


Introduction
Cochlear implants are widely used, in both children and adults, for the treatment of severe to profound sensorineural hearing loss, with well-established results.Reference Berettini, Baggiani, Bruschini, Cassandro, Cuda and Filipo1 Cochlear implants in general have a favourable outcome and improve quality of life.Reference Berettini, Baggiani, Bruschini, Cassandro, Cuda and Filipo1, Reference Turchetti, Belelli, Palla and Berrettini2 However, some complications have been recognised, including facial nerve palsy, wound infection, flap necrosis and electrode displacement.Reference Cohen and Hofman3, Reference Terry, Kelt and Jeyakumar4
An uncommon but increasingly encountered complication is the migration or dislocation of the cochlear implant magnet resulting from a magnetic resonance imaging (MRI) scan,Reference Hassepass, Stabenau, Arndt, Beck, Bulla and Grauvogel5, Reference Özgür, Dursun, Çeliker and Terzi6 which necessitates surgery for repositioning. This magnet migration or dislocation can occur despite meticulous head bandaging as recommended by the manufacturers and other authors.Reference Cohen and Hofman3–Reference Hassepass, Stabenau, Arndt, Beck, Bulla and Grauvogel5
We present a case of cochlear implant magnet dislocation despite head bandaging, and demonstrate that the use of an endoscope in the relocation of the cochlear implant magnet is a feasible and viable minimally invasive option.
Case report
A 67-year-old male with right-sided profound sensorineural hearing loss underwent right cochlear implantation in 2015 (using a HiRes 90 K Advantage cochlear implant, with the HiFocus Mid-Scala Electrode; Advanced Bionics, Valencia, California, USA). The cochlear implant was activated 14 days post-operatively, and the patient had near-normal hearing thresholds and good speech recognition 3 months later.
Nine months following cochlear implantation, the patient required an MRI scan of his spine for suspected cervical and lumbar radiculopathy. As per the manufacturer guidelines, the magnet was not removed, but a tight head dressing was applied for the scan. A 1.5 Tesla MRI scan was performed (using a Philips Ingenia 1.5 Tesla system) without initial complications; however, the patient experienced a sharp pain over the implant site during the MRI. He presented to the clinic shortly afterwards with discomfort and a bulge over his scalp at the magnet site.
Stenver's and lateral view skull radiographs were performed (Figure 1). The magnet was observed to be dislocated from its slot in the receiver stimulator.

Fig. 1. (a & b) Skull X-rays showing the magnet's dislocation. R = right
Instead of the U-shaped skin flap that is often used in surgery carried out to resolve such issues, an endoscopic minimally invasive approach was employed (Figure 2). Initially, a dummy processor was used to mark the position of the magnet and coil. A 2 cm skin incision was made posterosuperior to the receiver stimulator to avoid damaging the coil, and deepened to the subperiosteal layer. The periosteum was elevated, and a 0-degree endoscope was advanced and used to identify the dislodged magnet (Figure 3). The magnet was twisted and lifted, but was still partially in the inner coil's retaining pocket. There was no evidence of infection.

Fig. 2. Operating theatre set-up (Dr HW Yuen on the left).

Fig. 3. Endoscopic image of the dislocated magnet.
Under endoscopic guidance, the magnet was repositioned into its housing slot and its placement was checked (Figure 4). The polarity and functioning of the magnet was checked with a dummy processor. The wound was closed in layers. A mastoid compression bandage was then applied.
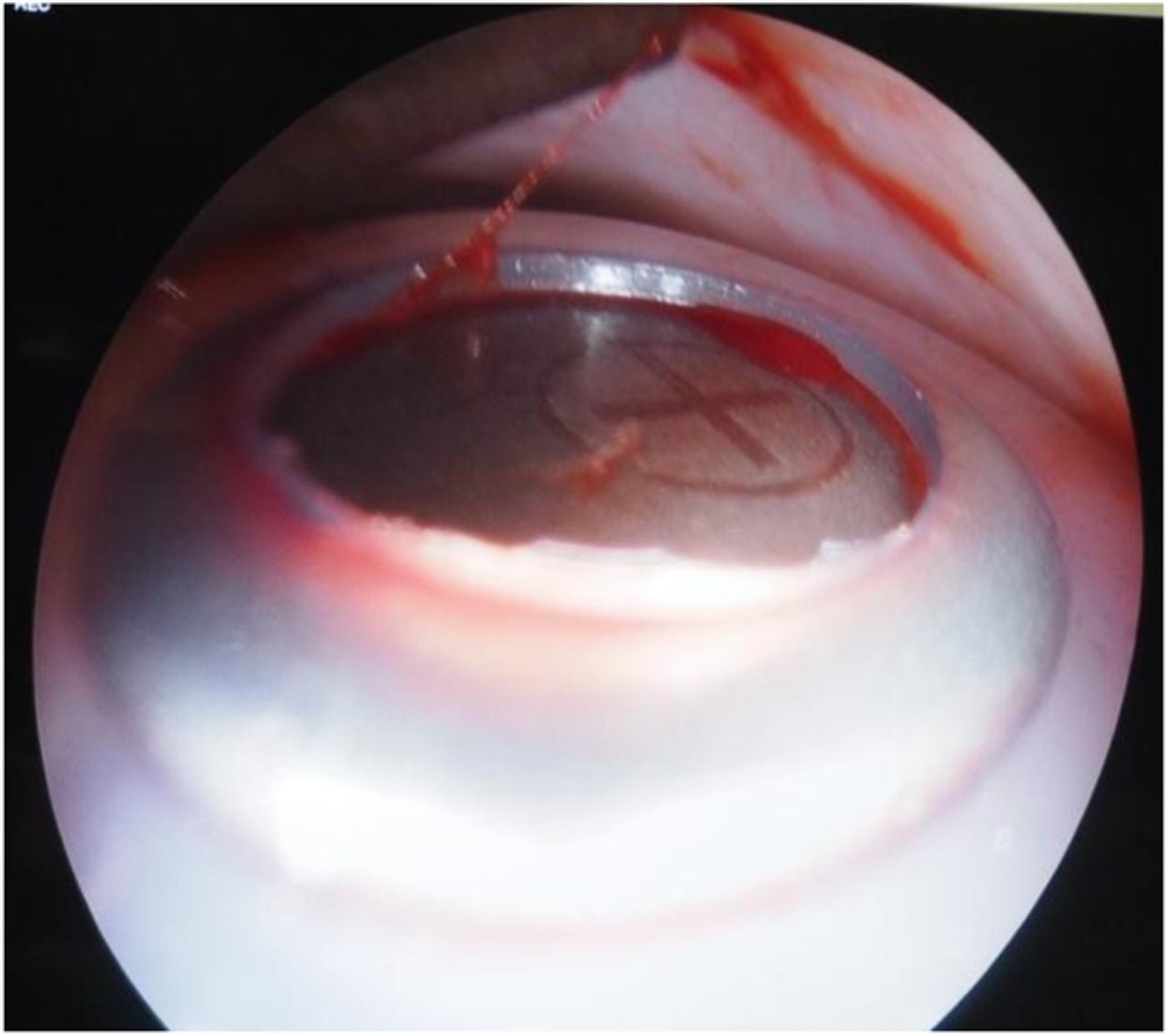
Fig. 4. Endoscopic image of the repositioned magnet.
The wound was well healed after one week and the skin sutures were removed. The speech processor was then turned on again without problems.
Discussion
An uncommon but serious complication of cochlear implants with a removable magnet is magnet dislocation caused by an MRI scan or, less commonly, direct trauma.Reference Hassepass, Stabenau, Arndt, Beck, Bulla and Grauvogel5 Magnetic resonance imaging is increasingly used in the diagnosis and management of many conditions. Early generations of cochlear implants required explantation and were not MRI-compatible. To minimise this complication, various authors and manufacturers have proposed recommendations involving tight head dressings, to avoid magnet explantation in suitable cochlear implant recipients undergoing 1.5 Tesla MRI scans. However, guidelines on MRI safety for patients with cochlear implants vary across the world, as a review by Azadarmaki et al. concludes.Reference Azadarmaki, Tubbs, Chen and Shellock7
Repositioning, and similarly explantation, of the cochlear implant magnet has generally entailed open exposure of the implant site. This increases the risk of microbiological contamination of the device, with possible extension to the meningeal layer. As described by multiple authors, the technique for repositioning the magnet involves an incision just superior to the receiver unit and dissection through the subcutaneous layers. The fibrous capsule is then opened, achieving direct visualisation and exposure of the magnet and inner coil. The skin and subcutaneous layers are then closed.Reference Hassepass, Stabenau, Arndt, Beck, Bulla and Grauvogel5, Reference Özgür, Dursun, Çeliker and Terzi6, Reference Cuda, Murri and Succo8
In any implant surgery, there are always concerns regarding infection, and skin or flap problems. Ray et al. examined cochlear implant explantation, revision and re-implantation surgery, and reported that wound and flap problems were more common with larger incisions.Reference Ray, Proops, Donaldson, Fielden and Cooper9 Minimising the exposure may reduce such problems. Di Nardo et al. described a case of manual external repositioning in a patient.Reference Di Nardo, Giannantonio, Schinaia, De Corso and Pauludetti10
Rigid endoscopes have been used by otolaryngologists for more than 30 years, and can be easily found in many specialist centres. Their use in the layers of the scalp and face, and within the temporal region, is well described.Reference Hu, Ma, Xue, Qi and Chen11 Orhan et al. reported on endoscopic-assisted cochlear implantation.Reference Orhan, Polat, Çelik, Çomoğlu and Güldiken12 We found that the use of an endoscope (i.e. Olympus Visera 4 K UHD System) enabled a smaller incision, further from the receiver, but with good visualisation of the inner coil and magnet. Extensive subcutaneous dissection was not required and the breach in the fibrous pocket was kept to a minimum.
Some potential benefits of this endoscope-assisted method include a reduced incision size, less compromise to the skin near the inner coil and minimal external exposure of the implant. In the modern context, a reduced need to shave hair, a smaller scar and a potentially faster return to aided hearing may have a positive impact on patient satisfaction and quality of life. There would, however, be situations where an endoscopic approach is arguably less feasible, such as in cochlear implant patients with distant magnet migration or revision cochlear implant cases. The logistics and potentially limited availability of rigid endoscopes may also be an inconvenience compared to the simplicity of an open procedure.
• Magnet dislocation due to magnetic resonance imaging is uncommon but serious in patients with a cochlear implant with a removable magnet
• This complication usually requires surgery for repositioning, mainly via a direct open approach
• This paper describes the first case of an endoscope successfully used to reposition the magnet, via a small incision away from the implant
• The cochlear implant resumed normal function and there were no post-operative complications
• Possible benefits include a smaller incision, less implant exposure, less compromise to overlying tissue and skin, and improved patient satisfaction
Conclusion
Cochlear implant magnet dislocation is an uncommon but increasingly reported complication of MRI scans. This can occur despite meticulous head bandaging according to recommendations, necessitating surgery for repositioning. Cochlear implant recipients must be made aware of this potential risk. To the best of our knowledge, this is the first description of cochlear implant magnet relocation performed with endoscopic assistance. It is a safe, quick and viable option for the relocation of a dislodged cochlear implant magnet in some situations.
Competing interests
None declared




