolongation. The average width and length of the posterior prolongation were recorded. The coronal images were then examined to determine the average thickness of the process. Figure 5 shows one of the parasagittal images used to determine the dimensions – the anterior bony boundary of the perpendicular plate of the ethmoid is clearly visible, although the bony boundaries of the posterior prolongation are less easily seen on this scan. Figure 6 shows the corresponding coronal image used to determine the thickness of the cartilage.

Fig. 5 Parasagittal computed tomography scan showing measurement of the length and height of the posterior prolongation.

Fig. 6 Coronal computed tomography scan showing measurement of the width of the posterior prolongation.
Results and analysis
Twenty-five patients undergoing primary rhinoplasty were assessed (8 (32 per cent) males and 17 (68 per cent) females). The mean patient age ± standard deviation (SD) was 29.1 ± 10.2 years (range, 16.3–48 years). All patients were of Caucasian ethnic origin.
One patient did not have a harvestable posterior prolongation. For the remaining 24 patients, the mean ± SD dimensions of the posterior prolongation were: length, 24.3 ± 8.40 mm (range, 10–40 mm); height, 4.33 ± 0.34 mm (range, 2–8 mm); and width, 1.1 ± 0.35 mm (range, 1–2 mm). In 21 (88 per cent) patients, the posterior prolongation was present between two plates of bone; it appeared to be on the left of the bony septum in 2 patients and on the right in 1 patient. In the sagittal plane, the mean area of measured posterior prolongation cartilage was 102.8 ± 41.8 mm2 (range 20–175 mm2).
In two patients, the posterior prolongation was not used and was discarded at the end of the operation. In three patients, the harvested posterior prolongation was used to construct one or more spreader grafts. In 22 patients, the harvested cartilage was used for onlay cartilage grafts for contouring – the cartilage in these patients was not suitable for use as a spreader graft owing to its friability. In 8 of these 22 patients, the cartilage was used at the nasal tip, in 4 in the infratip area, in 6 in the supratip area, and in 4 in the middle third area.
In 9 patients, the posterior prolongation was harvested as a single piece (mean length, 16.0 ± 4.47 mm; range, 10–21 mm), whilst in the other 15 it was removed piecemeal (mean length, 29.3 ± 5.80 mm; range, 20–40 mm), reflecting the increased friability of the posterior prolongation cartilage in comparison to the quadrilateral cartilage.
Seventeen patients had post-operative cosmesis scores available from their latest post-operative visit, at a mean post-operative follow-up interval of 45 ± 8.7 weeks (range, 22.9–59.1 weeks). All of these 17 patients reported an improvement in cosmesis post-operatively. The mean improvement score was +2.41 ± 0.71.
In the radiological group, 25 consecutive patients who had not undergone previous septal surgery were assessed: 11(44 per cent) males and 14 (56 per cent) females. The mean patient age was 45.4 ± 15.9 years (range, 25–76 years). All the CT scans assessed showed a visible posterior prolongation cartilage; mean dimensions ± SD were: length, 18.1 ± 5.1 mm (range, 8–26 mm); height, 4.2 ± 1.1 mm (range, 3–6 mm); and width, 1.5 ± 0.63 mm (range, 1–3 mm).
Discussion
Miles et al. have noted that much of the literature on the nasal septum comprises descriptions of various septoplasty techniques rather than definitions of the septal anatomy encountered.Reference Miles, Petrisor, Kao, Finn and Throckmorton7 However, the presence of the posterior prolongation of the septal cartilage has been noted in some previous work. An estimated length of 10–18 mm was quoted in one text.Reference Daniel3 This appears to be an underestimate in comparison with our finding of a mean length ± SD of 24.3 ± 8.40 mm.Reference Daniel3 In one of the few studies to investigate the posterior prolongation in a clinical context, Kim et al. quoted a figure of 26.05 ± 5.32 mm for posterior prolongation length in patients with septal deviations.Reference Kim, Cho, Kim, Kim and Lee8
It has previously been estimated that, once the dorsal and caudal struts are discounted, the area of nasal cartilage available for septal grafts averages 420 mm2, not including the cartilage available in the posterior prolongation.Reference Miles, Petrisor, Kao, Finn and Throckmorton7 We calculated that the average septal area available from the posterior prolongation is 102.8 mm2, which represents a potential 25 per cent increase in the cartilage available for grafts.
Investigation of the embryological development of the posteroinferior part of the nasal septum shows that the area is initially cartilaginous; ossification proceeds with the vomer developing as two bony plates with cartilage in between.Reference Yilmaz and Altuntas9, Reference Melsen10 Residual cartilage in this area will thus tend to be encased in the bone of the vomer on either side, and this is what was found in practice in our study (in 88 per cent of cases, the cartilage was encased in bone) (see Figure 2), although in some patients the posterior prolongation was on one side or the other of a single bony plate. We also observed that, even in severe deviation of the vomer, it was possible to harvest the cartilage process, which usually accompanied the bony deviation (see Figure 7). This is in line with work showing an association between the length of the posterior prolongation and certain septal deviations.Reference Dogru, Yasan and Tuz11 Kim et al. have found an increased posterior prolongation length in patients with septal deviation, suggesting an association between delayed ossification of the septal cartilage and the presence of a deviation.Reference Kim, Cho, Kim, Kim and Lee8 They noted that in patients with a septal deviation, the posterior prolongation cartilage had ‘burst through’ the osseous line linking the perpendicular plate of the ethmoid and the vomer. The same group have observed that posterior prolongation length increases with septal deviation angle.Reference Kim, Kim, Cho and Park12 It is of course patients with deviations who most frequently require septal surgery.
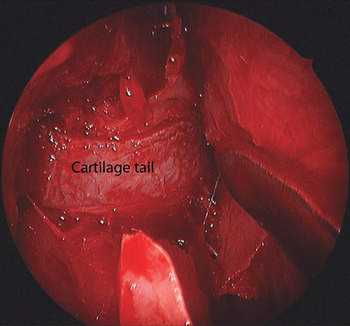
Fig. 7 Endoscopic view of a posterior prolongation (‘cartilage tail’) being harvested from a deviated septal spur.
Vetter et al. investigated the cellular and growth characteristics of the nasal septal cartilage in detail, and found that the posterior prolongation exhibits lower cell density and proliferative capacity in comparison to other areas of cartilage.Reference Vetter, Pirsig, Helbing, Heit and Heinze13 Certainly, the cartilage that we harvested from this region was more friable than that taken from the main body of the quadrilateral cartilage, which meant that the cartilage was sometimes unsuitable for use as a strut or spreader graft. However, it was more dependable as a crushed cartilage contour disguiser graft. Using crushed cartilage is an established method of concealing contour irregularities, and there is evidence for its success and durability in doing so.Reference Breadon, Kern and Neel14, Reference Cakmak and Buyuklu15 Our results showed that good cosmetic results were achieved with the use of this cartilage, at close to one year after surgery.
We found that an endoscope was a useful adjunct when harvesting the full length of the posterior prolongation. We routinely used an endoscope as part of functional rhinoplasty surgery, in order to optimise the nasal valve by reducing the inferior turbinates, and we found that endoscopic septal harvesting fitted in well with the sequence of the operation. However, we found that the longer the posterior prolongation being harvested, the more likely it was to fracture and be removed piecemeal. Dissection of the most posterior parts of the posterior prolongation was difficult to achieve without fracturing the cartilage.
Radiological assessment showed that the posterior prolongation appears to be well demonstrated on CT imaging using multiplanar reconstructions and averaging of measurements over a number of sections, although the shorter average length noted may indicate that CT scanning underestimates the true length of the harvestable process. Computed tomography scanning has previously been shown to be a viable method of estimating the nasal septal area.Reference Kim, Cho, Kim, Kim and Lee8 This would suggest that a pre-operative CT scan can be used to predict the presence of harvestable cartilage in cases in which some uncertainty exists about the need for distant cartilage harvest to reconstruct the nose.
• A posterior prolongation of the cartilaginous nasal septum is frequently present, and is associated with septal deviations
• Computed tomography (CT) is a feasible way of assessing septal cartilage
• The posterior prolongation is useful as a cartilage graft source in septorhinoplasty
• The posterior prolongation can be assessed via CT
However, we are aware of the limitations of this radiological part of our study. Unfortunately, it was not possible to correlate the posterior prolongation measurements obtained from clinical patients with those visible on their own CT scans, as only a minority had scans that could be assessed in this way. Also, specifically excluded from both parts of the study were patients who had had previous septal or rhinological surgery, and of course it is these revision patients in whom the presence of extra septal cartilage is most useful in reconstruction. Further work may shed light on correlations between imaged and actual posterior prolongation dimensions, and on the use of CT scans in revision cases.
Our patients were of Caucasian ethnic origin, and further work would be needed to demonstrate the presence and usefulness of the posterior prolongation in patients of other ethnic origins. However, at least for Caucasian noses, our study suggests that the posterior prolongation of the septal cartilage is a possible source of extra graft material in cases in which usable nasal cartilage is scarce.
Acknowledgements
Mr Phillips would like to thank the British Rhinological Society, the Ethicon Travelling Fellowship and the Ronald Raymond Barber Fellowship for helping to make his fellowship possible.







