


Introduction
Benign paroxysmal positional vertigo (BPPV) is considered the most common cause of vertigo. The diagnosis is made by detecting typical nystagmus on positioning the patient in the Dix–Hallpike position.Reference Yimtae, Srirompotong and Srirompotong1 Many cases of BPPV resolve spontaneously within a few weeks or months. Attacks tend to occur in clusters, and symptoms may recur after an apparent period of remission. Particle repositioning manoeuvres (of which Epley's manoeuvre is one) have become the ‘gold standard’ for treatment of this disorder.Reference Hilton and Pinder2, Reference Epley3
Double blind studies addressing follow up after such treatment have generally been of short-term duration. Three trials reported data after follow-up periods of only one to two weeks.Reference Radtke, Neuhauser and von Brevern4–Reference Froehling, Bowen and Mohr6 Only four trials could be identified which reported follow-up data for more than six months.Reference Wolf, Hertanu and Novikov7–Reference Prokopakis, Chimona, Tsagournisakis, Christodoulou, Hirsch and Lachanas10
This study aimed to assess the recurrence rate and the time to recurrence five years after treatment of BPPV with Epley's manoeuvre, as well as to identify predictors for recurrence.
Patients and methods
This study was begun in 1998 in the ENT department of Assiut University, when Epley's manoeuvre began to be offered to patients with posterior canal BPPV. Two hundred and sixty-nine patients were offered the manoeuvre from 1998 to the end of 2001. All these patients were diagnosed as having posterior canal BPPV, from a history of vertigo in the triggering position and detection of typical nystagmus in the Dix–Hallpike position. The following data were kept for every patient: name, age, sex, duration of complaint, number of attacks, and previous exacerbations and remissions of attacks.
After giving informed consent (as per the local ethics committee), patients were offered Epley's manoeuvre if their current exacerbation of BPPV had lasted for at least one month. It was assumed that this was enough time for spontaneous remission to take place, and to effect separation of loose particles from the otoconia to the endolymph.
The effectiveness of the manoeuvre was assessed at two weeks and one, three, six and 12 months after treatment. Patients were reviewed and data recorded regarding recurrence of symptoms and the patient's subjective sense of health (graded as complete cure, more than 50 per cent improvement, less than 50 per cent improvement, no improvement or getting worse).Reference Epley3 Those patients who had experienced further attacks after the first Epley's manoeuvre treatment were offered a second treatment. Dates of recurrence were ascertained (from the patient and/or their carer), related to memorable national and religious events. The 269 posterior canal BPPV patients were treated in a special clinic dedicated to the treatment of dizzy patients. One hundred and ninety-six patients completed one-year follow up. However, this clinic was then closed for three years for administration reasons.
Five years after the 269 patients had first been offered Epley's manoeuvre, they were sent a questionnaire (shown as Appendix 1) and an invitation to attend a specialised clinic for re-examination, whether or not they needed further treatment. One hundred and three patients (38 per cent of the total number) responded by attending the specialised clinic and returning the questionnaire. No other questionnaires were returned. No data were available for the five-year follow-up period for the defaulters. The 103-strong ‘present cohort’ of patients was analysed.
During each patient's review in the specialised clinic, the following were performed: full clinical history with handing out of a questionnaire; full ENT examination; Dix–Hallpike testing; and positional testing using electronystagmography (ENG).
Patients were considered to be cured of BPPV (i.e. no recurrence) if they had suffered no attacks during the five-year follow-up period since Epley's manoeuvre treatment, or only mild attacks not requiring medical consultation.
The original Epley's manoeuvre treatment was considered to be successful if the patient reported subsequent complete resolution or more than 50 per cent improvement of symptoms.
Data analysis
Data were analysed using the Statistical Package for the Social Sciences version 11 software. Variables were expressed as numbers and percentages. Chi-square testing was used for statistical comparison between groups. Significant variables at univariate analysis were entered into a logistic regression model to identify independent predictors of recurrence. Kaplan–Meier estimates were used to estimate the percentage of patients free of recurrence, and log rank tests were used to compare subgroups. The two groups of patients with mild attacks and major attacks were merged together for chi-square calculation. p ≤ 0.05 was considered to be statistically significant.
Results
Two hundred and sixty-nine patients were offered Epley's manoeuvre during the period 1998–2001. One hundred and three (38.3 per cent) patients completed five years' follow up and returned for reassessment. These same 103 patients returned completed questionnaires. This present cohort of patients was found to match the defaulters (n = 166) regarding age, sex, duration of BPPV complaints and number of BPPV exacerbations before receiving Epley's manoeuvre (Table I).
Table I Cross-tabular analysis of follow-up patients and defaulters: age, sex, and pre-treatment duration of attacks and number of exacerbations

* Prior to initial treatment. Yrs = years; pts = patients
The 103 patients' ages ranged from 19 to 65 years, with a mean age of 48.2 years (standard deviation (SD) 11.1 years). Fifty-eight patients (56 per cent) were female and 45 (44 per cent) male.
Table II shows results for the 196 patients who completed one-year follow up.

Of the 103 patients returning for five-year follow-up assessment, 67 patients (65 per cent) had suffered no further attacks, 29 (28 per cent) had suffered minor attacks (i.e. symptoms not severe enough to require medical advice), and seven (7 per cent) had suffered major attacks (i.e. severe symptoms requiring medical advice). The latter two groups of patients (i.e. minor attacks and major attacks) were merged together to enable statistical analysis of BPPV recurrence.
Data were retrieved from patients' medical records. Following their initial Epley's manoeuvre treatment, 75 per cent of the 103 re-presenting patients (77/103) had suffered no further BPPV during the first follow-up year. Epley's manoeuvre had needed to be performed more than once for patients with a less than complete cure (25 per cent; 26/103); this had increased the first year cure rate to 93 per cent (96/103). None of 103 re-presenting patients had been offered Epley's manoeuvre between the first and the fifth follow-up year. Of the 26 patients who had required a second Epley's manoeuvre treatment within the first year, the duration of recurrence ranged from two to six weeks after treatment, with a mean and median of 3.5 weeks and SD of one week. Comparing those patients who had required a second Epley's manoeuvre treatment, regarding their age, sex, and the number and duration of BPPV attacks before receiving treatment, only gender was found to have a significant effect; female patients were statistically significantly more likely to need a second Epley's manoeuvre treatment, compared with male patients (32.8 vs 15.6 per cent, respectively; p < 0.05). The study aimed to verify whether these factors affected long-term recurrence of BPPV after stabilisation of the condition by one or more Epley's manoeuvre treatments.
Univariate analysis for predictors of recurrence over five-year follow up was performed. This analysis showed that a higher incidence of recurrence was associated both with an age of 40 years or more, and with a duration of attacks of three years or more, at the time of initial Epley's manoeuvre. Patients' sex, number of exacerbations and receipt of a second Epley's manoeuvre treatment were not predictors of recurrence over the five-year follow-up period (Table III).
Table III Univariate analysis of predictors of recurrence over five-year follow up

* Prior to initial treatment. Yrs = years; EM = Epley's manoeuvre
Multivariate logistic regression revealed that the duration of illness prior to Epley's manoeuvre treatment was the only independent predictor of recurrence over the five-year follow-up period. Patients with a BPPV duration of three years or more at the time of initial Epley's manoeuvre treatment were 162.5 times more likely to experience recurrence during the five-year follow-up period, compared with those with a BPPV duration of less than three years (odds ratio = 162.5; 95 per cent confidence intervals = 30.97–852.7; p < 0.001).
During the five-year follow-up period, patients' overall mean time to recurrence of posterior canal BPPV was 46.3 months. The time to recurrence was significantly longer among patients aged less than 40 years, those with less than three years of BPPV attacks before initial Epley's manoeuvre treatment, and those with less than six BPPV exacerbations before initial Epley's manoeuvre treatment. Gender had no significant effect on time to recurrence. These results are shown as Kaplan–Meier curves in Figures 1, 2 and 3.

Fig. 1 Kaplan–Meier curves for effect of patient age on benign paroxysmal positional vertigo recurrence over the five-year follow-up period after initial Epley's manoeuvre (EM) treatment. Recurrence was significantly more likely in patients aged 40 years or older (p < 0.05).
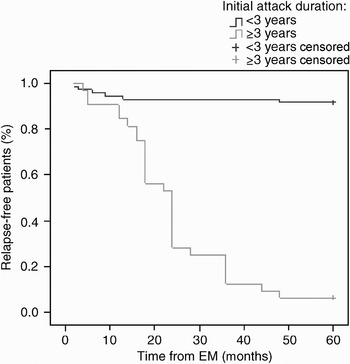
Fig. 2 Kaplan–Meier curves for effect of initial duration of benign paroxysmal positional vertigo (BPPV), prior to initial Epley's manoeuvre (EM) treatment, on BPPV recurrence over the five-year follow-up period. Recurrence was significantly more likely in patients with three or more years of BPPV attacks prior to initial EM (p < 0.001).

Fig. 3 Kaplan–Meier curves for effect of number of initial benign paroxysmal positional vertigo (BPPV) exacerbations, prior to Epley's manoeuvre (EM) treatment, on BPPV recurrence over the five-year follow-up period. Recurrence was significantly more likely in patients with six or more exacerbations prior to initial EM (p < 0.001).
After one year's follow up, 93 per cent of patients reported a subjective complete cure of BPPV. After five years' follow up, this had fallen to 65 per cent (Table IV).
Table IV Patients' overall subjective health after one- and five-year follow up

Discussion
Demographic data for the study group were concordant with previously published data.Reference Macias, Lambert and Massingale11, Reference Radtke, von Brevern, Tiel-Wilck, Mainz-Perchalla, Neuhauser and Lempert12
EpleyReference Epley3 reported an 80 per cent success rate for the Epley manoeuvre, following one week review. Parnes and Price-JonesReference Parnes and Price-Jones13 reported a 79 per cent success rate after three to four weeks' review, while Herdman et al. Reference Herdman, Tusa and Zee5 reported a 90 per cent success rate after two weeks' review. The current study results for short-term follow up are comparable with these reports. The apparently greater success rate (92 per cent subjective cure) in the current study (Table II) may be due to the fact that Epley's manoeuvre was offered only to those patients having a typical history of BPPV, plus nystagmus in the Dix–Hallpike position. Also, treatment was delayed for one month after commencement of the attack, in order to effect separation of loose particles from the otoconia. Repeated used of Epley's manoeuvre in those patients suffering recurrence of BPPV (after an initial post-treatment improvement) increased the success of this treatment to 93 per cent at one-year follow up. This points to the importance of follow up in these patients. Radtke et al. Reference Radtke, von Brevern, Tiel-Wilck, Mainz-Perchalla, Neuhauser and Lempert12 reported success rates ranging from 70 per cent (after a single application of Epley's manoeuvre) to nearly 100 per cent (after repeated application), on short-term follow up.
Ninety-three per cent of the present patient cohort had either no further attacks (65 per cent) or only minor attacks requiring no medical advice (28 per cent). Prokopakis et al. Reference Prokopakis, Chimona, Tsagournisakis, Christodoulou, Hirsch and Lachanas10 reported a 92 per cent subjective success rate after a mean follow up of 46 months. Eighty-six per cent of the present patient cohort reported either a subjective complete cure (65 per cent) or major improvement (i.e. more than 50 per cent; 21 per cent), over the five-year follow-up period. The difference between the current results and those of Prokopakis and colleagues may be due to the current study's longer follow-up period (five years).
All current patients with no or only minor attacks during five-year follow up (i.e. successful Epley's manoeuvre) had a negative Dix–Hallpike test on five-year re-examination. However, only two of those patients suffering major attacks over the five-year follow-up period had a positive Dix–Hallpike test on five-year re-examination. These two patients had negative ENG results. This may be due to the fact that ENG is unable to detect the torsional component of nystagmus typical of posterior canal BPPV.Reference Minor, Zee and Hurley14
• This study aimed to assess the long-term efficacy of Epley's manoeuvre for benign paroxysmal positional vertigo (BPPV)
• Epley's manoeuvre was an effective modality of treatment for BPPV. Patient age younger than 40 years and pre-treatment duration of attacks of less than three years were good prognostic factors
• Duration of illness prior to Epley's manoeuvre treatment was the only independent predictor of BPPV recurrence
The effect of the possible prognostic factors (i.e. patient age, sex, duration of BPPV attacks before initial treatment, and number of BPPV exacerbations before initial treatment) was analysed using logistic regression, Kaplan–Meier testing, and univariate and multivariate analysis. The time to BPPV recurrence was significantly longer among: patients aged less than 40 years (compared with those aged 40 years or more); patients with less than three years of BPPV attacks before initial Epley's manoeuvre treatment (compared with those with three or more years of BPPV attacks); and patients with less than six exacerbations of BPPV before initial Epley's manoeuvre treatment (compared with those with six or more exacerbations) (Table III). Gender had no effect on time to recurrence. Kaplan–Meier curves confirmed the same results (Figures 1 to 3). A literature search revealed no prior publications describing the time to BPPV recurrence after such long-term follow up of Epley's manoeuvre. Univariate analysis of these predictors of recurrence showed that both age ≥40 years and initial BPPV duration of attacks of ≥ three years were associated with a higher incidence of recurrence. Sex and number of initial BPPV exacerbations were not predictors (Table III). This means that an initial number of BPPV exacerbations of six and more does not affect the probability of BPPV recurrence, but it does affect the duration of time to BPPV recurrence. Brandt et al. Reference Brandt, Huppert, Hecht, Karch and Strupp15 reported that recurrences were seen significantly more often in women (58 vs 39 per cent). This finding was not observed in the current study. Brandt et al. also reported that the BPPV recurrence rate was higher in patients in their seventh decade than in other age groups. Brandt et al. suggested that, in their patients, a history of three or more BPPV attacks prior to treatment might be an indicator for BPPV recurrence.
If one considers that subjective improvement and acceptable patient satisfaction is present in those patients with either complete improvement or more than 50 per cent improvement, then subjective improvement was present in 86 per cent of the current patients, five years after Epley's manoeuvre treatment. Lopez-Escamez et al. Reference Lopez-Escamez, Gamiz, Fernandez-Perez and Gomez-Fiñana16 reported that the effectiveness of Epley's manoeuvre was 88 per cent after one-year follow up.
Prior to initial Epley's manoeuvre treatment, the current patients' duration of BPPV ranged from four to 96 weeks, with a mean duration of 27.7 and SD of 21.7 weeks. Multivariate logistic regression revealed that pre-treatment duration of illness was the only independent predictor of recurrence. Patients with a pre-treatment BPPV duration of three years or more were 162.5 times more likely to experience recurrence, compared with those with a BPPV duration of less than three years. This may be explained by the theory that patients with longer durations of BPPV may have degenerative processes resulting in frequent and persistent separation of particles from the otoconia. However, a literature search revealed no published data addressing the relationship between initial BPPV duration or the number of BPPV exacerbations and the BPPV recurrence rate.
Conclusions
Epley's manoeuvre remains an effective treatment modality for patients with BPPV, even after a long duration of illness. In the current study, a patient age of ≥40 years and a pre-treatment duration of BPPV attacks of ≥ three years were associated with a higher chance of recurrence. The number of pre-treatment BPPV exacerbations and the patient's sex did not affect the probability of recurrence over five years; however, they did affect the duration of time free from BPPV. The duration of illness prior to initial treatment was the only independent predictor of recurrence.
Acknowledgement
I am deeply grateful to Professor Abdel-Hady El-gilany MD, Professor of Public Health and Biostatistics, College of Medicine, King Faisal University, Saudi Arabia, for his great effort in undertaking the statistical analysis and arranging the table of this article.
Appendix 1. Patient questionnaire
Name:
Age:
Sex:
Duration of complaint before Epley's manoeuvre treatment:
Number of exacerbations before Epley's manoeuvre treatment:
Results after Epley's manoeuvre:
– No attacks
– Mild attacks, no consultation required
– Major attacks requiring consultation and repeat manoeuvre
Overall subjective feeling:
– Complete resolution of problem
– >50% improvement
– <50% improvement
– No improvement
– Getting worse







