Introduction
The human pinna is a thin, convoluted piece of cartilage covered with perichondrium and skin. These tissues are closely interwoven and receive less humoral circulation. Therefore, any injury or infection takes longer to heal and any oedema or exudate (the frequent outcomes of infection) takes longer to be absorbed. This results in collection of blood and other exudates in a pouch, which subsequently becomes infected to produce an abscess. The infective organisms are usually Pseudomonas aeruginosa or Staphylococcus aureus. Both can cause rapid necrosis of the aural cartilage and may be antibiotic-resistant.
Literature review
Perichondritis and haematoma of the pinna are not lethal; however, if not effectively treated they cause damage to the cartilage, resulting in disfigurement of the pinna – the so-called ‘cauliflower ear’ or ‘wrestler's ear’. This is aesthetically undesirable (although for wrestlers it may be seen as a badge of honour).
Medical treatment alone is almost always a failure. Surgical intervention is required, such as needle aspiration or incision and drainage, along with medical management. To prevent further collections, a tampon, dental roll or plaster mould are usually used along with a pressure bandage. Some authors prefer suturing perichondrium to the cartilage with soft pieces of rubber or Leonard buttons. However, in spite of such efforts, the disease frequently spreads until part or all of the cartilage is destroyed and the pinna deformed.Reference Ho, Jajeh and Molony1 Studies and reviews of the various techniques and methods of treatment have all reported similar results.Reference Jones and Mahendran2
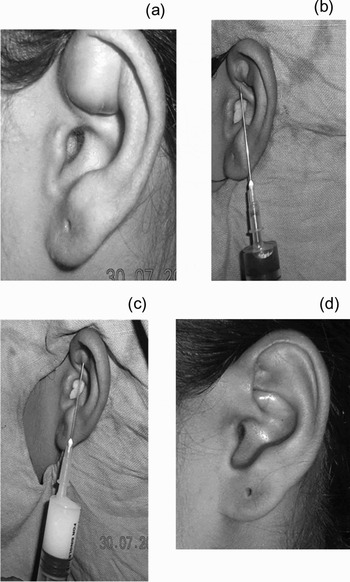
The present study of nine cases presents an alternative, effective treatment which is simple, less painful, leaves no scar or disfigurement, and generates no complications. The technique is indicated in Figures 1, 2 & 3.

Fig. 1 (a) Initial appearance; (b) aspirated material; and appearance on (c) day three, after first aspiration, (d) day five, after second aspiration, (e) day six, after third aspiration (cure complete).

Fig. 2 Another patient: (a) first appearance; (b) appearance after second aspiration.
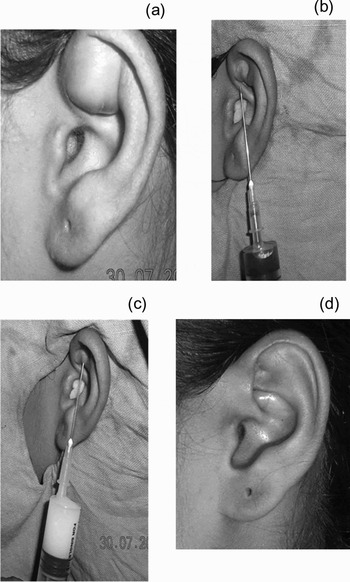
Fig. 3 Another patient: (a) first appearance; (b) first aspiration and aspirated fluid; (c) the injection of medicaments; (d) cured pinna.
This treatment has been practised by the author and his students for the last 20 years. It is now reported, following standardisation of drug doses and technique, and after a literature search to ensure that no such treatment has previously been documented.
Materials and methods
Seven cases of perichondritis of the pinna and two cases of haematoma of the pinna were studied.
Five of the cases were idiopathic and without symptoms. Two cases were due to spread of infection from a congenital intra-auricular sinus. The other two cases resulted from physical trauma.
Procedure
The technique requires the following materials and medicaments: one sterile 2 ml syringe; one 10 ml syringe; one 18 or 20 gauge injection needle; two 22 or 24 gauge injection needles; one vial of 0.5 g intramuscular streptomycin powder; one vial of 1500 IU hyaluronidase powder; one vial of 10 mg/1 ml triamcinolone acetonide; and six 5 ml ampoules of redistilled water.
The patient is seated. The pinna is sterilised and may be draped.
The vial of streptomycin is dissolved in 5 ml of redistilled water taken into the 10 ml syringe with one 22 or 24 gauge needle. Keeping the needle in position in the vial of streptomycin, the syringe is removed. This syringe is then fitted to the 18 or 20 gauge needle, which is then inserted into the swollen region of the pinna. The fluid collection is drained – the needle may need to be manipulated to different positions if the collection has several loculi. Keeping the needle in position in the pinna, the syringe is detached and its contents discarded (Figure 1b). The syringe is washed out with redistilled water. It is then reattached to the needle in the streptomycin vial, and 1 ml of the streptomycin solution is drawn up, which is further diluted to 5 ml with redistilled water (giving a 2 per cent streptomycin solution). The syringe is detached from its needle and reattached to the needle left penetrating the pinna. The perichondritis pouch is then irrigated with the syringe contents, and streptomycin solution washings subsequently aspirated back into the same syringe and discarded. This process (i.e. irrigation with 2 per cent streptomycin solution) is repeated two to three times, until the aspirated fluid becomes clear.
When this is completed, the same amount (5 ml) of 2 per cent streptomycin solution is prepared in the 10 ml syringe. Then, half a vial of triamcinolone (0.5 ml = 5 mg) and half a vial of hyaluronidase (pre-prepared by dissolving its contents in 1 ml redistilled water, using the 2 ml syringe) are drawn up into the same syringe and mixed thoroughly. This solution is injected into the collapsed, drained pinna pouch through the retained needle, until the resulting swelling equals the size of the original collection.
The syringe and needle are then withdrawn, and the puncture point is pressed gently with a sterile ear bud for approximately one minute to prevent leakage.
Further injections are used if healing fails or infection recurs. The duration of healing effect depends on the severity of infection and the extent of the area involved.
Systemic antibiotics and other necessary drugs are continued throughout the course of treatment.
Results
In the nine patients studied, one to four such injection treatments were required at three- to seven-day intervals, as required by the healing process.
The duration of treatment varied with the severity of disease, from five days to one month.
The cosmetic outcome in all cases was excellent – the pinna healed in its normal shape.
Discussion
Previously, most reports of perichondritis or pinna haematoma management have described repeated incision, drainage, suturing and dressing.Reference Macdonald, Calder, Perrett and McGuiness3–Reference Kishore, Prasad, Sridharam, Sampath, Prasad and Hari Mayyappan5
Lack of response to such treatment, and further spread of the disease process, are due to the deficient humoral circulation of the site and to infection by antibiotic-resistant organisms. Humoral insufficiency also hampers effective immunological defence against the infecting bacteria.
The described technique requires only a few injection treatments, and assists the healing process in several ways, as follows.
Firstly, aspiration clears the area of liquids and solids debris (Figure 1b shows the aspirated material in the syringe, in different layers and the figure 3b shows the aspirated haematoma fluid).
Secondly, replacement of infected exudate with an antibiotic solution enhances the drug's bactericidal effect.
Thirdly, streptomycin, although quickly absorbed when injected intramuscularly and excreted within hours, is poorly absorbed by oral or other routes, and thus is retained at the injection site for a prolonged time period, enabling sustained antibacterial action.
Fourthly, hyaluronidase encourages the permeability of humoral factors and enhances resorption of blood, fluid and necrosed products of cartilage infection.
Fifthly, triamcinolone restricts inflammatory and allergic reactions to other drugs, while systemic antibiotics assist the progress of healing.
Lastly, all these factors strengthen immunity, weaken bacteria and assist adherence of perichondrium to cartilage, resulting in rapid healing and prevention of deformity.
Conclusion
The described treatment may be recommended for universal use. The usual treatment (incision and suturing for compression) should be avoided as far as is practicable.