Introduction
Temporomandibular disorders is a collective term for a number of clinical problems involving the muscles of mastication, the temporomandibular joint (TMJ) and associated structures, or both.Reference Villalón, Arzola, Valdivia, Fresno, Santander and Gutiérrez 1 Otological symptoms, including otalgia, tinnitus, vertigo, subjective hearing loss and otic fullness, are associated with temporomandibular disorders.Reference Ramirez, Ballesteros and Sandoval 2 This symptom combination is termed Costen's syndrome because James Costen published a series of articles on this topic.Reference Costen 3 – Reference Costen 6 Costen attributed the otological symptoms to a misplaced mandibular condyle, resulting in pressure on ear structures. Since then, numerous theories have been proposed to explain the origin of otological symptoms in temporomandibular disorder patients.Reference Penkner, Köle, Kainz, Schied and Lorenzoni 7 – Reference Pihut, Majewski, Wisniewska and Reron 10
This prospective study aimed to determine the incidence of otological symptoms in temporomandibular disorder patients and, specifically, to assess audiometric findings as a more objective method of detecting otological dysfunction in these patients. Most previous reports of audiometric results in temporomandibular disorder patients involved only small cohorts, thus limiting the statistical evaluation.Reference Totta, Santiago, Gonçales, Saes and Berretin-Felix 11 – Reference Dolowitz, Ward, Fingerle and Smith 16 The findings of the current study were interpreted in the light of recently published research findings. For this purpose, a PubMed search was conducted to identify relevant articles published in the English language between 1934 and 2015 using the main search terms ‘temporomandibular joint’ and ‘temporomandibular disorders’.
Materials and methods
This prospective study took place over one year, starting on 10 July 2014. Local ethics committee approval was granted and informed consent was obtained from both patients and control participants to participate in the study.
Consecutive patients attending the Otolaryngology Clinic at El-Sahel Teaching Hospital, Cairo, were considered for inclusion in the study if they presented with otalgia or headache attributable to disturbance of the masticatory system.Reference Kuttila, Kuttila, Bell, Alanen and Jouko 17 Patients were excluded if they were aged over 60 years or had a family history of hearing loss, a history of significant noise exposure or ototoxic drug consumption, typical Ménière's complex symptoms, or previous ear surgery. Patients were also excluded if they were subsequently found to have otitis externa, acute otitis media, a perforated tympanic membrane, an upper respiratory tract infection, parotitis, an acute periodontal infection or intracranial pathology as detected by imaging.Reference Brookes, Maw and Colemnan 18
A control group of healthy adults (i.e. not suffering from temporomandibular disorders) was recruited from hospital staff and patient relatives. The same exclusion criteria were applied to the control group.
Patients were asked to complete a standard questionnaire to record the duration of symptoms, including any otological complaints (otalgia, tinnitus, subjective hearing loss, sensation of fullness in the ear and/or vertigo). Complaints of any disturbance during mastication, such as noises in the TMJ, limited mouth opening associated with jaw deviation (i.e. closed lock) or a history of joint dislocation (i.e. open lock) were also noted.Reference Bag, Gaddikeri, Singhal, Hardin, Tran and Medina 19 Any possible predisposing factors for temporomandibular disorder were explored, including prior dental surgery, direct trauma to the jaw or the presence of parafunctional habits (especially bruxism).Reference de Souza, de Mello, Magalhães, Morais and Vasconcelos 20 A standard examination was performed to classify the major dysfunction as (1) a TMJ disorder, (2) masticatory muscle dysfunction, (3) headache attributable to temporomandibular disorder or (4) any combination of these morbidities.Reference Shaffer, Brismée, Sizer and Courtney 21 , Reference Peck, Goulet, Lobbezoo, Schiffman, Alster-Gren and Anderson 22
Both patients and control participants underwent pure tone audiometry and tympanometry by an audiologist blinded to the clinical data. A Grason-Stadler audiometer (Model GSI 67, Milford, New Hampshire, USA) was used in a sound-proof booth for pure tone audiometry at the following frequencies: 0.25, 0.5, 1, 2, 4 and 8 kHz. The pure tone average for air-conduction thresholds was used to categorise hearing loss as: normal, a threshold of less than 25 dB HL; mild loss, more than 25 dB HL and less than 40 dB HL; and moderate loss, more than 40 dB HL and less than 65 dB HL.Reference Jun, Hwang, Lee, Lee, Sang and Choe 23 Hearing loss was classified as unilateral or bilateral, and as sensorineural, conductive or mixed. Tympanometry was performed using a Grason-Stadler tympanometer (Model GSI 38). The tympanogram was classified according to middle-ear pressure as: type A, more than −100 daPa; type B, not measurable; or type C, less than −100 daPa.Reference Schröder, Lehmann, Sauzet, Ebmeyer and Sudhoff 24
Statistical analysis was performed using SPSS for Windows, Version 16.0 (Chicago, Illinois, USA). Results were expressed as the mean ± standard deviation or number (percentage). Comparisons between categorical data were performed using the χ2 test. A p value of less than or equal to 0.05 was considered significant and of less than 0.01 as highly significant. The major categorical data type used for statistical analysis was audiometric findings in temporomandibular disorder patients vs control participants.
Results
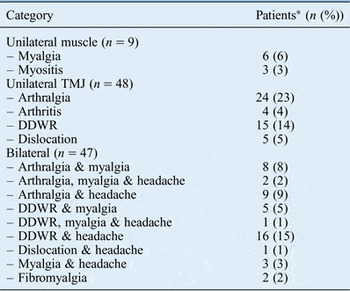
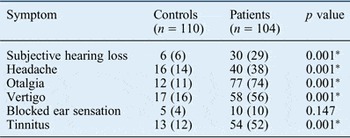
The study included 104 temporomandibular disorder patients and 110 control participants. The demographic features of both groups are shown in Table I. Most temporomandibular disorder patients were women of childbearing age. The clinical dysfunction categories of temporomandibular disorder patients are listed in Table II. Patients with TMJ disorders outnumbered those with masticatory muscle disorders. However, many patients experienced both conditions. Table III shows the otological symptoms reported by temporomandibular disorder patients. Many of these patients had a combination of various otological symptoms (subjective hearing loss, headache, otalgia, vertigo, blocked ear sensation and/or tinnitus), thus meeting the clinical diagnostic criteria for Costen's syndrome. The prevalence of all otological symptoms, apart from a blocked ear sensation, was significantly higher in temporomandibular disorder patients than in control participants. Table IV shows the audiometric profile of temporomandibular disorder patients. An important finding is that 25 per cent of patients had unilateral (ipsilateral to the affected temporomandibular disorder side) or bilateral (in bilaterally affected patients) hearing loss, which was usually mild.
Table I Both study groups: demographic features

SD = standard deviation; F = female; M = male
Table II Temporomandibular disorder patients: clinical dysfunction categories

*n = 104. TMJ = temporomandibular joint; DDWR = disc displacement with reduction
Table III Both study groups: otological symptoms

Data are expressed as n (%). *p < 0.01
Table IV Temporomandibular disorder patients: audiometric profiles

*n = 104
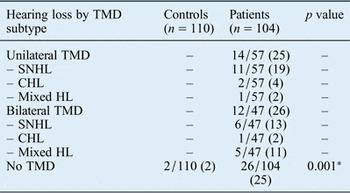
The types of hearing loss are listed in Table V. Most abnormal audiograms showed sensorineural hearing loss; although uncommon, conductive and mixed hearing loss were also encountered. Audiometric data for temporomandibular disorder patients were compared with those of the control group (shown in Table V). Hearing loss was significantly associated with temporomandibular disorder (p = 0.001). As shown in Table VI, type B or C tympanograms were obtained for 6 temporomandibular disorder patients with bilateral disease and ipsilaterally in 14 patients with unilateral disease. This may indicate some middle-ear dysfunction in temporomandibular disorder patients. These changes are highly significant (p = 0.001) compared with the control group.
Table V Temporomandibular disorder patients: types of hearing loss

Data are expressed as n (%). *p < 0.01. TMD = temporomandibular disorder; SNHL = sensorineural hearing loss; CHL = conductive hearing loss; HL = hearing loss
Table VI Both study groups: comparison of tympanometry findings

Data are expressed as number (%). *Highly significant.
Table VII shows the correlation between hearing loss and a clinical diagnosis of masticatory dysfunction in temporomandibular disorder patients. There was no significant correlation between diagnostic category and the degree of hearing loss (p > 0.05).
Table VII Temporomandibular disorder patients: correlation between degree of hearing loss and diagnostic category

Data are expressed as n (%). *Not significant. TMJ = temporomandibular joint
Discussion
Most temporomandibular disorder patients included in the current study were women of childbearing age (Table I). This is consistent with the findings of previous studies and may be related to hormonal fluctuations that may affect TMJ nociceptive responses.Reference Kramer and Bellinger 25 As indicated in the inclusion criteria, otalgia and/or headache were almost universally reported in this study (Table III), with the pain frequently being referred to areas remote from the TMJ, such as the face, back of the neck or shoulders. Most recent studies on TMJ nociception focus on central nervous system sensitisation as an important factor in the pain referral pattern for temporomandibular disorder.Reference Sarlani and Greenspan 26 , Reference Sessle 27
The prevalence of at least one otological symptom other than pain (i.e. tinnitus, vertigo, blocked ear sensation or subjective hearing loss) was 70 per cent for those with normal audiometry and tympanometry findings. These medically unexplained symptoms can be referred to as somatisation,Reference Jahn 28 , Reference Ullas, McClelland and Jones 29 and may be related to a central processing disorder in temporomandibular disorder patients.Reference Moayedi, Weissman-Fogel, Salomons, Crawley, Goldberg and Freeman 30 , Reference Hind, Haines-Bazrafshan, Benton, Brassington, Towle and Moore 31 The symptoms could be augmented by emotional factors.Reference Hilgenberg, Saldanha, Cunha, Rubo and Conti 32 Indeed, the taxonomy of the diagnostic criteria for temporomandibular disorder considers the psychosocial status of the patient as axis 2 in the evaluation of the disorder.Reference Peck, Goulet, Lobbezoo, Schiffman, Alster-Gren and Anderson 22
Apart from a putative central contribution of otological symptoms associated with temporomandibular disorder, a normal audiogram and tympanogram does not exclude the possibility of subtle physiological changes in the middle or inner ear. A study of patients with unilateral TMJ dysfunction assessed by multiple frequency tympanometry reported significant alterations in the resonance frequency for the affected ear compared with the normal contralateral ear.Reference Riga, Xenellis, Peraki, Ferekidou and Korres 33 These changes were found despite normal otoscopy findings, 226-Hz tympanometry, pure tone audiometry and brainstem auditory evoked potentials in the affected ear. The authors concluded that TMJ dysfunction could cause subtle alterations in middle-ear biomechanics, and hypothesised that these could be attributable to anatomical links between the TMJ and the middle ear, including the discomalleolar ligament, the anterior malleolar ligament and the tendon between the tensor tympani and tensor veli palatini muscles.Reference Rodríguez-Vázquez, Mérida-Velasco, Mérida-Velasco and Jiménez-Collado 34 – Reference Kierner, Mayer and v Kirschhofer 36 Changes in tension on these structures in TMJ dysfunction could be transmitted to the malleus, thereby altering the stapes position.Reference Riga, Xenellis, Peraki, Ferekidou and Korres 33 The latter could cause a pressure change in inner-ear fluids and alter the polarisation state of cochlear and vestibular hair cells, thereby contributing to symptoms of ear fullness, tinnitus, subjective hearing loss and vertigo.Reference Noreńa 37 – Reference Mom, Pavier, Giraudet, Gilain and Avan 39 Subtle changes in inner-ear fluid pressure have been detected by multiple frequency tympanometry.Reference Franco-Vidal, Bonnard, Bellec, Thomeer and Darrouzet 40
Reports of audiometric findings in temporomandibular disorder patients are contradictory: some studies have reported no hearing loss,Reference Totta, Santiago, Gonçales, Saes and Berretin-Felix 11 – Reference Toller and Juniper 13 while others have documented a correlation between temporomandibular disorder and sensorineural hearing loss.Reference McKenna and Hall 14 – Reference Dolowitz, Ward, Fingerle and Smith 16 The major drawback of most studies was the small patient cohort, which limits statistical evaluation. In the current study of 104 temporomandibular disorder patients, pure tone audiometry revealed ipsilateral or bilateral hearing loss in 25 per cent of patients with unilateral or bilateral temporomandibular disorder, respectively (Table IV). Hearing loss was usually mild and most commonly sensorineural (Table V). Audiometric findings were significantly different from those of the control group (Table V).
The cause of hearing loss associated with temporomandibular disorder can only be speculated upon. Recently, a hypothesis was proposed linking temporomandibular disorders, Eustachian tube dysfunction and inner-ear dysfunction.Reference Franz and Anderson 41 Irritation in the TMJ region was hypothesised to result in the release of inflammatory mediators in the Eustachian tube via an axon reflex, which could further activate the anterior cervical sympathetic system. The latter would enhance neurogenic inflammation in the Eustachian tube, resulting in reduced middle-ear ventilation. The imbalance between middle-ear and inner-ear pressure could alter the polarisation state of cochlear hair cells, thereby causing sensorineural hearing loss.Reference Noreńa 37 – Reference Mom, Pavier, Giraudet, Gilain and Avan 39 In this context, another recent study reported multiple system dysregulation (especially affecting the sensory, autonomic and inflammatory domains) in patients with painful temporomandibular disorders.Reference Chen, Nackley, Miller, Diatchenko and Maixner 42 This hypothesis may help explain the various types of hearing loss observed in patients with various categories of temporomandibular disorder in the current study (Table VII).Reference Franz and Anderson 41
-
• Costen's syndrome combines various otological symptoms with temporomandibular disorder
-
• Temporomandibular disorder patients and controls underwent pure tone audiometry and tympanometry
-
• Twenty-five per cent of unilateral or bilateral patients had ipsilateral or bilateral hearing loss, respectively, which was usually mild
-
• Hearing loss was predominantly sensorineural
-
• The otological symptoms and hearing loss associated with temporomandibular disorders may be caused by an altered middle-ear to inner-ear pressure equilibrium
A potential cause of bias in the present study was the difference in sex distribution between the patient (81% women) and control (60% women) groups (p < 0.01). Most control participants were patients’ relatives (87 per cent). However, members of both groups were mostly young or middle aged.
Conclusion
Although otological symptoms in temporomandibular disorder patients have been considered coincidental, recent research supports the validity of Costen's syndrome. However, further studies into the relationship between the masticatory apparatus and ear structures are necessary.