


Introduction
Radiotherapy has long been recognised as a proven treatment for malignancies of the head and neck. However, one of its well documented side effects is osteoradionecrosis of the temporal bone. The tympanic part of the temporal bone is most often involved, resulting in exposed, necrotic bone in the external auditory canal. The aetiology of osteoradionecrosis of the auditory canal and the possible treatment modalities have been described in detail by Metselaar et al. Reference Metselaar, Dumans, van der Huls, Sterk and Feenstra1
Treatment is either conservative or surgical. With conservative treatment, symptoms may slowly decrease and the meatal skin defect may close spontaneously over years.Reference Ramsden2 Surgical treatment can consist of excavation of the necrotic bone and either primary closure of the skin defect or closure with a retroauricular rotational skin flap.Reference Metselaar, Dumans, van der Huls, Sterk and Feenstra1, Reference Hill, Gaze and Grant3
The use of hyperbaric oxygen therapy in addition to any other therapy for head and neck osteoradionecrosis seems to be beneficial, but the effect on this specific group of patients is uncertain.Reference Spiegelberg, Djasim, van Neck, Wolvius and van der Wal4
This paper aims to describe the results of reconstruction of the external auditory canal by transpositioning of the superficial layer of either the anterior or the posterior part of the temporalis muscle, in patients with osteoradionecrosis of the external auditory canal. Due to its vascularisation, the temporalis muscle can be split into an anterior and a posterior part. This muscle can also be split into a superficial and a deep layer. To our best knowledge, the use of such a temporalis muscle flap in the treatment of osteoradionecrotic skin defects of the external auditory canal has not previously been described.
We present the results of this procedure in three patients.
Patients and methods
Patient one
A 47-year-old man presented 11 years after radiotherapeutic treatment (70 Gy) for a nasopharyngeal carcinoma, with persistent ear pain and severe pain in the left temporomandibular joint during mastication.
On examination, he had trismus and mixed hearing loss. Otoscopic inspection revealed exposed, necrotic bone on the inferior and anterior parts of the external auditory canal.
Osteoradionecrosis was confirmed with a computed tomography (CT) scan, which showed corrosion of the anterior and inferior walls of the external auditory canal. In spite of the patient's complaints, there was no indication that the bony structures or soft tissue of the temporomandibular joint were involved.
Patient two
A 45-year-old man had previously been treated for a squamous cell carcinoma of the left external auditory canal, using surgery (a parotidectomy with sleeve resection of the external auditory canal) and radiotherapy (70 Gy). Six months after radiotherapy, osteoradionecrosis was diagnosed, after which the external auditory canal was reconstructed with a pedicled post-auricular skin flap. However, healing was complicated by necrosis of the flap and the remains of the auricle.
One year later, he presented with chronic external otitis and a large area of bare, avascular bone in the external auditory canal, which included mastoid cortex.
Osteoradionecrosis was confirmed with a CT scan, which showed no temporomandibular joint involvement.
Patient three
A 52-year-old man underwent resection of a metastatic tumour in the left parotid gland and received radiotherapy (70 Gy) post-operatively. Five and a half years later, he presented with temporomandibular joint complaints and left-sided chronic external otitis.
Otoscopy revealed exposed, necrotic bone on the anterior and inferior parts of the external auditory canal (Figure 1).
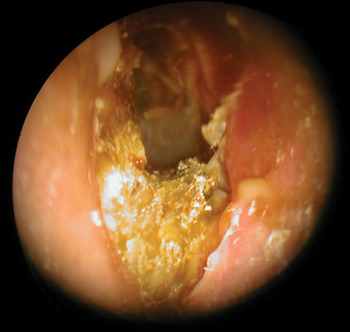
Fig. 1 Pre-operative otoscopic view of the left ear of patient three, showing exposed, necrotic bone of the inferior and anterior parts of the external auditory canal.
The initial intention was to treat the patient conservatively with only hyperbaric oxygen. However, three months after this therapy he was still experiencing temporomandibular joint complaints and chronic otitis.
A CT scan confirmed the presence of osteoradionecrosis of the external auditory canal, with involvement of the mandibular fossa (Figure 2).

Fig. 2 Pre-operative, coronal computed tomography scan of the left ear of patient three, showing the corroded inferior wall of the external auditory canal (i.e. the tympanic bone).
Surgical methods
In all three patients, surgery was performed under general anaesthesia. Either a pre- or retroauricular, S-shaped incision was made and elongated over the temporal bone. The skin of the external auditory canal was removed to fully expose the necrotic bone, which was excavated using sharp and diamond drills until only viable bone was seen.
The temporalis muscle was mobilised and split into an anterior and a posterior part according to its vascularisation (Figure 3). The anterior part remained vascularised by the deep anterior temporal artery, whereas the posterior part remained vascularised by the deep posterior temporal artery. Either the anterior or the posterior part of the temporalis muscle was used, being split into a superficial and a deep layer (Figure 4). The deep layer was re-attached to the periosteum of the skull.

Fig. 3 Surgical photograph looking from the left side of patient one. After a retroauricular incision, the posterior part of the temporalis muscle was mobilised and rotated inferiorly.

Fig. 4 Surgical photograph of patient one, showing splitting of the mobilised flap into superficial and deep layers.
The superficial layer was formed into a flap which was rotated inferiorly into the auditory canal and fixed to the surrounding tissue. The transposed flap remained vascularised by its corresponding (anterior or posterior) deep temporal artery.
At the end of the procedure, an earwick impregnated with Terra-Cortril (Pfizer, New York, USA) was placed in the external auditory canal, with or without a surrounding silicon sheet, to keep the canal open.
All three patients received hyperbaric oxygen therapy pre-operatively. Patients one and three received additional hyperbaric oxygen therapy post-operatively.
Results
There were no complications during or after surgery in any of the patients. Facial function remained intact.
At one month follow up, patient one no longer reported temporomandibular joint complaints or ear pain. At three month follow up, intact skin was seen and the transposed flap had been re-epithelialised.
Patient two no longer suffered from chronic external otitis after surgery. Re-epithelialisation of the external auditory canal was complete within three months. It was planned to place a bone-borne external ear prosthesis one year after surgery.
In patient three, a few small, necrotic flap edges had to be removed one month post-operatively. Two months post-operatively, some granulation tissue was removed with micro-scissors. These procedures were performed without local anaesthesia in an out-patient setting. After three months of follow up, all meatal skin was observed to be re-epithelialised, including the transposed temporalis muscle flap (Figure 5).

Fig. 5 Otoscopic view of patient three, three months post-operatively, showing re-epithelialised meatal skin.
The three patients' results are summarised in Table I.
Table I Patient data summary

Pt no = patient number; Ca = cancer; RT = radiotherapy; y = years; EAC = external auditory canal; Prev = previous; HBOT = hyperbaric oxygen therapy; surg = surgery; FU = follow up; mth = months; Compls = complications; M = male; ant = anterior; inf = inferior; post = posterior; TMJ = temporomandibular joint; HL = hearing loss; pre-op = pre-operative; post-op = post-operative; L = left; COE = chronic otitis externa
Discussion
The influence of radiation on bone was first described by Ewing.Reference Ewing5 After radiotherapy of the temporal bone, the tympanic part is most frequently affected, resulting in exposed, necrotic bone in the external auditory canal. Possible explanations for the relatively frequent involvement of the external auditory canal are its thin skin coverage and its proximity to the middle ear and hence the potentially infected upper respiratory tract (via the eustachian tube).Reference Ramsden2
Therapy for localised osteoradionecrosis of the external auditory canal can be either conservative or surgical.
After prolonged conservative treatment, symptoms may slowly resolve and the meatal skin defect may close spontaneously over years.Reference Ramsden2
Surgical treatment of osteoradionecrosis of the external auditory canal consists of excavation of the necrotic bone and either primary closure of the skin defect or closure with a retroauricular rotational skin flap.Reference Metselaar, Dumans, van der Huls, Sterk and Feenstra1, Reference Hill, Gaze and Grant3 Although reconstruction with a retroauricular skin flap is less invasive, the risk of complications may be higher compared with a temporalis muscle flap, for the following reasons. Firstly, the graft skin flap is selected at random and thus is not vascularised by any specific artery. Secondly, the length–width ratio of the flap may exceed maximum limits. These two factors can contribute to necrosis of the flap. Furthermore, the muscle flap may have an additional advantage over the skin flap in that its preserved vascularisation may enable it to cover a larger area than a skin flap (which is restricted by maximum length–width ratio limits).
The characteristics of the temporalis muscle make it a reliable option for transpositioning. The muscle can be split into an anterior and a posterior segment according to its vascularisation, and also into a superficial and a deep layer. The deep temporalis muscle is vascularised by the anterior and posterior branches of the deep temporal artery. Both branches originate from the maxillary artery on the medial side of the coronoid process. When the flap is rotated, it remains vascularised by the temporal artery, thus preventing flap necrosis and allowing quicker attachment to adjacent structures.
• Osteoradionecrosis is common after head and neck radiotherapy
• Temporal bone osteoradionecrosis may cause exposed, necrotic bone in the external auditory canal
• This can be treated conservatively or surgically
• A temporalis muscle flap can be rotated into the external auditory canal, without necrosis
• An anterior or posterior, superficial layer temporalis muscle flap provides reliable reconstruction
The thinness of the muscle, when split, enables a non-bulky reconstruction. Its flexibility makes it a versatile flap that can be used for the reconstruction of numerous defects. It is considered a viable alternative for free-flap transplantations in the craniofacial area.Reference Dallan, Lenzi, Sellari-Franceschini, Tschabitscher and Muscatello6–Reference Clauser, Curioni and Spanio8 The temporalis muscle and/or fascia flap is used for a variety of reconstruction purposes in craniofacial surgery, including reconstruction of the orbit, maxilla, palate, oropharynx, cranial cavity, temporomandibular joint, mandible, face, eyelid, mastoid and ear. Many authors attribute the discovery of this muscle flap to Verneuil or Lentz.Reference Clauser, Curioni and Spanio8, Reference Smith, Ducic and Adelson9
Hyperbaric oxygen therapy appears to be beneficial in the treatment of osteoradionecrosis in the head and neck region.Reference Spiegelberg, Djasim, van Neck, Wolvius and van der Wal4 It has been proved beneficial in the treatment of osteoradionecrosis of the jaw.Reference Curi, Dib and Kowalski10, Reference Peleg and Lopez11 However, its effectiveness for the treatment of osteoradionecrosis of the temporal bone, and specifically that involving the external auditory canal, has not yet been proven.
The risks of the described surgical procedure are bleeding, infection, flap necrosis, facial paralysis, and an altered appearance due to temporal indentation or an overly bulky flap. However, the flap usually atrophies over time.
After the transposed muscle flap has been sutured in the external auditory canal, it needs to be covered with skin. This grows from the surrounding parts of the auditory canal skin. In our three patients, re-epithelialisation had occurred within three months post-operatively.
Conclusion
To our best knowledge, the use of the temporalis muscle for the reconstruction of the external auditory canal has not previously been described. In our three patients undergoing this procedure, all gained fully epithelialised meatal skin and none suffered recurrence of the osteoradionecrosis.
In our opinion, transposition of the anterior or posterior superficial part of the temporalis muscle provides a reliable flap for the reconstruction of the external auditory canal, with a satisfactory outcome.






