


Introduction
Assessment of the electrically elicited stapedius reflex threshold provides useful assistance during initial setting of the cochlear implant speech processor, especially in young children and uncooperative, multi-morbid or long-term deafened patients. There is well known correlation between the stapedius reflex threshold and the maximal comfort level for speech understanding (i.e. the C-level).Reference Stephan and Welzl-Müller1–Reference Wolfe and Kasulis6
Most surgeons use intra-operative visual observation of stapedius muscle contraction during electrical stimulation to determine the stapedius reflex threshold. However, does the first visible movement of the tendon reflect the true stapedius reflex threshold, or is the actual threshold somewhat lower but not visually detectable by the observer? This question is particularly prompted by the fact that reflex thresholds determined post-operatively, after the healing phase, are generally lower. Furthermore, intra-operative thresholds vary rather widely.Reference Allum, Greisiger and Probst2
Of course, this can potentially be explained by the effect of narcotics used during surgery, which have a significant impact on stapedius muscle contractions.Reference Makhdoum, Snik, Stollman, de Grood and van den Broek7–Reference Crawford, White, Propst, Zaarour, Cushing and Pehora9 However, there may be another factor: the intra- and post-operative reflex thresholds are usually measured by two different techniques. Intra-operatively, visual observation is the method of choice; post-operatively, however, changes in middle-ear impedance are used to indirectly indicate stapedius muscle contractions.
Visual observation may be influenced by subjective factors, and it may be difficult to identify slight contractions accurately. In contrast, tympanometric measurements yield more objective results.
Ideally, identical methods should be used to compare intra- and post-operative stapedius reflex thresholds.
In the present study, we estimated intra-operative thresholds both visually and tympanometrically, in order to assess any differences. Intra-operative stapedius reflex thresholds were also compared to post-operative thresholds measured tympanometrically.
Materials and methods
The study assessed six consecutive patients receiving a cochlear implant (four Nucleus Freedom® devices (Cochlear, Sydney, Australia), one Pulsar® device (Med-El, Innsbruck, Austria) and one Sonata® device (Med-El, Innsbruck, Austria)). Intra-operative measurement of electrically elicited stapedius reflexes was performed using two methods: visual observation and tympanometry.
The first method used visual observation of stapedius muscle contractions to determine the stapedius reflex threshold.
Subsequently, we used tympanometry, a technique which has become established for post-operative measurement of stapedius reflex thresholds. Prior to commencing surgery, a plug was inserted into the patient's ear canal and connected to a tympanometer (a version 2 GSI TympStar middle-ear analyser; Grason-Stadler, Conshohocken, Pennsylvania, USA). We used the same mode as for acoustic reflex decay measurements. While this function was activated, electrical stimulation was performed on certain channels of the cochlear implant. During measurements, care was taken to minimise the noise level in the operating theatre. In the case of a positive response, the resulting curve on the tympanometer screen showed a typical peak, indicating an impedance change due to stapedius muscle contraction. By reducing the stimulus, a threshold was established below which no more peaks were recorded.
Tympanometric measurements were performed on a number of electrodes, and compared to visually determined reflex threshold results.
In three of our patients, additional reflex threshold recordings were performed seven weeks after surgery, providing a comparison between intra- and post-operative thresholds determined on single electrodes.
Results
In general, the visually and tympanometrically determined thresholds were almost identical (Figure 1a). In two cases, the visually determined threshold curve was slightly higher than the tympanometrically determined curve (Figure 1b), while in another two cases we observed the opposite effect (Figure 1c). Twenty-two electrodes were tested in the six patients. The difference between the visually and tympanometrically determined thresholds was calculated for each electrode, and the mean difference calculated for all channels tested. The mean difference was 0.06 ± 0.26 charge units – a minimal amount.
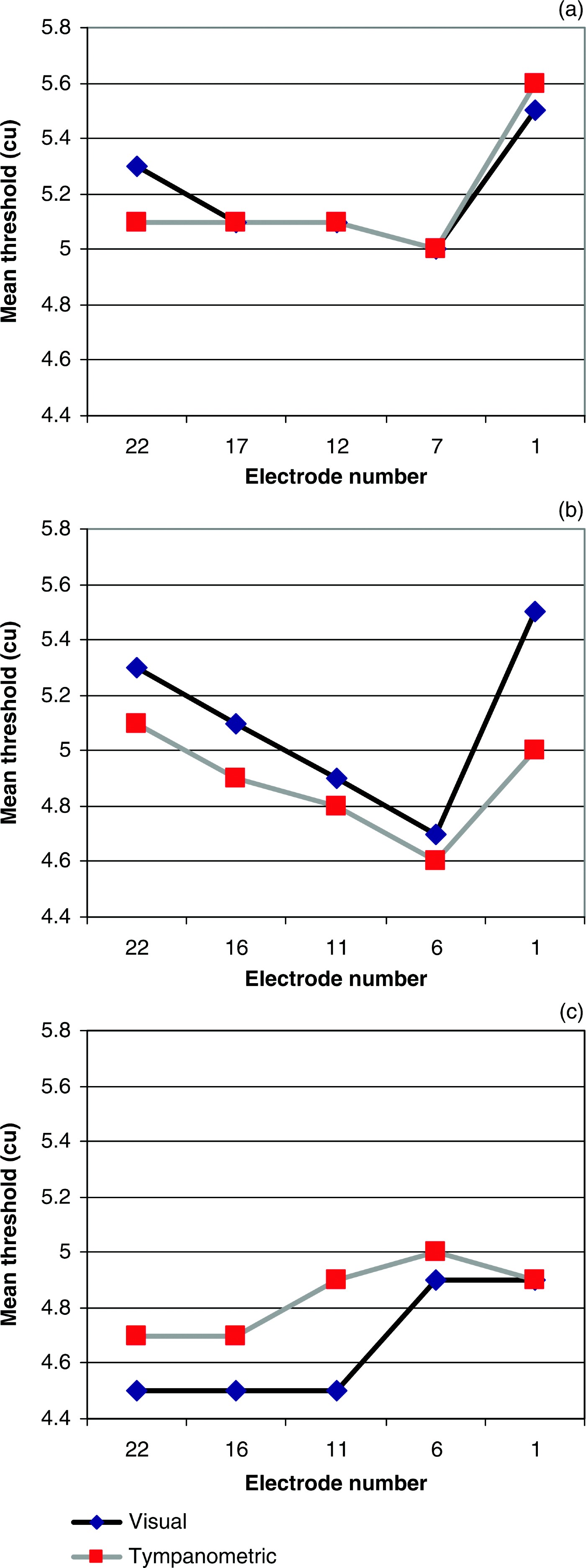
Fig. 1 Comparison of electrically stimulated stapedius reflex threshold patterns determined visually and tympanometrically: (a) almost identical threshold curves; (b) slightly higher threshold curve for visual vs tympanometric assessment; (c) slightly lower threshold curve for visual vs tympanometric assessment. cu = charge units
In contrast, we observed a distinct difference between intra- and post-operative reflex threshold measurements performed with the same technique (impedance measurement) on single channels: the post-operative thresholds were lower. As this effect is known from the literature, we only tested seven electrodes in three patients. The mean difference between the intra- and post-operative reflux thresholds was 1.17 ± 2.35 charge units.
Due to the small number of patients, no statistical analysis was planned or performed.
Discussion
Our results clearly indicate that the difference between intra- and post-operative stapedius reflex thresholds is not caused by different measurement techniques. This is unsurprising, but confirmation of the fact is useful.
We performed the study because we were unsure whether visual assessment of the stapedius reflex threshold was sufficiently accurate. Cochlear implant surgeons will be well aware of the difficulty of deciding whether a muscle contraction has been observed or not. In ideal situations, this decision is very easy. However, problems may arise if there is bleeding or scar tissue in the middle ear, especially around the tendon. Sometimes, contractions appear to be slower and later than usual, raising difficulties. In such cases, we hypothesised that impedance measurement via a tympanometer may give a different and more reliable threshold. This was obviously not the case.
• This study compared the accuracy of electrically elicited stapedius reflex threshold determination via visual assessment (of stapedius muscle contraction) versus tympanometry (assessing impedance changes), during cochlear implantation surgery
• No substantial differences were found between intra-operative thresholds measured using these two techniques
• Intra-operative electrically elicited stapedius reflex threshold measurements may give an approximate indication which aids initial setting of the cochlear implant speech processor, to help avoid over-stimulation, especially in young children and in unco-operative, multi-morbid or long-term deafened patients
We also took additional electromyographical measurements via a bipolar needle introduced into the stapedius muscle, which yielded similar results, that is, reflex thresholds recorded visually and electromyographically were in the same range.Reference Pau, Zehlicke, Sievert, Schaudel, Behrend and Dahl10 These findings were in good accordance with those of Clemen and Kipke (in rats) and Almquist et al. (in humans).Reference Clement and Kipke11, Reference Almquist, Harris and Shallop12
As assumed by many authors, narcotics given during surgery may influence the stapedius muscle reflex and cause threshold shifts.
We emphasise that – in contrast to post-operative threshold measurements – intra-operative stapedius reflex threshold measurements are not especially suitable for preliminary setting of speech processors; however, they may give an approximate value, facilitating the avoidance of over-stimulation, especially in young children and in uncooperative, multi-morbid or long-time deafened patients.

