Introduction
Any scar tissue developing in the middle ear is referred to as tympanosclerosis, a term frequently used to refer to scarring of the tympanic membrane. A more appropriate term for the latter is myringosclerosis.Reference Gray, Lusk, Cummings, Fredrickson, Harker, Krause and Schuller1 Myringosclerosis is supposed to represent the end stage of the inflammatory process. During the acute stage of inflammation, fibrocytes invade the lamina propria of the eardrum and then decompose and hyalinise; this is followed by calcification and the formation of characteristic myringosclerotic plaques.Reference Gray, Lusk, Cummings, Fredrickson, Harker, Krause and Schuller1
Hyalinisation and calcification can occur in any part of the subepithelial connective tissue of the tympanic membrane and middle ear; however, bone deposition and ossicular fixation are found most frequently in the attic, and include the heads of the malleus and incus.Reference Chole, Sudhoff, Cummings, Flint, Haughey, Robbins and Thomas2 Myringosclerosis may frequently be found in association with tympanic membrane perforation. Certain factors can influence the short- and long-term success of tympanoplastic surgery, such as the patient's age, perforation size and location, involvement of tympanic membrane margins, and status of the contralateral ear.Reference Kessler, Potsic and Marsh3, Reference Brodsky, Pizzuto, Nagy, Poje and Carr4,Reference Vlastarakos, Nikolopoulos, Korres, Tavoulari, Tzagaroulakis and Ferekidid5 Regardless to its cause, myringosclerosis has been found to have little effect on hearing. There are no reports indicating the effect of sclerotic plaque removal on tympanoplasty outcomes.
The current study analysed the success rate of tympanoplasty for perforated eardrums in paediatric patients who had coexisting myringosclerosis confined to the tympanic membrane.
Method
A retrospective study was conducted on 40 children who had been referred to the out-patient clinic, who had undergone primary tympanoplasty, and in whom myringosclerosis had been found on primary otoscopic examination and confirmed at surgery.
The study was designed after several surgical failures had occurred in patients with myringosclerosis whose sclerotic plaques had not been removed. Due to this observation, when designing this study we considered it unethical to leave sclerotic plaques in situ for research purposes only. Thus, the control group for this study included 34 children who had undergone primary tympanoplasty and whose tympanic membrane was free of myringosclerosis.
The study and control groups were well matched in terms of age, gender, pre-operative hearing status, and perforation location and size. Patients were followed up for at least 12 months. Their medical records were reviewed for: age; cause; perforation size (i.e. small, medium or large, being 25, 50 or 75 per cent of the tympanic membrane area, respectively); perforation location (central or marginal); surgical findings (i.e. site and size of myringosclerotic plaques, status of ossicular chain and presence of tympanosclerosis); audiological findings before and after surgery (i.e. air conduction and air–bone gap for 500, 1000, 2000 and 4000 Hz, and speech reception threshold); and surgical outcome (i.e. closed eardrum, residual perforation or re-perforation).
All primary tympanoplasty procedures were routinely performed transmeatally, with a temporalis fascia graft having been harvested (through a small supra-auricular incision) and placed medial to the tympanic membrane remnants, utilising the underlay technique. The three revision procedures were also performed transmeatally, and tragal perichondrium was used in the underlay technique in all these cases. Sclerotic plaques were meticulously removed, along with maximal conservation of the outer layer of the tympanic membrane. Enlargement of the tympanic membrane defect depended on the size of the removed plaques, and the graft used to repair the sclerotic tympanic membrane was larger than that used to repair a perforation without coexisting myringosclerosis.
Patients were examined at least four times post-operatively, i.e. at two weeks and at two, six and 12 months after surgery.
Surgical success was defined as the perforation remaining closed 12 months after surgery.
Pure tone audiometry was routinely performed pre-operatively and two and 12 months post-operatively.
Results
The study group included 40 children (23 girls, 17 boys; age range six to 16 years, mean age 9.85 years) with 13 large, 22 medium-sized and five small perforations; 21 perforations were central and 19 were marginal.
Sclerotic plaques occupied the whole remnant tympanic membrane in 15 (37.5 per cent) patients, and were located anterior to the perforation margins in eight, anteroposterior in eight, anterosuperior in four and posterior in five. Tympanosclerosis associated with myringosclerosis was found in six (15 per cent) children. Tympanosclerotic plaques were located on the ossicles in all these six children, and were also present on the promontory in one child. All ossicles were fixed in two patients.
It should be noted that the study children underwent only myringoplasty, without interventions for any existing ossicular chain problem.
Post-operatively, two children had delayed healing of tympanomeatal flap margins. A small cholesteatoma pearl was removed from the eardrum in another two children, eight and 12 months after initial surgery. One child presented with bullous myringitis and acute otitis media 21 months after surgery, and was successfully treated with a one-week course of amoxicillin clavulanate, which led to complete resolution of the middle-ear infection.
Three children had residual perforations; Table I lists their characteristics. All three of these children successfully underwent revision procedures for their residual tympanic membrane defects, four, eight and 10 months after the initial procedure (cases three, two and one, respectively).
Table I Characteristics of 3 children with residual perforation

No = number; yrs = years; perf = perforation; MS = myringosclerosis; F = female; med = medium; marg = marginal; ant = anterior; post = posterior; TM = tympanic membrane
Primary tympanoplasty failed in two children of the control group (5.9 per cent); one presented with a medium-sized, central perforation and the other with a small anterior tympanic membrane defect. Both children underwent successful revision surgery using tragal perichondrium, eight and 10 months after their primary procedure, respectively.
Pure tone audiography in the study group children showed that the mean pre-operative air conduction, air–bone gap and speech reception threshold results were respectively 25 ± 12.5, 18 ± 16.1 and 20 ± 5.0 dB, while the post-operative results were respectively 20 ± 12.0, 18 ± 10.3 and 18 ± 5.0 dB. No study group patients demonstrated worsening of hearing after surgery. Overall, 27 of the 40 (67.5 per cent) patients demonstrated a post-operative speech reception threshold of 20 dB or better and had a post-operative mean air–bone gap of 20 dB or less.
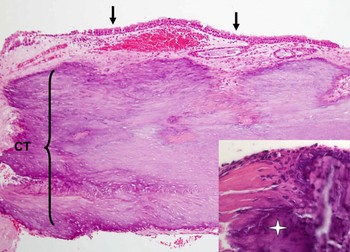
Histopathological analysis of the removed sclerotic plaques demonstrated hyaline sclerosis of the tympanic membrane lamina propria. In all study group patients, the tympanic membrane was found to be almost entirely replaced by dense, avascular, heavily hyalinised connective tissue with calcifications in the sclerotic area (Figure 1).

Fig. 1 Photomicrograph of tympanic membrane from a study group child. The tympanic membrane consists of an inner cuboidal epithelial layer covering (arrows) over dense, markedly hyalinised connective tissue (CT). Inset shows focal calcification (star) present in the lamina propria.
Discussion
It is now generally accepted that tympanoplasty can be successfully performed in young patients in the presence of well functioning eustachian tubes. The findings of the present study indicated that primary tympanoplasty was surgically successful in 92.5 per cent of children with concomitant myringosclerosis, compared with 94.1 per cent of a control group (p = 0.332). These results were comparable with those reported by other authors.Reference Kessler, Potsic and Marsh3, Reference Brodsky, Pizzuto, Nagy, Poje and Carr4, Reference Vrabec, Deskin and Grady6, Reference Umapathy and Dekker7 Notably, all three surgical failures were observed in girls with marginal perforations. However, the difference in success rate was not related significantly to gender (p = 0.122) or perforation location (p = 0.058).
The current study had some limitation. Theoretically, the controls should have comprised patients whose sclerotic plaques remained untouched. However, this was considered unethical. Thus, surgical success in the study group was compared with that in children who had undergone primary tympanoplasty and whose eardrums were free of sclerotic plaques.
Acute otitis media is the most common bacterial infection in the general paediatric population, and young children suffer middle-ear infections more frequently than others (aged >3 years). As the age limits of paediatric tympanoplasty decrease, acute infection of the middle ear poses potential problems in the operated children. In the current series, one child suffered a post-operative middle-ear infection and bullous myringitis following an upper respiratory tract infection; a one-week course of amoxicillin clavulanate resulted in complete resolution. The eardrum remained closed.
Umapathy and DekkerReference Umapathy and Dekker7 reported a 90 per cent perforation closure rate in children aged four to 14 years, but this figure dropped to 88 per cent due to the development of glue ear in two patients. These authors did not specify any existing pathological findings during the surgery, and it was not clear if any of their patients had additional myringosclerosis.
Special attention should be paid to children with chronic rhinitis, which may cause eustachian tube dysfunction and result in re-perforation after successful tympanoplasty. In the present series, a small cholesteatoma pearl was seen to have developed in two children. The fact that this complication was discovered eight and 12 months after tympanoplasty makes long-term surgical follow up mandatory.
• This study analysed the success rate of tympanoplasty for perforated tympanic membrane in children with coexisting myringosclerosis confined to the tympanic membrane
• A retrospective study was conducted on 40 children who had undergone primary tympanoplasty
• Surgery involved removal of the sclerotic plaque from the tympanic membrane remnant. The success rate of primary tympanoplasty was 92.5 per cent
• Appropriate freshening of the perforation edges, with removal of sclerotic plaque, can result in a high rate of successful closure of perforated tympanic membrane with coexisting myringosclerosis
Good vascularisation of tympanic membrane remnants is essential for successful tympanoplasty – otherwise, the free graft used to close the defect will become necrotic and may disappear. Hyalinisation and the development of myringosclerosis result in hypovascularity of the tympanic membrane, which can lead to the failure of even well performed tympanoplasties. Since adequate refreshing of the perforation edges is impossible in the presence of sclerotic plaques, we recommend removing these plaques. This procedure usually enlarges the eardrum defect; a larger graft is thus required.
Conclusions
Appropriate freshening of the tympanic membrane perforation edges, with removal of sclerotic plaques, can lead to a high rate of surgical success (92.5 per cent) for closure of tympanic membrane defects with coexisting myringosclerosis. Long-term surgical follow up is mandatory in paediatric patients who undergo tympanoplastic surgery, because of the possibility of late re-perforation and cholesteatoma formation.