


Introduction
The sensory innervation of the external auditory canal is complex and supplied by multiple nerves. One of these nerves can be encountered during otological surgery procedures, when gradually thinning the posterior canal wall, and may initially be mistaken as the origin of the chorda tympani. This nerve supplies the sensory innervation to the posterior external auditory canal. Coughing during ear wax removal, neuralgic pain, vesicular eruptions described in Ramsay Hunt's syndrome and hypoesthesia from acoustic neuromas (Hitselberger's sign) are all attributed to this area.Reference Hitselberger and House 1 – Reference Hunt 4
Although this nerve seemed to originate from the mastoid segment of the facial nerve, anatomical schematic descriptions suggest that these fibres travel with the auricular branch of the vagus nerve (Arnold's nerve) before innervating the posterior external auditory canal.Reference Schuknecht 5 , Reference Lang 6 Morphological documentation and correlation of this entity in humans remain vague. A review of the original literature, cadaveric specimen dissections and histological analysis, and our clinical cases, guided us to reconsider the clinical impact of this nerve.
Methods and results
Our routine approach in cochlear implant surgical procedures is an anterior mastoidectomy, with identification and skeletonisation of the facial nerve from the stylomastoid foramen towards the second genu, before opening the facial recess.
Drilling close to the mastoid portion of the facial nerve and thinning the posterior canal wall, we encountered a small nerve exiting the Fallopian canal in the distal half of the mastoid segment in the majority of cases. The nerve typically appears caudal to the origin of the chorda tympani, travels laterally and superiorly, before bending inferiorly and anterolaterally. It therefore has a distinctly different course from the chorda, which also leaves the Fallopian canal but courses directly anterosuperiorly towards the middle ear.
In a recent patient with intractable otalgia, and another with severe coughing whilst inserting a hearing aid, who both had a temporary response to local anaesthesia, we sectioned this sensory branch along the posterior canal wall, and became more interested in the true origin of these fibres.
Clinical cases
A 50-year-old woman was referred with a 3-year history of severe and persistent left-sided otalgia localised along the concha and posterior canal wall. After eliminating other causes, the diagnosis of ‘idiopathic neuralgia’ was made. After injecting 2 cc of 1 per cent lidocaine solution to the concha and posterior canal wall, the pain immediately resolved. She underwent an anterior mastoidectomy. The sensory branch to the external auditory canal was identified, removed from its canal and transected over a 5 mm length (Figure 1a). Bone wax was then applied to close the previous bony canal in order to prevent reinnervation. Initially, slight dysaesthesia at the concha was noted, but without pain. Three years post-operatively, the patient remained pain-free.

Fig. 1 Sensory branch (arrowheads) on the posterior canal wall in: (a) left-sided intractable otalgia case (facial nerve is outlined), and (b) right-sided coughing case. FN = facial nerve; SS = sigmoid sinus
Another case involved a 77-year-old gentleman with severe attacks of coughing when cleaning his ear canal and upon inserting the ear mould of his conventional hearing aid. The irritation immediately disappeared upon administration of local anaesthesia to the posterior canal wall and cavum conchae. At the beginning of surgery, the removal of cerumen immediately dropped his pulse rate to 24 per minute, with gradual recovery. Following anterior mastoidectomy, the sensory branch appeared as a dominant nerve one-third the size of the facial nerve at the typical site (Figure 1b). Once drilled out of its bony canal, 5 mm were resected, and the distal stump was coagulated and covered by bone dust and fascia (this is demonstrated in a short video, available on The Journal of Laryngology & Otology website; Appendix 1). At the end of surgery, further cleaning of the ear canal did not induce any change in pulse rate. Ten days after surgery, the hearing aid could be inserted without disturbances.
Temporal bone dissection
In a temporal bone specimen, we skeletonised the facial nerve at the stylomastoid foramen, gradually thinned the posterior canal and identified the sensory nerve exiting the Fallopian canal, as mentioned above. Next, an open mastoido-epitympanectomy, and bony decompression of the facial nerve, chorda tympani and sensory nerve was achieved. The main bundle of this nerve was travelling further inferomedially, whilst a small fibre from the facial nerve trunk joined this nerve (Figure 2). We further followed this sensory nerve to the jugular bulb.

Fig. 2 Left-sided temporal bone specimen showing the origin of the sensory branch (arrowheads) to the posterior external auditory canal. (a) Photographic view showing the relationship of the sensory branch with the chorda tympani and facial nerve. (b) Photographic view showing the origin of the sensory nerve coming from the dome of the jugular bulb. (c–d) Endoscopic views of the sensory branch (arrowheads, outlined) and fibres from the facial nerve. FN = facial nerve; CT = chorda tympani; JB = jugular bulb; SS = sigmoid sinus
To reveal its origin, we rerouted the facial nerve, exposed the internal carotid artery and jugular bulb, and identified the lower cranial nerves. We confirmed that the sensory branch was a continuation of the auricular branch of the vagus nerve (Arnold's nerve) by following the nerve into the vagus nerve at the pars nervosa of the jugular foramen. It was also joined by fibres from the glossopharyngeal nerve just proximal to its inferior ganglion (Figure 3).

Fig. 3 Left-sided temporal bone specimen after anterior rerouting of the facial nerve; the internal carotid artery (ICA) and jugular bulb (JB) were exposed. The relationship of the auricular branch of the vagus nerve (Arnold's nerve is outlined) with the inferior ganglion of the glossopharyngeal nerve (IXth cranial nerve (IX)) can be seen. RW = round window; LSC = lateral semicircular canal; PSC = posterior semicircular canal; X = vagus nerve; ICV = inferior condylar vein; SS = sigmoid sinus
Histology
Serial sectioning, and haematoxylin and eosin staining of the facial nerve with the Arnold's nerve confirmed communicating fibres between the two nerves (Figure 4).
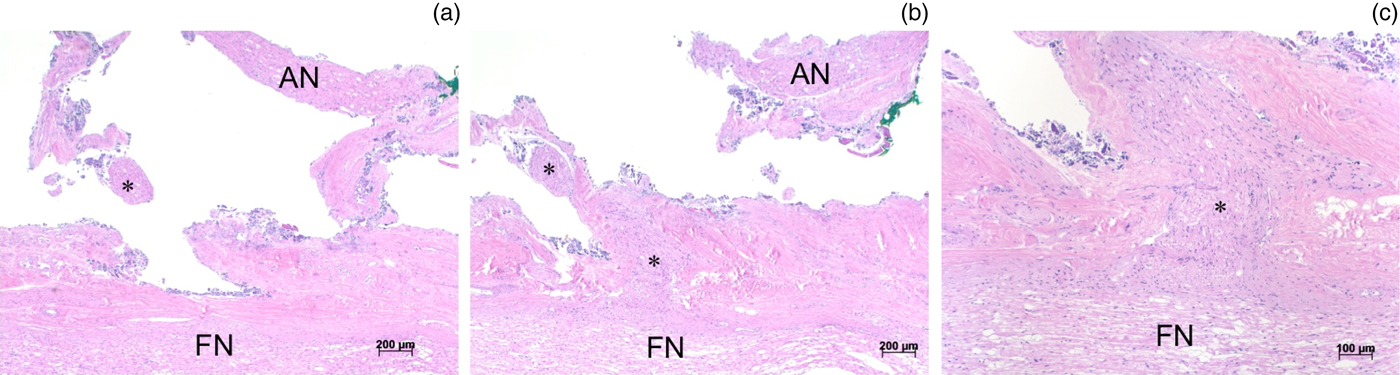
Fig. 4 Histological sections explaining the relations between Arnold's nerve (AN) and the facial nerve (FN). (a–b) Communicating fibres (asterisks) between the facial nerve and Arnold's nerve can be seen (H&E; ×5). (c) Communicating fibres (asterisk) can be seen joining the main trunk of the facial nerve (H&E; ×10).
Discussion
We have highlighted the origin of the sensory nerve to the posterior external auditory canal. It receives nerve fibres from the facial nerve, but is predominantly a continuation of Arnold's nerve, also gathering fibres from the glossopharyngeal nerve.
This nerve is commonly referred to as the ‘sensory branch of the facial nerve to the posterior external auditory canal’; this assumption mostly depends on clinical annotations. James Ramsay Hunt observed an eruption in the posterior aspect of the external auditory canal and pinna in pure herpes zoster oticus cases.Reference Hunt 4 In his paper, in light of previous anatomical descriptions, Ramsay Hunt acknowledged the communicating fibres from Arnold's nerve to the sensory facial nerve branch, but assigned the vesicles on the pinna to herpetic inflammation of the geniculate ganglion associated with facial palsy and auditory symptoms.Reference Hunt 4
Hitselberger noted a sensory deficit in the posterior aspect of the external auditory canal in patients with vestibular schwannomas that compressed the facial nerve (nervus intermedius) in the internal auditory canal (Hitselberger's sign).Reference Hitselberger and House 1 From previous cadaveric dissections, Hitselberger and House attributed their findings entirely to a distinct sensory branch of the facial nerve to the external auditory canal.Reference Hitselberger and House 1
However, the somatic sensory innervation of the external ear canal constitutes multiple neural communications.Reference Grey 2 According to Schuknecht, Arnold described the auricular branch of the vagus in 1831: it begins as a branch of the jugular (superior) ganglion of the vagus nerve, receives some fibres from the petrous (inferior) ganglion of the glossopharyngeal nerve,Reference Schuknecht 5 and then travels over the dome of the jugular bulb. During its ascent, it crosses the mastoid segment of the facial nerve canal with close proximity. To enter the external auditory canal, it goes through the posterior tympanosquamous suture at the midpoint of the posterior bony canal.Reference Grey 2
Schuknecht also described the course of Arnold's nerve in relation to the Fallopian canal, and mentioned a small fibre coming from the facial nerve and innervating the external auditory canal together with Arnold's nerve.Reference Schuknecht 5 According to the anatomist Lang, Arnold's nerve crosses the facial nerve in its mastoid portion approximately 4 mm above the stylomastoid foramen, and connects with the facial nerve by a few fibres.Reference Lang 6
We confirmed that the sensory nerve to the posterior external auditory canal is predominantly a continuation of Arnold's nerve, receiving nerve fibres from the glossopharyngeal nerve and a branch from the main trunk of the facial nerve in the mastoid segment.
From the clinical perspective, it is well known that stimulation of the external auditory canal, especially during aural toilet, often causes reflex coughing or gagging.Reference Grey 2 In these cases, the stimulus travels via Arnold's nerve to the vagal nuclei, which send impulses to the respiratory centre to co-ordinate forced expiration by the phrenic and intercostal nerves.Reference Grey 2 In our clinical case of severe attacks of coughing upon inserting the conventional hearing aid, we attributed this symptom to the Arnold's nerve participation of sensory innervation to the posterior external auditory canal. The symptoms disappeared temporarily upon infiltration of local anaesthesia to the posterior external auditory canal wall, and disappeared permanently following sectioning of the posterior auricular sensory branch.
For otological surgeons, the sensory innervation to the external auditory canal is also important in investigating intractable idiopathic otalgia. Sectioning of this nerve to treat recalcitrant otalgia has already been described.Reference Eshraghi, Buchman and Telischi 7 In our clinical case, immediate pain relief was achieved temporarily with local anaesthesia and permanently with nerve sectioning.
Our experience is that this posterior auricular sensory branch originates distal to the take-off of the chorda, courses a few millimetres superolaterally, and then makes a sharp turn inferiorly, extending towards the bony cartilaginous junction of the inferior external auditory canal (Figure 5). Given the variability of the chorda exiting the facial nerve, the relationship with the posterior auricular sensory branch can also vary, as mentioned by Eshraghi et al., who reported the origin of the sensory branch superior to the chorda tympani.Reference Eshraghi, Buchman and Telischi 7

Fig. 5 Schematic drawing of the posterior auricular sensory branch on a left-sided temporal bone. CT = chorda tympani; FN = facial nerve; IX = glossopharyngeal nerve; X = vagus nerve; JB = jugular bulb; SS = sigmoid sinus
We believe that the sensory branch to the posterior external ear consists of a network of fibres from the IXth, Xth and some fibres from the VIIth cranial nerves. The main part of this nerve comes from Arnold's nerve, with contributory fibres joining from the facial nerve main trunk, as shown in our histological study. As already mentioned by Ramsay Hunt, we postulate variations in the contribution of these different nerves, which explains the differences in symptomatology between individuals.Reference Hunt 4
-
• A distinct nerve innervating the external auditory canal can often be identified in close relation to the facial nerve
-
• This nerve has been attributed to coughing during ear wax removal, neuralgic pain, Hitselberger's sign and vesicular eruptions in Ramsay Hunt's syndrome
-
• This posterior auricular sensory branch is mainly a continuation of Arnold's nerve, receiving fibres from glossopharyngeal and intermedius nerves
The term ‘sensory auricular branch of the facial nerve’ is a misnomer for this nerve, although it may contain some sensory fibres from the intermedius nerve. We prefer the terminology of ‘posterior auricular sensory branch’ for this nerve. Clinicians and surgeons should be aware of this entity and its implications.
Acknowledgement
We acknowledge the help of Dr Katia Dalkowski (kdalkowski@online.de) for her illustration.
Appendix 1 Supplementary video material
A short video demonstrating resection of the sensory branch to the external auditory canal is available online at The Journal of Laryngology & Otology website, at https://doi.org/10.1017/S0022215117000160






