Introduction
Mucoceles are benign, expansile, cyst-like lesions of the paranasal sinuses.Reference Canalis, Zajtchuk and Jenkins1 The mucoid secretions of mucoceles are usually sterile. However, secondary infections, mostly bacterial, may lead to the development of pyocoeles. In contrast, mucoceles with superimposed fungal infections are extremely rare.
We report an extremely rare case of a fungus ball within a mucocele of the sphenoid sinus and infratemporal fossa.
Case report
A 62-year-old woman with a benign medical history, including no history of allergies, was referred for evaluation of a mass lesion in the left sphenoid sinus and infratemporal fossa. There was no history of nasal surgery, and the patient did not complain of sinus symptoms.
The patient's visual acuity and fields were normal bilaterally. Laboratory investigations, including allergy tests, were normal. Endoscopic examination of the nasal cavity was unremarkable, with the exception of a slight fullness of the anterior wall of the sphenoid.
Computed tomography (CT) scanning of the paranasal sinuses revealed a large, expansile, low-attenuation mass in the sphenoid sinus, which had broken into the left infratemporal fossa, and which consisted of subtle, high-density material containing calcifications (Figure 1).

Fig. 1 Axial (a) and coronal (b) computed tomography scans showing a large, expansile, low-attenuation mass in the sphenoid sinus (white arrows) which has broken into the left infratemporal fossa, and which consists of subtle, high-density material containing calcifications.
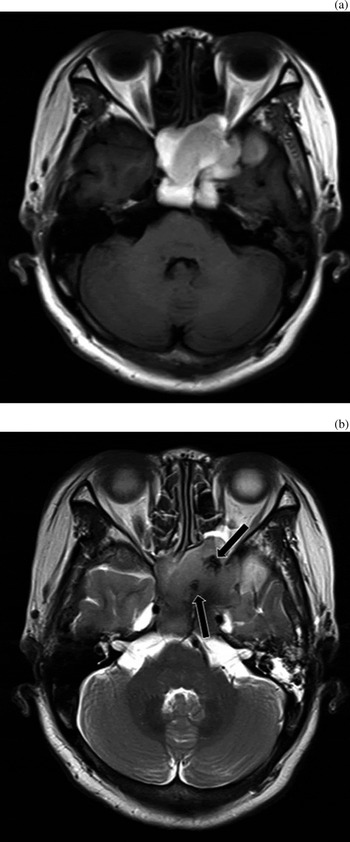
Axial T1- and T2-weighted magnetic resonance imaging (MRI) scans showed a multi-lobulated, expansile, non-homogeneous sphenoid sinus mass (Figure 2). The mass had high T1-weighted and intermediate T2-weighted signal intensities. The T2-weighted scan showed a hypointense signal within the sphenoid sinus mass.

Fig. 2 Axial T1-weighted (a) and T2-weighted (b) magnetic resonance imaging scans showing a multi-lobulated, expansile, non-homogeneous sphenoid sinus mass. The mass has high T1-weighted signal intensity and intermediate T2-weighted signal intensity. The T2-weighted image shows a hypointense signal within the sphenoid sinus mass (black arrows).
The pre-operative diagnosis was a mucocele with high protein content.
At operation, after widening of the mucocele wall via a sphenoidotomy and trans-pterygopalatine fossa approach, we discovered a large amount of a yellow, purulent secretion, together with a cheesy, clay-like material suggestive of fungus (Figure 3). The fungus ball and mucous secretions were successfully drained endoscopically.
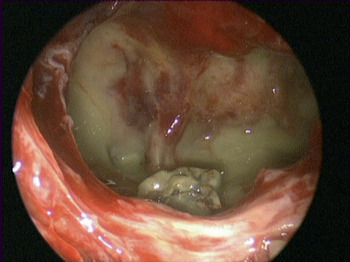
Fig. 3 Intra-operative endoscopic view showing a fungus ball and yellow secretions, within a mucocele of the sphenoid sinus and left infratemporal fossa.
Histopathological examination of the cheesy, clay-like material was consistent with an aspergilloma. This case was diagnosed as a fungus ball within a mucocele of the sphenoid sinus and infratemporal fossa.
The post-operative course was uneventful.
This report was approved by the institutional review board of Chonnam National University Hospital.
Discussion
A mucocele is an expansile lesion of the paranasal sinuses. Mucoceles with a superimposed fungus ball are extremely rare. The coexistence of a fungus ball within a mucocele can be explained by the hypothesis that the fungus ball within the sinus causes recurrent infections, which leads to obstruction of the sinus ostium and the development of a mucocele.
Although Ishibashi and Kikuchi have reported MRI findings for an aspergilloma within a sphenoid sinus mucocele, the radiological findings of this case were not discussed in detail.Reference Ishibashi and Kikuchi2
The differential diagnosis of expansile cystic lesions includes mucocele, allergic fungal sinusitis, cholesterol granuloma and cystic schwannoma.
In allergic fungal sinusitis, CT scans show mixed high and low attenuation in the involved sinus, and frequent bony erosion.Reference Sun and Elluru3 Areas of highly attenuated CT signal correspond to fungal and mucous material. On MRI scanning of allergic fungal sinusitis, T1-weighted images typically reveal a low signal intensity, but high signal intensity or mixed signal intensities are also frequently observed.Reference Aribandi, McCoy and Bazan4 The T2-weighted images are generally hypointense or signal-void, suggesting the presence of fungal organisms together with a low concentration of free water within any mucous material. Enhancement of T1-weighted images with gadolinium contrast also demonstrates peripheral mucosal enhancement.
Mucoceles often present as homogeneous opacifications on CT, hypointense lesions on T1-weighted MRI, and hyperintense lesions on T2-weighted MRI. In contrast-enhanced MRI images, the sinus mucosa enhances as a thin line surrounding the mucocele. However, the MRI appearance of mucoceles varies depending on their protein concentration, which changes over time.
Cholesterol granulomas show high signal intensity on both T1- and T2-weighted MRI images, due to the paramagnetic effect of methaemoglobin and granulations.Reference Kang, Kim and Kim5 Although mucoceles with high concentrations of protein may appear similar to cholesterol granulomas on T1-weighted MRI images, mucoceles have a lower signal intensity on T2-weighted scans, compared with cholesterol granulomas. Similarly to our case, the association of cholesterol granulomas and aspergilloma within the maxillary sinus has been reported.Reference Kang, Kim and Kim5, Reference Sarioglu, Pabuççuoglu and Arzu Topal6
Cystic schwannomas involving the sphenoid sinus are very rare.Reference DiNardo and Mellis7 Depending on the degree of cystic degeneration, cystic schwannomas show variable enhancement on contrast-enhanced CT and MRI scans. Thus, the solid, enhancing portion within the tumour, and the bright signal intensity of the cystic component on T2-weighted MRI images, enable differentiation of cystic schwannomas from other diseases.
In our case, the contrast-enhanced CT showed a cystic, lobulated, relatively homogeneous, low-attenuation, thin-walled, peripherally enhancing lesion of the sphenoid and infratemporal fossa, with calcifications and bony erosion. Because an increased central density on CT images is one of the characteristic findings of allergic fungal sinusitis, the low attenuation of the mass on non-enhanced CT made a diagnosis of allergic fungal sinusitis less likely. Magnetic resonance imaging showed a mass with a high signal intensity on T1-weighted images and an intermediate signal intensity on T2-weighted images. Based on radiological findings, a mucocele with a high protein content was initially suspected; however, the focal, low-signal intensities seen within the mass on T2-weighted images presented a diagnostic challenge.
During surgery, clay-like material was noted within the mucocele, which corresponded to the hypointense signal seen on T2-weighted images; this material was diagnosed as aspergillus on histopathological examination.
On MRI, fungus balls have been described as having hypointense or intermediate signal intensity on T1-weighted images, and having low or no signal intensity on T2-weighted images.Reference Ishibashi and Kikuchi2, Reference Eggesbø8 However, the signal intensity of the fungus ball on T1-weighted images may be impossible to differentiate from the signal intensities of surrounding material, as was the case in our patient. In this case, T2-weighted images helped to differentiate between fungus concretions (giving a hypointense signal) and mucosal swelling or low-protein mucous retention (giving a hyperintense signal).
As mucoceles and allergic fungal sinusitis can have similar imaging findings, fungal allergy tests are helpful in the differential diagnosis.
Intrasinus materials with similar MRI findings to fungus balls include air, desiccated secretions, acute haemorrhage, calcium, bone and enamel.Reference Som, Dillon, Curtin, Fullerton and Lidov9 Necrotic, inspissated material with a hypointense signal on T2-weighted imaging may be found within mucoceles.Reference Ishibashi and Kikuchi2
• Mucoceles with superimposed fungal infection are extremely rare
• Computed tomography and magnetic resonance imaging facilitate the diagnosis of fungal ball within a mucocele of the paranasal sinus
• The treatment of choice is drainage and restoration of sinus ventilation
Any pre-operative suggestion of a fungal infection is valuable, as it alerts the surgeon to request serological and histopathological evaluation of removed material; this is crucial for excluding allergic or invasive fungal sinusitis.
The treatment of choice for fungus balls within a mucocele is drainage and restoration of sinus ventilation. The endoscopic approach has the advantages of easy access to the affected sinus, perfect sinus visualisation and low morbidity. In our patient, sphenoidotomy and a trans-pterygopalatine fossa approach enabled successful endoscopic drainage of the fungus ball and purulent secretions.